Erythema Migrans — The Lyme Rash Guide
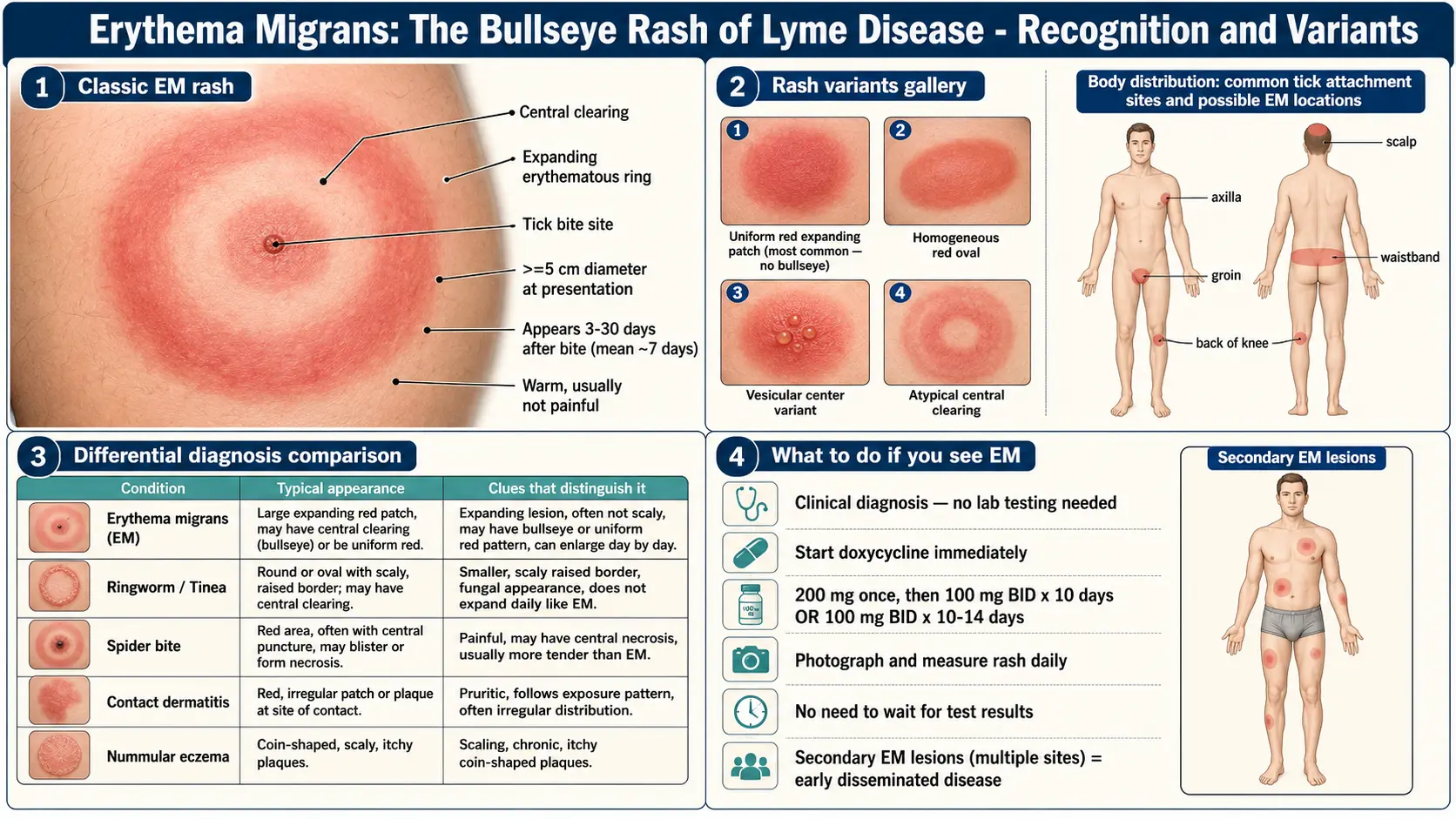
Table of Contents
- What EM Is — and Why It Matters Most
- Classic Bullseye vs. Atypical Forms
- Timing — When It Appears and How Fast It Grows
- What It Feels Like
- Where It Appears — the "Missed Rash" Problem
- How to Photograph It
- Look-Alikes You Should Know
- Multiple EM Lesions — Early Disseminated Disease
- Why the Rash Alone Is Enough to Treat
- When to Skip Testing and Just Treat
- What Happens If EM Is Missed
- Photograph and Go — Scripts for Urgent Care
- After You Start Antibiotics
- Key Research Papers
- Connections
- Featured Videos
What EM Is — and Why It Matters Most
Erythema migrans (EM) is the expanding skin rash that appears at the site of a Borrelia burgdorferi tick bite. It is the single most important physical sign of early Lyme disease. About 70–80% of people with confirmed Lyme develop a recognizable EM in the first month. If you see one, you essentially have a confirmed diagnosis — no blood test required.
This matters because Lyme is one of those rare infections where a patient can catch their own diagnosis early. A rash you notice on Tuesday and show to a clinician on Thursday can be cured with two to three weeks of oral doxycycline. The same infection left to "see if it goes away" can smolder into Lyme arthritis, carditis, facial palsy, or neuroborreliosis weeks later.
The rash is caused by the bacteria migrating outward through the skin from the bite site. As spirochetes spread radially through the dermis, the immune system follows, creating an expanding ring of inflammation. That is literally what erythema migrans means: "migrating redness."
Classic Bullseye vs. Atypical Forms
Everybody has seen the stock photo — a round red ring with a pale center and a dark dot in the middle. That classic bullseye is diagnostic when you see it, but it is not the most common form.
In the largest U.S. cohort studies, the bullseye appears in only about 20–40% of EMs. The remaining 60–80% are atypical and get dismissed as "just a bite" every day:
- Solid / homogeneous red oval. The most common atypical form. A uniform pink-to-red patch, often oval rather than round, with no central clearing. Looks like a flat, painless bruise that happens to be red instead of purple.
- Uniform red plaque. Slightly raised, smooth, warm but not hot. Easy to mistake for a mild allergic reaction.
- Bluish or purplish hue. Common on darker skin tones, where the classic "red ring" descriptions fail completely. EM on Black and brown skin frequently looks bruise-like or violaceous rather than bright red — and is under-diagnosed for exactly that reason.
- Central vesicle or crust. A small blister or scab at the bite point inside an expanding red area. Often mistaken for a spider bite.
- Multiple concentric rings. Less common but essentially pathognomonic — almost no other rash makes two or three concentric rings.
- Multiple EM lesions. Several separate red patches scattered on trunk, limbs, and face, each one representing a site where bacteria seeded through the bloodstream. See the disseminated section below.
The practical rule: any expanding red patch larger than 5 cm (2 inches) that appears within a month of possible tick exposure should be treated as EM until proven otherwise. Size and growth matter more than shape.
Timing — When It Appears and How Fast It Grows
EM typically appears 3 to 30 days after the tick bite, with a median of about 7 days. A rash within hours is almost certainly not EM — that is an irritant reaction to tick saliva, which is harmless. Real EM takes days to develop.
Once it starts, EM expands roughly 1–2 cm per day. That outward march is one of the most useful diagnostic features. Spider bites, allergic reactions, and contact dermatitis all peak within 24–48 hours and then shrink. EM keeps getting bigger, often reaching 15 cm or more by the time it is noticed.
Many people never saw the tick. Nymphal deer ticks — the primary U.S. vector — are the size of a poppy seed; they attach for 24–72 hours, feed, drop off, and leave no trace. Not remembering a bite does not rule out Lyme.
What It Feels Like
This is where EM surprises almost everyone. It usually does not itch and does not hurt. At most, people describe a mild warmth, a vague tingling, or a feeling that "something is there." Many discover their rash only because a partner notices it on their back, or they see it in the mirror while changing clothes.
That painless, itchless quality is diagnostically important because it separates EM from its top look-alikes:
- Spider bite: painful, often throbbing, sometimes with a necrotic (blackened) center.
- Cellulitis: hot, tender, tight-feeling, with ill-defined borders that blur into surrounding skin.
- Allergic or contact dermatitis: itchy, sometimes burning.
- Ringworm: mildly itchy, scaly, with a raised and flaking leading edge.
When a painless expanding red ring shows up on someone who was hiking, gardening, or playing in grass a week earlier, the clinical picture is already about 80% of the way to a Lyme diagnosis.
Many patients also feel a mild flu-like illness — low-grade fever, fatigue, headache, muscle aches, swollen lymph nodes near the bite. Systemic symptoms without a respiratory component ("summer flu" with no cough) are another strong Lyme clue.
Where It Appears — the "Missed Rash" Problem
Ticks climb. They prefer warm, moist, tucked-away skin where they can feed undisturbed. That means EM overwhelmingly shows up in places you cannot easily see:
- Popliteal fossa — the back of the knee.
- Groin and inner thigh.
- Axilla — the armpit.
- Back, especially between the shoulder blades and along the waistband.
- Scalp and hairline, where hair hides both tick and rash.
- Buttocks and gluteal fold.
- Behind the ears and the nape of the neck.
This is the "missed rash" problem. A real minority of EMs — perhaps 20–30% — never get noticed because they sit somewhere the patient cannot see or fade before anyone looks. If you have been in a tick-exposed area and feel flu-like without respiratory symptoms, have someone check your scalp, back, buttocks, and the backs of your knees. A 30-second inspection can change everything.
How to Photograph It
Your phone camera is one of the most powerful diagnostic tools available to a patient. A well-documented series can convince a skeptical clinician to treat in five minutes:
- Photograph daily. Same spot, once per day. The point is to document expansion over time.
- Include a scale reference. Place a ruler, a coin (quarter = 24 mm, dime = 18 mm), or a credit card (85 mm long) next to the rash. Without scale, a clinician cannot judge size from a photo.
- Mark the border with a pen. Trace the outer edge today. Tomorrow, if the rash has expanded past the pen line, you have documented growth — which is diagnostic.
- Use flat natural light. Daylight near a window gives the truest color; phone flash distorts red tones.
- Take a wide shot and a close-up. Wide for body location; close-up for texture and border detail.
- Photograph any tick you find on a white background with a coin for scale. Many state health departments identify species for free.
Three daily photos showing measurable outward expansion is essentially ironclad evidence of EM. Bring them to the appointment.
Look-Alikes You Should Know
A rash that fools people into missing Lyme is a bigger problem than a rash that triggers unnecessary antibiotics, so knowing the look-alikes helps you argue both directions:
- Spider bite (especially brown recluse). Painful from the start, often with a dark necrotic center and a surrounding pale ring. Rarely exceeds 3–4 cm. Most "spider bites" diagnosed in U.S. emergency rooms turn out to be something else — EM is one of the most commonly mislabeled.
- Cellulitis. Hot, tender, rapidly advancing (hours, not days), with poorly defined margins. Often accompanied by fever. Responds to cephalexin — which does not cover Borrelia. See Cellulitis.
- Ringworm (tinea corporis). Scaly, flaking leading edge and clearer, drier center. Mildly itchy. Expands over weeks, not days. The scale is the giveaway; EM is smooth.
- Nummular eczema. Coin-shaped itchy, dry, scaling plaques, often multiple. No central bite mark.
- Granuloma annulare. Firm, ring-shaped, skin-colored-to-red plaque that can look remarkably bullseye-like. Painless, very slow growing, and notably smaller than EM.
- Fixed drug eruption. A single round red-brown patch that recurs in the same spot each time the patient takes the causative drug.
- STARI (Southern Tick-Associated Rash Illness). An EM-identical rash caused by the bite of the lone star tick (Amblyomma americanum) in the southeastern United States. Clinically indistinguishable from EM; the CDC recommends treating as Lyme because you cannot tell them apart at the bedside.
Multiple EM Lesions — Early Disseminated Disease
If you see several EM patches scattered across the body — one on the back, one on the thigh, one on the arm — you are looking at early disseminated Lyme disease. The first (primary) lesion forms at the bite. Within days to a few weeks, spirochetes enter the bloodstream and seed the skin at multiple distant sites, each of which blooms into its own smaller EM.
Multiple EMs occur in roughly 10–20% of U.S. Lyme cases. They mean the infection is past the local-skin stage and justify a slightly longer oral-antibiotic course (see Antibiotic Treatment Protocols). Neurologic symptoms, facial palsy, heart-rhythm changes, and arthritis are all more likely if treatment is delayed past this stage.
Why the Rash Alone Is Enough to Treat
The 2020 IDSA/AAN/ACR Lyme guidelines (Lantos et al.) state plainly: a characteristic EM in a person with plausible tick exposure is a clinical diagnosis of Lyme disease, and serologic testing is not required before starting antibiotics.
Two reasons. First, EM is specific — few other conditions produce a painless, expanding, large red ring at a possible tick-bite site. Second, blood tests at this stage are unreliable: the two-tier serology (ELISA + Western blot) needs 2–6 weeks for detectable antibodies and is negative in 60–70% of true Lyme cases in the first week. A negative result during the rash stage only tells you that you tested too early.
Correct sequence: see the rash, start antibiotics, worry about testing later (or not at all). See Lyme Testing Explained.
When to Skip Testing and Just Treat
Skip the blood work and go straight to antibiotics when all of the following apply:
- An expanding red lesion that is at least 5 cm across (classic or atypical).
- Plausible tick exposure in the prior 3–30 days — hiking, yard work, camping, living in or visiting a Lyme-endemic area (most of the northeastern and upper-midwestern United States, parts of northern California, and much of Europe).
- No better alternative explanation (no prescription sulfa drug just started, no history of tinea, no painful necrotic center suggesting spider bite or staph).
In that situation, first-line treatment is oral doxycycline 100 mg twice daily for 10–14 days in adults and children over 8 years. Alternatives exist for pregnant women, young children, and doxycycline-intolerant patients (amoxicillin, cefuroxime). See Antibiotic Treatment Protocols for the full dosing table.
Testing does help later — weeks or months after the rash, when arthritis, cardiac, or neurologic symptoms suggest later-stage Lyme. But at the EM stage, testing usually just slows you down.
What Happens If EM Is Missed
An untreated EM usually fades within 3–4 weeks. That is misleading comfort — the rash fades because the bacteria have moved deeper, not because they are gone. Untreated early Lyme progresses predictably:
- Days to weeks later — early disseminated disease. Multiple secondary EMs, facial-nerve palsy (often called Bell's palsy when the cause is not recognized), meningitis-like headache and stiff neck, heart-block and other cardiac arrhythmias ("Lyme carditis"), migrating joint pains.
- Weeks to months later — late disseminated disease. Large-joint arthritis, most classically of the knee, with dramatic swelling and little pain. See Arthritis.
- Months to years — chronic sequelae. Neuroborreliosis (nerve-root pain, neuropathy, encephalopathy, cognitive fog), chronic inflammatory arthritis, and in a minority of treated patients, the controversial syndrome of post-treatment persistent symptoms. See PTLDS and Chronic Lyme.
Every one of these outcomes is dramatically less likely if the EM is recognized and treated within a few days of appearing. That is the entire argument for taking this rash seriously.
Photograph and Go — Scripts for Urgent Care
Same-day urgent care or a same-week primary-care visit is the usual path. Most clinicians will treat on the spot once they see good documentation; a minority push back, want to "watch and wait," or insist on confirmatory blood tests before prescribing. You have good arguments ready.
If the clinician wants to wait for serology:
"I understand, but the 2020 IDSA–AAN–ACR Lyme guidelines specifically say that serology is not required before treating an erythema migrans rash, because the two-tier test is 60–70% negative in the first week. I have daily photos showing the rash expanding over three days. I'd rather start doxycycline today than wait two more weeks for a test that can't rule it out."
If they say it looks like a spider bite:
"It doesn't hurt and there's no necrotic center. I took this photo three days ago and it has grown 4 cm since then. Spider bites peak at 48 hours and shrink. Can we treat this as presumed EM and reassess in two weeks?"
If they say you are in a non-endemic area:
"I was in [endemic area] [N] days ago. The incubation for Lyme is up to 30 days. Even if local transmission is rare, travel exposure would explain this."
If they say you tested negative:
"A negative test in week one is expected — antibodies take 2–6 weeks. The CDC and IDSA both say a characteristic EM is a clinical diagnosis and treatment should not wait for serology."
If push-back continues, ask for the refusal to be documented in the chart ("patient refused doxycycline trial for suspected EM"). That single request usually ends the argument. Otherwise try another urgent care or a telemedicine service — many will prescribe doxycycline for EM with a photo. The downside of a 14-day course in a healthy adult is trivial compared to untreated disseminated Lyme.
After You Start Antibiotics
Expect a gradual fade. The rash does not vanish overnight. Typical timeline once doxycycline is on board:
- Days 1–3. Some patients feel briefly worse for 24–48 hours — chills, headache, muscle aches, a flare of the rash. This is a Jarisch–Herxheimer reaction, the immune response to dying spirochetes dumping their contents. It is self-limited. Ibuprofen and rest are enough. Do not stop the antibiotic.
- Days 3–7. The rash stops expanding. The central area pales first. Borders begin to blur.
- Week 2. Redness fades substantially. A faint brownish discoloration (post-inflammatory hyperpigmentation) often remains.
- Weeks 3–8. The discoloration slowly resolves. A very faint oval shadow may persist for months but is cosmetic only.
Finish the full course even if the rash is gone by day 5. Stopping early is the single biggest cause of under-treated Lyme. If new symptoms appear during or after treatment — facial droop, knee swelling, heart palpitations, severe headache — call your clinician the same day. The rash resolving is not the same as the infection resolving, and a second-line regimen (IV ceftriaxone) exists for the rare cases where oral therapy is insufficient.
Practical support: take doxycycline with a full glass of water and stay upright for 30 minutes (prevents pill-induced esophagitis); avoid direct sun or use high-SPF sunscreen; and do not take it within two hours of dairy, iron, calcium, antacids, or magnesium, which block absorption. Supportive herbs such as Cat's Claw can be used alongside — never instead of — antibiotics.
Key Research Papers
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. Clinical Practice Guidelines by the IDSA, AAN, and ACR: 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1–e48.
- Shapiro ED. Clinical practice: Lyme disease. N Engl J Med. 2014;370(18):1724–1731.
- Feder HM Jr, Johnson BJB, O'Connell S, et al. A Critical Appraisal of "Chronic Lyme Disease." N Engl J Med. 2007;357(14):1422–1430.
- Smith RP, Schoen RT, Rahn DW, et al. Clinical Characteristics and Treatment Outcome of Early Lyme Disease in Patients with Microbiologically Confirmed Erythema Migrans. Ann Intern Med. 2002;136(6):421–428. (image atlas of classic and atypical EM).
Live PubMed Searches
For deeper reading, the following PubMed topic searches return current peer-reviewed work on EM recognition, differential diagnosis, and early Lyme management:
- Erythema migrans and Lyme disease diagnosis
- Atypical erythema migrans presentations
- STARI vs. erythema migrans
- Erythema migrans on skin of color
- Multiple erythema migrans and early disseminated Lyme
- Doxycycline duration in early Lyme disease
- Serology sensitivity in early Lyme infection
- Jarisch–Herxheimer reaction in Lyme treatment
Connections
- Infectious Disease
- Antibiotic Treatment Protocols
- PTLDS and Chronic Lyme
- Lyme Testing Explained
- Arthritis
- Cellulitis
- Lyme Neuroborreliosis
- Cat's Claw
- Lyme Disease Overview
- Prevention and Tick Removal
- Tick Bite First Aid
- Tick-Borne Co-Infections
- Alpha-Gal Syndrome
- Chronic Pain
- Headache
- Lyme Carditis
- Fatigue