Antibiotic Treatment Protocols for Lyme Disease
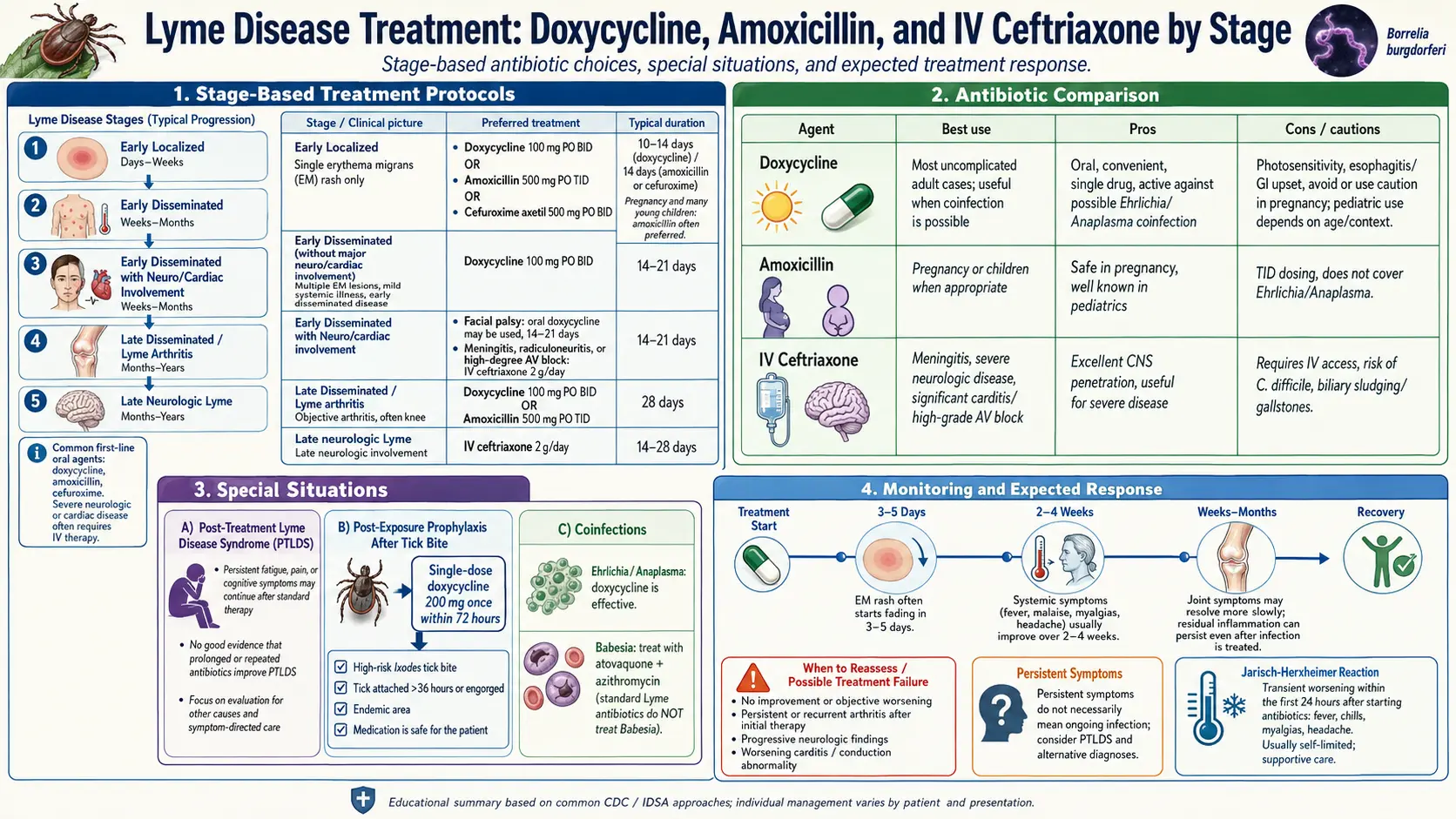
Table of Contents
- The Core Principle — Right Dose, Right Duration
- Early Localized Lyme (Single EM Rash)
- Early Disseminated Lyme (No CNS)
- Lyme Carditis
- Lyme Arthritis
- Lyme Neuroborreliosis
- Pediatric Dosing
- Pregnancy and Breastfeeding
- Jarisch-Herxheimer Reaction
- IV vs. Oral — When Each Is Needed
- Why Longer Courses Don't Help
- Re-Treatment After a First Course
- Drug Interactions and Side Effects
- If Symptoms Persist After Treatment
- Key Research Papers
- Connections
- Featured Videos
The Core Principle — Right Dose, Right Duration
Lyme disease is caused by the spirochete bacterium Borrelia burgdorferi (plus a small number of related species in Europe and Asia). It is a bacterium, which means antibiotics work — reliably, measurably, and usually quickly. Roughly 90% of patients treated in the early localized stage are cured with a single oral course, and even late-stage manifestations like Lyme arthritis respond to standard regimens in the large majority of cases.
Two principles guide every protocol on this page:
- The right drug at the right dose for the right duration works. Underdosing (skipping doses, stopping early, using suboptimal drugs) leaves residual infection.
- Longer is not better. Four major randomized controlled trials have tested multi-month antibiotics against placebo in patients with persistent symptoms. None showed durable benefit; all showed significant harm (line infections, C. difficile, candidiasis, drug reactions). Stretching a two-week course into six months does not kill more bacteria — it just accumulates complications.
Everything below follows the 2020 IDSA/AAN/ACR joint guidelines, the current U.S. standard of care. Where European practice differs (notably for neuroborreliosis), we note it.
Early Localized Lyme (Single EM Rash)
Early localized disease means a single erythema migrans (EM) rash, usually within 30 days of a tick bite, with or without mild constitutional symptoms (low-grade fever, fatigue, headache, mild myalgia). No neurologic, cardiac, or joint involvement. First-line oral options in adults:
- Doxycycline 100 mg PO twice daily × 10 days. The preferred agent in non-pregnant adults and children ≥8 years. It has the added advantage of covering Anaplasma phagocytophilum and Ehrlichia, the two most common tick-borne co-infections transmitted by the same Ixodes ticks. A 10-day course is the current IDSA 2020 recommendation — shortened from the older 14-to-21-day courses after RCTs showed equivalent efficacy.
- Amoxicillin 500 mg PO three times daily × 14 days. The default for pregnant or breastfeeding patients and children under 8 who cannot receive doxycycline. Slightly longer course because amoxicillin does not achieve the intracellular concentrations doxycycline does.
- Cefuroxime axetil 500 mg PO twice daily × 14 days. Reserved for patients who cannot tolerate doxycycline or amoxicillin (penicillin allergy short of anaphylaxis, doxycycline GI intolerance).
- Azithromycin 500 mg PO once daily × 7 days. Only when all three above are contraindicated. Clinical cure rates are 5–10 percentage points lower than doxycycline or amoxicillin, so it is a third-line drug, not a convenience choice.
The EM rash typically fades within days of starting antibiotics. Fatigue and myalgia may take 2–4 weeks to resolve fully even after the bacteria are gone — normal post-infectious recovery, not treatment failure.
Early Disseminated Lyme (No CNS)
Early disseminated Lyme means the spirochetes have spread beyond the tick-bite site but without meningitis or encephalitis. Typical presentations:
- Multiple EM lesions (several secondary rashes elsewhere on the body).
- Cranial nerve palsy — most commonly isolated facial nerve (CN VII) palsy, unilateral or bilateral, without headache/stiff neck/meningeal signs.
- Lyme carditis without high-grade AV block (see the next section).
- Radiculoneuropathy — shooting pain in a dermatomal distribution.
Treatment is the same oral regimens as early localized disease, extended to 14–21 days. Doxycycline 100 mg BID, amoxicillin 500 mg TID, or cefuroxime axetil 500 mg BID. Isolated facial palsy in particular — which was once routinely treated with IV ceftriaxone — is now clearly an oral-antibiotic condition based on multiple European RCTs showing equivalent outcomes.
Lyme Carditis
Lyme carditis is uncommon (about 1% of untreated cases) but matters because it can cause sudden high-grade AV block, syncope, and — rarely — death. The cornerstone of management is the PR interval on ECG:
- First-degree AV block with PR < 300 ms, asymptomatic, hemodynamically stable: outpatient oral doxycycline 100 mg BID × 14–21 days. Repeat ECG in 48–72 hours to confirm the interval is narrowing. No hospitalization needed.
- PR ≥ 300 ms, or any second- or third-degree AV block, or symptomatic (syncope, dyspnea, chest pain): hospitalize with continuous telemetry. Start IV ceftriaxone 2 g daily. Transition to oral doxycycline once the block has resolved (usually 3–7 days) to complete a total 14–21-day course.
Temporary pacing may be required for high-grade block. Permanent pacemakers are almost never needed — Lyme carditis is reversible with antibiotics. If a patient receives a permanent pacemaker for what later turns out to be Lyme carditis, it was almost always an unnecessary procedure.
Lyme Arthritis
Lyme arthritis is typically a monoarthritis or oligoarthritis of large joints, most often one knee, appearing weeks to months after infection. The joint is swollen, warm, and stiff but often surprisingly less painful than you would expect from the size of the effusion.
Standard first course: doxycycline 100 mg PO twice daily × 28 days. Amoxicillin 500 mg TID × 28 days is an alternative.
About 80–90% of patients resolve completely with this single oral course. The remaining 10–20% have persistent synovitis at the 2-month mark. For them:
- Second course: a repeat 28 days of oral doxycycline or a 2–4 week course of IV ceftriaxone 2 g daily. IDSA 2020 considers these roughly equivalent; oral is cheaper and avoids line complications.
- Post-antibiotic Lyme arthritis. A subset of patients — often HLA-DR4-positive — have persistent synovitis even after two full courses. By that point, live bacteria are rarely recoverable from the joint; the inflammation is immune-driven, not infection-driven. Management shifts to a rheumatologist and DMARDs (methotrexate, hydroxychloroquine) or intra-articular steroids. More antibiotics do not help and should be stopped.
Lyme Neuroborreliosis
Neuroborreliosis encompasses meningitis, encephalitis, encephalomyelitis, cranial neuropathies, and radiculoneuropathy. Diagnosis requires CSF analysis (pleocytosis, elevated protein, intrathecal antibody production).
- Meningitis or encephalomyelitis with CNS parenchymal involvement: IV ceftriaxone 2 g daily × 14–21 days. Penicillin G 18–24 million units daily IV and cefotaxime 2 g IV every 8 hours are acceptable alternatives.
- Isolated cranial neuropathy (e.g., facial palsy) or radiculoneuropathy without meningeal signs: oral doxycycline 100 mg BID × 14–21 days. This is the major 2020 IDSA/AAN/ACR change: based on European RCTs (Ljostad et al. and others) showing oral doxycycline non-inferior to IV ceftriaxone for most neuroborreliosis, the IDSA now endorses oral as first-line unless parenchymal CNS disease is present.
Patients often ask whether IV is "stronger." It isn't. Doxycycline achieves excellent CSF penetration; ceftriaxone's only real advantage is that you cannot miss a dose while an infusion is running.
Pediatric Dosing
The 2020 IDSA guidelines made an important change: doxycycline is now considered safe for short courses (≤21 days) in children under 8 years. Older concerns about permanent tooth staining came from long-course tetracycline use in the 1960s and do not appear to apply to short doxycycline courses. CDC data specifically support this for Rocky Mountain spotted fever and, by extension, for tick-borne diseases generally.
- Doxycycline: 4.4 mg/kg/day PO divided twice daily, maximum 100 mg per dose. All ages.
- Amoxicillin: 50 mg/kg/day PO divided three times daily, maximum 500 mg per dose.
- Cefuroxime axetil: 30 mg/kg/day PO divided twice daily, maximum 500 mg per dose.
- IV ceftriaxone (for carditis with high-grade block or CNS disease): 50–75 mg/kg once daily, maximum 2 g.
Pregnancy and Breastfeeding
Doxycycline is contraindicated in pregnancy (second and third trimester — risk of fetal tooth discoloration and bone growth inhibition) and avoided while breastfeeding, though brief exposure is likely low-risk. Preferred agents:
- Amoxicillin 500 mg PO three times daily × 14–21 days (first-line in pregnancy for any stage except CNS/high-grade carditis).
- Cefuroxime axetil 500 mg PO twice daily × 14–21 days if penicillin-allergic.
- IV ceftriaxone 2 g daily for neuroborreliosis or high-grade carditis, same as non-pregnant adults.
Treated Lyme disease in pregnancy has an excellent fetal outcome record. Untreated Lyme in pregnancy has rare reports of adverse outcomes, which is why prompt treatment matters more than agent choice.
Jarisch-Herxheimer Reaction
In roughly 15% of patients, the first 24 hours of antibiotic treatment produce a transient worsening known as the Jarisch-Herxheimer reaction: fever, chills, headache, muscle aches, sometimes a rash flare. It is caused by a burst of bacterial lipoproteins released as the spirochetes die, triggering the innate immune system.
Key points for patients:
- It is not a drug allergy. Do not stop the antibiotic.
- It peaks within 24 hours and resolves within 48.
- Supportive care works: hydration, acetaminophen or ibuprofen for fever and aches, rest.
- True allergic reactions (hives, facial/lip swelling, wheezing, anaphylaxis) are different and do require stopping the drug and calling the prescriber immediately.
IV vs. Oral — When Each Is Needed
There is widespread patient belief that IV antibiotics are categorically stronger than oral. For most of Lyme disease, this is wrong. Doxycycline, amoxicillin, and cefuroxime axetil all reach therapeutic tissue levels that kill Borrelia effectively. IV therapy adds three things and three things only:
- Guaranteed adherence (an infusion pump cannot skip doses).
- Higher peak CSF concentrations of some agents (useful in parenchymal CNS disease).
- Management of patients who cannot absorb oral drugs (severe vomiting, gut disease).
Reserve IV for: meningitis with parenchymal CNS involvement, high-grade AV block (PR ≥300 ms or worse), refractory Lyme arthritis after two oral courses, and patients who truly cannot take oral medication. Everything else is an oral-antibiotic condition. Indwelling central lines for months of IV antibiotics in Lyme have caused deaths from line sepsis and are never indicated.
Why Longer Courses Don't Help
Four large randomized controlled trials have tested multi-month antibiotics against placebo in patients with persistent symptoms after standard treatment:
- Klempner et al. (2001, NEJM) — 30 days IV ceftriaxone followed by 60 days oral doxycycline vs. placebo. No benefit.
- Krupp et al. (2003) — 28 days IV ceftriaxone vs. placebo for post-Lyme fatigue. Mild transient fatigue benefit; no durable improvement in cognition or quality of life.
- Fallon et al. (2008) — 10 weeks IV ceftriaxone vs. placebo for cognitive symptoms. Small initial cognitive gain that did not persist at 6 months.
- Berende et al. (2016, NEJM) — 12 weeks oral doxycycline, clarithromycin-hydroxychloroquine, or placebo after induction ceftriaxone. No benefit over placebo.
Against no benefit, the trials documented real harm: Clostridioides difficile colitis, central-line bloodstream infections (including fatal ones), gallbladder disease from ceftriaxone, candidiasis, and drug rashes. This is why mainstream infectious disease physicians will not prescribe multi-month antibiotics for persistent symptoms — not because they dismiss suffering, but because the intervention has been studied and it does not work.
Re-Treatment After a First Course
If clear objective findings return or persist (recurrent EM, persistent arthritis, new carditis or neurologic signs), a single repeat oral course is reasonable:
- For persistent Lyme arthritis: repeat 28-day doxycycline or a 2–4 week IV ceftriaxone course.
- For recurrent EM: a fresh oral course (usually implies a new tick bite, not treatment failure).
- For persistent subjective symptoms (fatigue, cognitive complaints, myalgia) without objective findings: no additional antibiotics. See the section below.
Do not escalate to months of IV therapy. It has been tested, it does not work, and it causes serious complications.
Drug Interactions and Side Effects
Doxycycline.
- Photosensitivity. Easily sunburned even through a cloudy sky. Use broad-spectrum SPF 30+, long sleeves, a hat. Crucial in summer, which is exactly when most Lyme is treated.
- Esophagitis. Take each dose with a full 8-ounce glass of water and remain upright (standing or sitting) for at least 30 minutes afterward. Never swallow a pill dry or just before bed.
- Chelation. Dairy, calcium supplements, iron supplements, antacids, and bismuth reduce absorption. Separate by at least 2 hours.
- GI upset. Common. Taking with food (non-dairy) is acceptable and does not meaningfully reduce efficacy.
Amoxicillin.
- Generally well tolerated. Diarrhea and yeast overgrowth are the main issues.
- Classic maculopapular rash if co-infected with EBV (mononucleosis). This is a non-allergic drug-virus interaction, not a true penicillin allergy, though it still warrants stopping the drug in that episode.
Cefuroxime axetil.
- GI upset; diarrhea. Take with food to improve absorption and reduce nausea.
- Minor cross-reactivity risk in penicillin-allergic patients (<1% for non-anaphylactic allergies).
Ceftriaxone (IV).
- Biliary sludge and pseudolithiasis — can mimic gallstones; usually reversible on stopping the drug but occasionally causes cholecystitis.
- Line-related complications: bloodstream infection, thrombosis, mechanical failure.
- C. difficile colitis.
If Symptoms Persist After Treatment
About 10–20% of treated patients report lingering fatigue, cognitive complaints (brain fog, word-finding trouble), myalgia, or arthralgia for 6 months or longer after a completed antibiotic course. This is called Post-Treatment Lyme Disease Syndrome (PTLDS). The symptoms are real and often disabling.
What PTLDS is not: evidence of persistent live infection. Repeated large, well-designed studies have failed to culture viable Borrelia from these patients or to demonstrate benefit from extended antibiotics. The leading current hypotheses are immune dysregulation, persistent non-viable bacterial antigens, autoimmunity, small-fiber neuropathy, and microbiome disruption from the initial treatment itself.
Management is symptomatic and multimodal: graded exercise, sleep optimization, treatment of co-existing conditions (dysautonomia, MCAS, co-infections, thyroid disease), cognitive rehabilitation, and mental-health support. See the dedicated PTLDS and Chronic Lyme article for a full treatment framework.
Key Research Papers
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. Clinical Practice Guidelines by the IDSA, AAN, and ACR: 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1–e48.
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: IDSA Guidelines. Clin Infect Dis. 2006;43(9):1089–1134.
- Klempner MS, Hu LT, Evans J, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001;345(2):85–92.
- Dattwyler RJ, Halperin JJ, Volkman DJ, Luft BJ. Treatment of late Lyme borreliosis — randomised comparison of ceftriaxone and penicillin (oral vs. IV neuroborreliosis comparator). N Engl J Med. 1990.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on Lyme antibiotic regimens, comparative trials, and adverse-event data:
- Doxycycline Lyme disease treatment
- Ceftriaxone and Lyme neuroborreliosis
- Lyme arthritis antibiotic treatment
- Amoxicillin for Lyme disease in children
- Lyme carditis and AV block management
- Jarisch-Herxheimer reaction in Lyme disease
- Post-treatment Lyme disease syndrome and prolonged antibiotics
- Oral vs. intravenous antibiotics for Lyme disease
Connections
- PTLDS and Chronic Lyme
- Lyme Neuroborreliosis
- Lyme Disease Overview
- Erythema Migrans Rash
- Tick-Borne Co-Infections
- Prevention and Tick Removal
- Tick Bite First Aid
- Lyme Testing Explained
- Alpha-Gal Syndrome
- Arthritis
- Meningitis
- Fatigue
- Lyme Carditis
- Headache
- Cat's Claw
- Immune Boosting