Tick Bite First Aid and Single-Dose Doxycycline Prophylaxis
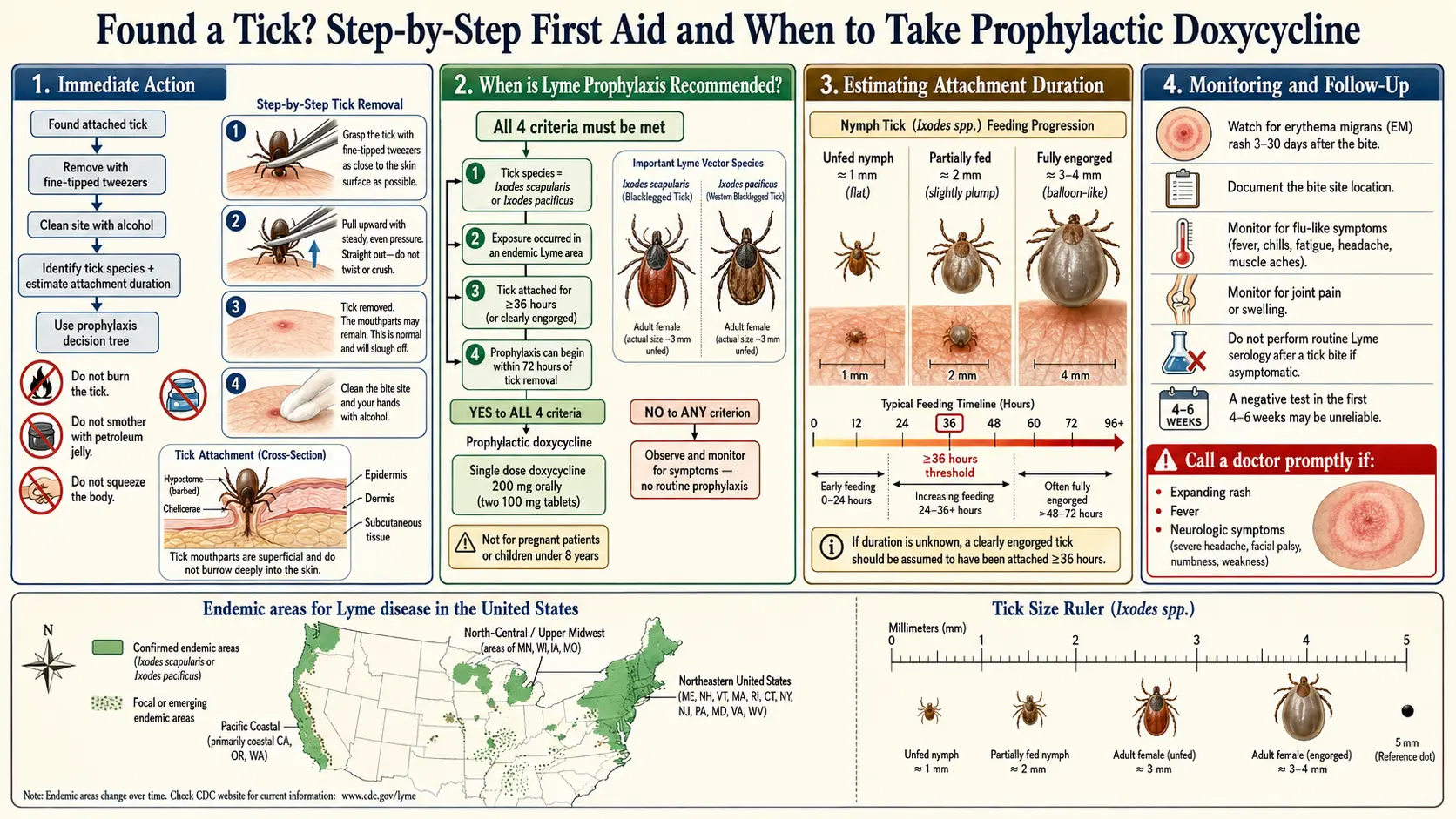
Table of Contents
- The 72-Hour Clock — Why Time-to-Action Matters
- Step-by-Step Tick Removal
- What NOT to Do
- If the Head or Mouthparts Break Off
- After Removal — Clean, Photograph, Document
- Save the Tick
- Tick Species That Matter
- Engorgement — Reading the Body Size
- Single-Dose Doxycycline Prophylaxis — The IDSA 2020 Criteria
- If You Do Not Qualify for Prophylaxis
- Pregnancy and Children Under Eight
- What to Watch For Over the Next 30 Days
- Tick Testing — What It Can and Cannot Tell You
- When to Skip Prophylaxis and Treat Empirically
- Key Research Papers
- Connections
- Featured Videos
The 72-Hour Clock — Why Time-to-Action Matters
You just found a tick. Take a breath. Most tick bites do not transmit disease, and even the ones from infected ticks usually do not cause Lyme if you act within the next few days. But there is a clock, and it has two hands worth knowing about.
The first hand is the attachment clock. The Lyme spirochete Borrelia burgdorferi lives in a tick's midgut. When the tick starts feeding, the bacteria have to migrate from the gut to the salivary glands before they can enter you. In laboratory and field studies, that migration typically requires 36 to 48 hours of attachment. Ticks pulled off within the first 24 hours rarely transmit Lyme; ticks attached longer than 72 hours transmit most reliably. Other pathogens have different timelines — Powassan virus can transfer in as little as 15 minutes, and Anaplasma may transmit faster than Borrelia — but the 36-hour threshold drives almost all prophylaxis decisions.
The second hand is the prophylaxis clock. If you qualify for the single-dose doxycycline regimen, it must be taken within 72 hours of tick removal. So the practical rule: remove the tick now, assess calmly, decide today or tomorrow — not next week.
Step-by-Step Tick Removal
The only tool that reliably works is a pair of fine-tipped tweezers. Drugstore tweezers with slanted wide tips are the wrong tool — they crush the tick's body and can force gut contents into the wound. Look for pointed, straight-tipped tweezers labeled for splinter or tick removal.
- Expose the bite. Good light. Reading glasses if you need them. A magnifying glass helps for nymphs, which are poppy-seed sized.
- Grasp the tick as close to the skin surface as possible. You are aiming for the mouthparts, not the body. The body is the balloon; the mouthparts are the straw embedded in you.
- Pull upward with steady, even pressure. Straight up. Do not twist. Do not jerk. Do not saw back and forth. The tick's mouthparts have backward-facing barbs; steady traction lets them release.
- Expect 10 to 30 seconds of pulling. It will feel stuck. Keep the pressure on. If you rush, you will leave mouthparts behind or squeeze the body and inject saliva.
- Once the tick releases, do not squish it with your fingers. Drop it into a zip-top bag or small container.
- Clean the bite site with soap and water, then rubbing alcohol or an iodine-based antiseptic.
- Wash your hands thoroughly.
If you are removing a tick from a child or from a spot you cannot easily see (scalp, behind an ear, back), ask another adult to do it. Panic and awkward angles cause most of the crushed-body mistakes.
What NOT to Do
Folk remedies for tick removal are nearly all counterproductive. They either do nothing or actively increase your infection risk by stressing the tick into regurgitating gut contents into the wound.
- Do not smother with petroleum jelly, nail polish, or liquid soap. The tick does not quickly suffocate; it stays attached for hours while stress hormones rise and it salivates more — exactly the saliva that carries pathogens.
- Do not burn with a hot match or lighter. Aside from giving yourself a burn scar next to the bite, heat makes the tick regurgitate and can cause it to rupture.
- Do not use essential oils, alcohol, gasoline, or bleach on the attached tick. Same problem: chemical irritation drives the tick to salivate and regurgitate.
- Do not twist or unscrew. Ticks do not have threaded mouthparts. Twisting snaps off the head.
- Be cautious with "tick keys" and lasso tools. Commercial removal devices (Tick Key, Tick Twister, Ticked Off spoons) can work well for large, fully-engorged adult ticks where there is enough of a tick body to catch. On tiny nymphs, flush against the skin, these tools often slide off or slice the tick in half. If you already own and have practiced with one, fine — otherwise the default tool is still pointed tweezers.
If the Head or Mouthparts Break Off
This is common, especially with nymphs or when removal is rushed. What you see is a tiny black fleck embedded where the tick was. Do not panic. Do not dig at it with a needle. Do not squeeze like a pimple.
Residual mouthparts act like a splinter. Infection risk is low — the bacteria live in the tick's body, not its mouth — and the pieces will usually work their way out over days to a couple of weeks. Clean the site, apply an antiseptic, and leave it alone. If the area becomes red, warm, painful, or starts draining pus after several days, that is a local skin infection (typically Staphylococcus or Streptococcus) — not Lyme — and warrants a clinic visit. Aggressive digging with unsterile tools causes far more infections than retained mouthparts.
After Removal — Clean, Photograph, Document
Once the tick is out and the bite is clean, spend three minutes on documentation. Future-you will be grateful.
- Photograph the bite site. A close-up with something for scale (a coin, a ruler, or a fingernail) and a wider shot showing the anatomical location. If an expanding rash develops later, you will want a baseline image from day zero.
- Photograph the tick. Top view and side view, on a white background, next to a coin or ruler. This is the single most useful piece of evidence for a clinician deciding about prophylaxis. Species identification from a good photograph is quick; from a verbal description, it is a guessing game.
- Write down the date, time, and approximate attachment duration. How long could it have been on you? When was your last shower or clothing change before you found it? The answer feeds directly into the 36-hour threshold.
- Note the location and the activity. Hiking in Connecticut in June is a different risk profile than brushing a tick off your dog in suburban Arizona.
Save the Tick
Do not flush it, do not squish it, do not drop it outside. A saved tick is cheap insurance.
- If the tick is alive (most are, right after removal), drop it into a small zip-top bag or screw-top container with a tiny piece of slightly damp paper towel. Seal. The moisture keeps it alive for species ID and possible commercial pathogen testing.
- If the tick is dead or you have crushed it, preserve it in a few drops of rubbing alcohol (70% isopropyl) in a sealed container. Alcohol-preserved ticks are still fine for PCR-based pathogen testing and visual species identification.
- Label the container with the date of removal, the person it came from, and the geographic location of likely exposure (town or park).
- Store in the refrigerator — not the freezer — until you decide whether to ship it to a testing lab.
Tick Species That Matter
Not every tick carries Lyme. In North America, four genera do most of the damage, and each carries a different set of pathogens. Identifying the species narrows the threat list dramatically.
- Ixodes scapularis (blacklegged tick, deer tick). The primary Lyme vector in the eastern and upper-midwestern United States. Also transmits anaplasmosis, babesiosis, Powassan virus, Borrelia miyamotoi, and Borrelia mayonii. Small and dark, with a solid dark scutum (back shield) on the female and a uniformly dark body on the male. Nymphs are poppy-seed size and are the main source of human Lyme.
- Ixodes pacificus (western blacklegged tick). The Pacific Coast cousin. Transmits Lyme and anaplasmosis in California, Oregon, and Washington. Overall Lyme risk is lower than on the east coast (the western fence lizard's blood kills Borrelia in juvenile ticks), but bites still warrant assessment.
- Amblyomma americanum (lone star tick). Aggressive, widespread across the southeastern and mid-Atlantic U.S. and moving north. The adult female has a single white dot on her back. Does not transmit classic Lyme. Does transmit ehrlichiosis, STARI (southern tick-associated rash illness — a Lyme-like rash with unclear etiology), Heartland virus, and is the cause of alpha-gal syndrome, the mammalian-meat allergy.
- Dermacentor variabilis (American dog tick) and Dermacentor andersoni (Rocky Mountain wood tick). Larger, brown with ornate white patterning. Primary vectors of Rocky Mountain spotted fever (Rickettsia rickettsii), tularemia, and tick paralysis. Not Lyme vectors.
Practically: if the tick is not an Ixodes, single-dose doxycycline prophylaxis for Lyme does not apply. But other tick-borne illnesses still do, so the documentation and watch-for-symptoms steps remain just as important.
Engorgement — Reading the Body Size
How long was it attached? The tick's body tells you more than your memory does.
- Flat and dark, looks like a freckle or poppy seed. The tick has barely fed. Attachment likely under 24 hours. Lyme transmission risk is low even from an infected tick.
- Slightly rounded, body paler at the edges but still dark overall. Partially fed, probably 24–48 hours attached. This is the grey zone where the 36-hour threshold matters most.
- Clearly swollen, pale gray or cream-colored balloon-shape with small dark legs. Fully or near-fully engorged. Attached 48–96+ hours. Maximum transmission risk.
For nymphs, the flat-to-engorged progression swells a barely-visible body to about sesame-seed size. Adult female Ixodes go from roughly 3 mm flat to 10 mm fully engorged. Tick-ID references online include photo plates of feeding stages — another reason to photograph your tick before preserving it.
Single-Dose Doxycycline Prophylaxis — The IDSA 2020 Criteria
The Infectious Diseases Society of America's 2020 Lyme guideline recommends a single 200 mg oral dose of doxycycline as post-exposure prophylaxis when all of the following criteria are met:
- The attached tick is reliably identified as Ixodes scapularis (or I. pacificus in the west).
- The tick has been attached for 36 hours or longer, or is visibly engorged.
- Prophylaxis can be started within 72 hours of tick removal.
- The bite occurred in an area where the local Ixodes infection rate with Borrelia burgdorferi is at least 20% (most of New England, the mid-Atlantic, Minnesota, and Wisconsin meet this threshold).
- There is no contraindication to doxycycline (pregnancy, lactation in some protocols, age under 8 without clinical judgment, true doxycycline allergy).
Adult dose: 200 mg orally, single dose, taken with a full glass of water and ideally with food to reduce stomach upset.
Pediatric dose (age 8 and up): 4.4 mg/kg orally, single dose, up to a maximum of 200 mg.
The regimen rests on the 2001 Nadelman trial, a randomized placebo-controlled study in a high-endemic New York region showing that a single 200 mg dose reduced the development of erythema migrans from 3.2% in the placebo arm to 0.4% in the doxycycline arm — an 87% relative risk reduction.
Side effects from one 200 mg dose are usually limited to mild nausea for a few hours. Take with food, stay upright 30 minutes afterward to prevent esophageal irritation, and avoid dairy, antacids, or iron at the same time — these chelate doxycycline and cut absorption.
If You Do Not Qualify for Prophylaxis
The criteria above are strict for a reason: the trial evidence only supports the regimen in that narrow scenario. Outside of it, single-dose doxycycline has not been shown to help, and giving antibiotics when they are not needed has costs — resistance, microbiome disruption, side effects, and false reassurance.
You do not qualify if any of these apply:
- Attached less than 36 hours and not engorged.
- The tick is not an Ixodes species (lone star, dog tick, wood tick).
- The bite occurred in a low-endemic area (<20% local infection rate — much of the South, Mountain West, and Pacific Coast).
- More than 72 hours have passed since removal.
What to do instead: watchful waiting with daily skin checks. Look at the bite site every day for 30 days. Take a photograph once a week to compare. Watch for a red, expanding rash — the classic erythema migrans (EM) — which typically appears 3 to 30 days after the bite (median around 7 days), starts as a small red spot, and expands to a ring or bullseye of 5 cm or more. Also watch for unexplained fever, chills, aches, severe headache, stiff neck, facial palsy, or new joint pain. Any of those symptoms in the 30-day window after a tick bite warrants a clinician visit and, if Lyme is suspected, empirical treatment without waiting for serology.
Pregnancy and Children Under Eight
Doxycycline is traditionally restricted in pregnancy and in children under 8 because of fetal tooth and bone development concerns. Recent data suggest short courses are likely safe, but single-dose prophylaxis for Lyme in these groups remains off-protocol and physician-directed.
Pregnancy. A bite that would otherwise qualify should trigger a same-day call to the obstetrician or primary care clinician. Options include close observation with a low threshold for amoxicillin if EM appears, or an abbreviated empiric amoxicillin course started immediately.
Children under 8. Similar logic. The AAP considers a single 4.4 mg/kg doxycycline dose safe, and some clinicians extend that to prophylaxis in clearly qualifying cases. Others prefer amoxicillin or observation with prompt treatment if EM appears. Call the pediatrician; do not self-treat.
What to Watch For Over the Next 30 Days
Whether or not you take prophylaxis, the monitoring window is the same: 30 days from tick removal. Mark it on your calendar.
- Daily check of the bite site. Watch for a red spot that starts at the bite and expands larger than a quarter over days. Central clearing (the "bullseye") happens in about 20–30% of EM rashes; the remainder are solid red expanding patches. EM is typically not itchy and not painful, which distinguishes it from local allergic reactions.
- Weekly photograph of the bite site for objective comparison.
- Fever, chills, fatigue, headache, muscle aches. A flu-like illness 1–4 weeks after a tick bite is Lyme, anaplasmosis, or babesiosis until proven otherwise. Call your clinician same-day.
- New joint pain, facial drooping, palpitations, severe headache, or stiff neck. These are disseminated or neurologic Lyme features. Seek care promptly.
- Any rash anywhere on the body — not just at the bite. Secondary EM lesions can appear at sites distant from the original bite in disseminated disease.
Tick Testing — What It Can and Cannot Tell You
Several commercial labs offer PCR testing of mailed-in ticks for Borrelia, Anaplasma, Babesia, and other pathogens. The best known are TickCheck, UMass TickReport, and IGeneX. Cost runs roughly $50–$150 per tick, and turnaround is typically 3–7 business days.
What tick testing is good for:
- Confirming a positive tick can support a decision to watch more closely, pursue prophylaxis in borderline cases, or treat empirically if symptoms appear.
- Identifying co-infections (babesiosis, anaplasmosis) that change the empirical antibiotic choice.
- Local surveillance data — some labs report aggregate results by zip code, useful for understanding your area's risk.
What it is not good for:
- A negative tick PCR does not rule out your infection. You may have been bitten by another tick you never saw. The sensitivity is also imperfect.
- A positive tick does not guarantee you were infected. Transmission depends on attachment duration and a handful of biological factors.
- The result rarely arrives within the 72-hour prophylaxis window. Do not delay the prophylaxis decision waiting for lab results.
In short, tick testing is a useful supplement to clinical decision-making, not a substitute for it.
When to Skip Prophylaxis and Treat Empirically
Single-dose prophylaxis is for asymptomatic people with a known recent bite. If any of the following are present, you have moved past prophylaxis and into empirical treatment for presumed Lyme — which means a full course of antibiotics (typically 10–21 days of doxycycline, amoxicillin, or cefuroxime axetil) started on clinical grounds without waiting for serology.
- An expanding erythema migrans rash has appeared — regardless of whether you ever saw a tick. EM is itself a clinical diagnosis of Lyme, and serology is often negative in the first 2–4 weeks of infection.
- Fever, chills, severe headache, or flu-like illness without obvious cause within a month of a tick bite, especially in an endemic area.
- New facial palsy, meningitis-like symptoms, palpitations with heart block, or large-joint swelling following a tick bite or exposure — these are disseminated Lyme presentations requiring immediate care.
- A clearly engorged Ixodes tick found days to weeks after the bite — too late for prophylaxis but a strong indication to start monitoring and have a low threshold for empirical treatment at the first symptom.
See the antibiotic treatment protocols article for detailed regimens and durations once the decision is empirical rather than prophylactic.
The core message: tick bites are common, disease is far less so, and careful action in the first 72 hours resolves almost every case cleanly. Remove the tick, save it, document, assess, and call your clinician. Panic is not part of the protocol.
Key Research Papers
- Lantos PM, et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021.
- Nadelman RB, et al. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med. 2001.
- Warshafsky S, et al. Efficacy of antibiotic prophylaxis for the prevention of Lyme disease: an updated systematic review and meta-analysis. J Antimicrob Chemother. 2010.
- Sood SK, et al. Duration of tick attachment as a predictor of the risk of Lyme disease in an area in which Lyme disease is endemic. J Infect Dis. 1997.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on tick bite management, transmission biology, and Lyme prophylaxis:
- Doxycycline prophylaxis after tick bite
- Ixodes scapularis attachment time and Borrelia transmission
- Tick removal techniques and comparison of devices
- Powassan virus and rapid tick-borne transmission
- Lone star tick and alpha-gal syndrome
- Rocky Mountain spotted fever and Dermacentor vectors
- Commercial tick testing and PCR for Borrelia
- Doxycycline safety in pregnancy and young children
Connections
- Erythema Migrans Rash
- Antibiotic Treatment Protocols
- Alpha-Gal Syndrome
- Lyme Disease Overview
- Meningitis
- Lyme Neuroborreliosis
- Prevention and Tick Removal
- PTLDS and Chronic Lyme
- Lyme Testing Explained
- Tick-Borne Co-Infections
- Sepsis
- Headache
- Joint Pain
- Lyme Carditis
- Cat's Claw
- Tick Bite Prevention