Lyme Carditis & Cardiac Complications
Lyme carditis is the heart complication of early-disseminated Lyme disease. It is uncommon, it is almost always reversible with prompt antibiotic treatment, and it is one of the only bacterial infections in North America that can kill a healthy 25-year-old in their sleep. The good news dominates the story: catch it, treat it, and within a few weeks the heart's electrical wiring typically comes back online, fully normal, and stays that way for life. The hard news is that it is easy to miss, because the early symptoms — lightheadedness, palpitations, fatigue — look like a hundred other things, and the rash that should tip doctors off has often faded or was never on a visible part of the body. This page explains what Lyme carditis is, how to recognize it, what to expect in the emergency department and hospital, and why almost no one who gets it needs a permanent pacemaker.
Table of Contents
- What Lyme Carditis Is
- Who Gets It and How Often
- Symptoms — What to Watch For
- AV Block Explained
- Diagnosis — ECG, Telemetry, Serology, SILC
- Treatment — Antibiotics and Temporary Pacing
- Why You Almost Never Need a Permanent Pacemaker
- Pericarditis and Myocarditis
- Sudden Death — The Rare but Real Risk
- Distinguishing Lyme Carditis from Other Causes
- Recovery and Follow-Up
- Key Research Papers
- Connections
- Featured Videos
What Lyme Carditis Is
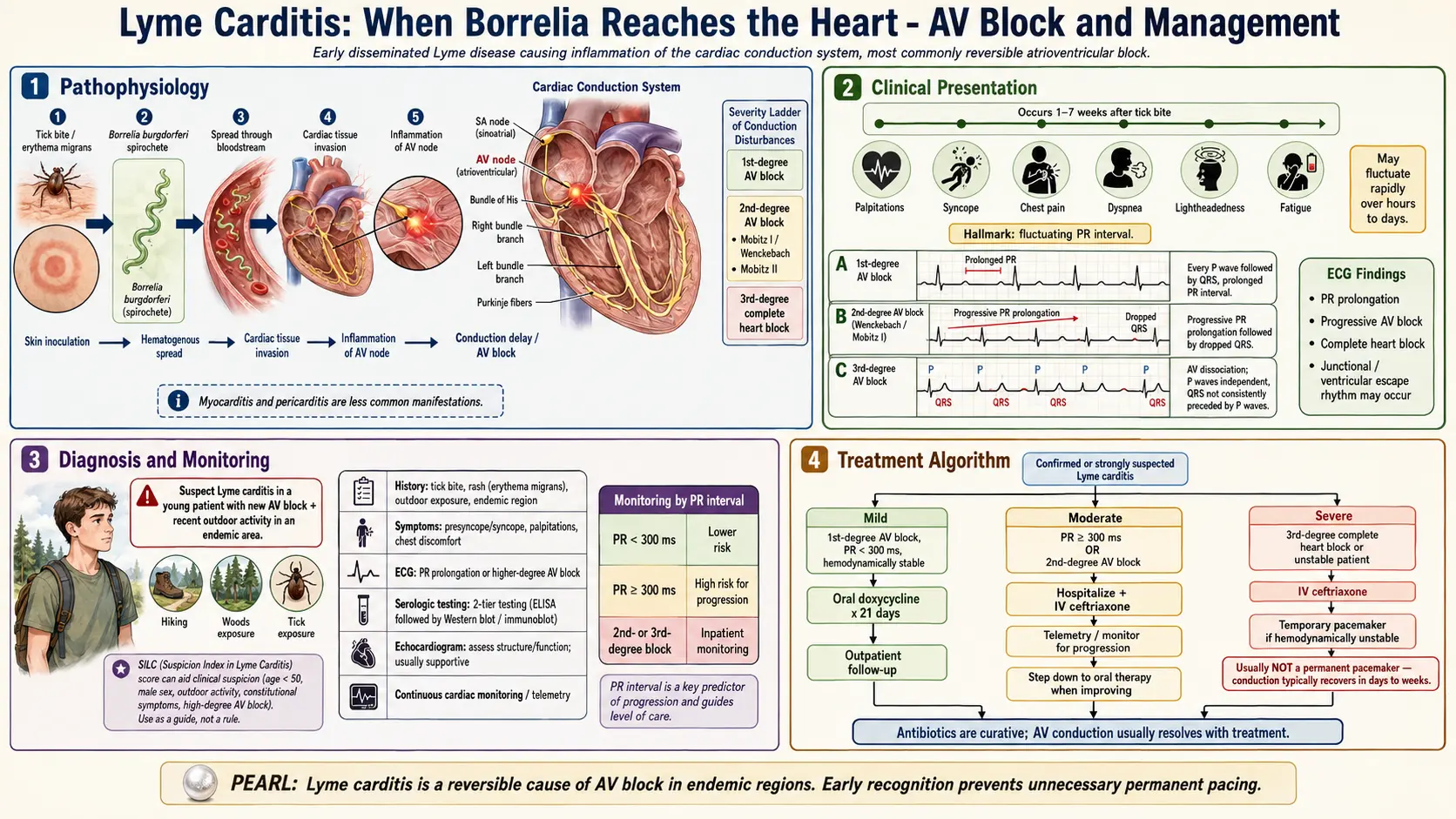
Lyme carditis is direct bacterial invasion of the heart by Borrelia burgdorferi (and occasionally related species such as B. mayonii) during the early-disseminated stage of Lyme disease — typically days to a few weeks after the tick bite. The spirochetes travel from the skin through the bloodstream and seed multiple tissues. In a small minority of patients, the bacteria reach the heart and settle preferentially in the atrioventricular (AV) node and the surrounding conduction tissue. Inflammation of the conduction system disrupts the electrical signal that normally travels from the atria to the ventricles, producing the hallmark feature of Lyme carditis: AV block.
Less commonly, the spirochete reaches the pericardium or the myocardium itself, causing pericarditis or myocarditis. Cardiac biopsies from rare fatal cases have shown spirochetes embedded in myocardial tissue surrounded by dense lymphocytic infiltrate — the signature of direct infection rather than an autoimmune after-effect.
The condition is time-limited. Antibiotics kill the bacteria within days, and the inflamed conduction tissue heals over one to six weeks. In contrast to ischemic heart disease or idiopathic heart block, Lyme carditis leaves no lasting scar in the conduction system in the vast majority of treated patients.
Who Gets It and How Often
Among untreated early Lyme disease in endemic areas of the U.S. northeast, upper midwest, and mid-Atlantic, roughly 1% of cases develop symptomatic carditis. Subclinical ECG changes without symptoms may be more common, but the clinically significant cases — the ones that land someone in the hospital — cluster around that 1%.
The demographic skews young and male. Most case series report a peak in men aged 15–40, reflecting both outdoor-exposure patterns (landscaping, hiking, military, hunting) and some still-unexplained sex difference in how the infection interacts with the conduction system. Women and older adults get Lyme carditis too, but the classic patient is a physically fit young man who tells the emergency room he was feeling great a week ago and now he keeps nearly fainting when he stands up.
Geographically, almost all U.S. cases originate in the high-incidence states: Connecticut, Massachusetts, Rhode Island, New York, New Jersey, Pennsylvania, Maryland, Delaware, Virginia, Vermont, New Hampshire, Maine, Minnesota, Wisconsin. Cases outside these areas are almost always travel-related. Europe sees Lyme carditis as well, often associated with B. afzelii or B. garinii, though the incidence per infection appears slightly lower than in North America.
Symptoms — What to Watch For
Symptoms typically arrive days to weeks after the tick bite, often overlapping with or just after an erythema migrans rash. In about a third of carditis cases the rash is already gone or was never noticed. Patients may also have a viral-flu-like illness (fever, sweats, muscle aches, headache) before the cardiac symptoms appear. The cardiac picture itself is distinctive once you know what to look for:
- Lightheadedness and presyncope. A feeling of almost fainting, especially on standing, walking up stairs, or exerting yourself. Often the first symptom.
- Syncope. Brief loss of consciousness, usually with rapid spontaneous recovery. May happen once or repeatedly.
- Palpitations. An awareness of the heartbeat — skipped beats, pounding, irregular rhythm.
- Chest pain or pressure. Usually mild, sometimes positional (worse lying flat, better leaning forward) when pericarditis is present.
- Shortness of breath. Particularly on exertion.
- Unusual fatigue. Out of proportion to activity, sometimes the only symptom.
- Slow pulse. A resting heart rate under 50 in a previously healthy adult should prompt evaluation.
Any of these in a patient with known or possible tick exposure — a recent hike, camping trip, rural yard work, or an EM rash — should prompt an ECG the same day. Do not wait to "see if it passes." Lyme carditis can progress from first-degree to third-degree AV block within hours.
AV Block Explained
The atrioventricular (AV) node is a small bundle of specialized cells between the upper chambers (atria) and lower chambers (ventricles) of the heart. Every heartbeat starts in the atria and must pass through the AV node to reach the ventricles. When Borrelia inflames the AV node, that electrical signal slows, stutters, or drops out entirely.
The three degrees of AV block, in order of severity:
- First-degree AV block. The signal reaches the ventricles but takes longer than normal. Visible on ECG as a prolonged PR interval (> 200 ms, often much longer in Lyme carditis — PR intervals of 300–400 ms are common). Usually asymptomatic. Mild cases with PR < 300 ms and no symptoms can often be treated at home with oral antibiotics.
- Second-degree AV block. Some beats conduct through to the ventricles and some do not. Subdivided into Mobitz I (Wenckebach, a progressive lengthening until a beat drops) and Mobitz II (intermittent dropped beats without warning). Either type with symptoms warrants hospital admission.
- Third-degree (complete) AV block. No signal reaches the ventricles from the atria; the ventricles generate their own slow backup rhythm. Heart rates of 30–40 are common. This is a medical emergency. Patients can suddenly lose consciousness or die if the backup rhythm fails.
A striking feature of Lyme carditis is how quickly the degree of block can shift. A patient can walk into the ER with a first-degree block and progress to third-degree within hours. This is why continuous telemetry monitoring — not just a single ECG — is standard for any symptomatic or higher-degree block.
Diagnosis — ECG, Telemetry, Serology, SILC
Diagnosis combines clinical suspicion with a small battery of tests. The workup:
- 12-lead ECG. The starting point. Measures the PR interval and identifies any degree of AV block. Should be done immediately in any patient with palpitations, presyncope, or syncope in an endemic area.
- Continuous telemetry. Required for any patient with symptomatic block or block beyond first-degree. Captures intermittent high-grade block that a single ECG might miss and allows minute-to-minute monitoring as the patient is treated.
- Lyme serology. Two-tier testing — ELISA followed by Western blot — is the standard. See the testing article. Note that serology can be negative in the first 1–2 weeks of infection; treatment should not wait for the result if clinical suspicion is high.
- Basic cardiac workup. Troponin, BNP, chest X-ray, echocardiogram to rule out concurrent myocarditis or pericardial effusion, and blood cultures to exclude bacterial endocarditis.
- Endomyocardial biopsy. Rarely needed. Reserved for atypical presentations, suspected alternative diagnoses (giant cell myocarditis, sarcoidosis), or failure to respond to antibiotics.
The SILC Score
The Suspicious Index in Lyme Carditis (SILC) score, developed by Besant and colleagues in 2018, is a practical tool for ER physicians and cardiologists trying to decide whether a new AV block is Lyme-related. It assigns points for:
- Constitutional symptoms (fever, malaise, arthralgia, myalgia) — 2 points
- Outdoor activity or endemic area exposure — 1 point
- Male sex — 1 point
- Tick bite history — 3 points
- Erythema migrans rash — 4 points
- Age under 50 — 1 point
Scores are interpreted as low (0–2), intermediate (3–6), or high (7–12) probability of Lyme carditis. A high score supports presumptive antibiotic treatment while serology is pending. A low score in a non-endemic area argues for looking elsewhere (ischemia, sarcoidosis, medication-induced block).
Treatment — Antibiotics and Temporary Pacing
Treatment has two simultaneous arms: antibiotics to kill the infection and supportive cardiac care to keep the patient alive until the conduction system recovers.
Antibiotic Regimens (IDSA/AAN/ACR 2020 guidelines)
- Hospitalized patients with high-degree (second- or third-degree) block, or first-degree block with PR ≥ 300 ms with symptoms: IV ceftriaxone 2 g once daily for 14–21 days. Ceftriaxone may be transitioned to oral doxycycline once the block has improved and the patient is stable, completing a total 14–21 day course.
- Outpatient mild first-degree block (PR < 300 ms) without symptoms: oral doxycycline 100 mg twice daily for 14–21 days. Amoxicillin or cefuroxime axetil are alternatives for pregnancy or doxycycline intolerance.
- Pediatric and pregnant patients: regimens are adjusted — doxycycline is now considered acceptable in young children for short Lyme courses, but pregnancy uses amoxicillin or ceftriaxone.
See the antibiotic protocols page for full dosing across all Lyme manifestations.
Supportive Cardiac Care
- Continuous telemetry monitoring until the PR interval is back under 300 ms and any high-degree block has resolved.
- Temporary transvenous pacing for symptomatic third-degree or high-grade second-degree block. A pacing wire is threaded through a central vein into the right ventricle and attached to an external pulse generator. It keeps the heart beating at a safe rate while the antibiotics work.
- Transcutaneous (external) pacing pads placed on the chest as a bridge if transvenous pacing is not immediately available.
- Avoid negative chronotropic medications (beta-blockers, calcium channel blockers, digoxin) which can worsen the block.
Most patients demonstrate improvement in conduction within 3–7 days of starting IV antibiotics. The PR interval typically normalizes completely within 1–6 weeks.
Why You Almost Never Need a Permanent Pacemaker
This is one of the most important teaching points in Lyme carditis, and it is occasionally missed even in well-staffed hospitals. Lyme-induced heart block resolves. In the large majority of cases, the conduction tissue heals completely, and the patient walks out of the hospital with a normal ECG and no implanted hardware.
A permanent pacemaker implanted reflexively during the acute phase — before the clinician realizes this is Lyme — is likely to become a lifelong foreign body that the patient never actually needed. The device brings real costs: infection risk, lead fracture, battery replacements every 7–10 years, MRI restrictions, and surgical revisions. Avoiding unnecessary permanent pacing is one of the highest-value clinical decisions in all of Lyme medicine.
The right approach: temporary pacing only, while antibiotics do the work. Reserve permanent pacing for the rare patient whose high-grade block persists beyond 6 weeks of completed antibiotic therapy — at which point it is reasonable to believe the conduction tissue has been permanently damaged and will not recover.
Pericarditis and Myocarditis
A smaller subset of Lyme carditis patients develop inflammation of the heart muscle itself (myocarditis) or the sac around it (pericarditis), with or without concurrent AV block.
- Pericarditis presents with sharp, positional chest pain — worse lying flat, better sitting up and leaning forward. ECG shows diffuse ST elevation and PR depression. Echocardiogram may show a small pericardial effusion. Treated with antibiotics; NSAIDs are added for pain and inflammation. Tamponade is very rare.
- Myocarditis presents with chest pain, shortness of breath, arrhythmias, and an elevated troponin. Echocardiogram may show reduced ejection fraction or wall motion abnormalities. Cardiac MRI shows patchy delayed-enhancement suggesting inflammation. Treated with antibiotics and heart-failure supportive care (diuretics, ACE inhibitors, beta-blockers once block has resolved). Most cases recover full left ventricular function.
- Chronic Lyme cardiomyopathy has been reported, particularly in Europe with B. burgdorferi sensu lato species, though the evidence base is thinner and the association less accepted than the acute carditis picture.
Sudden Death — The Rare but Real Risk
In 2013, the CDC published a Morbidity and Mortality Weekly Report documenting three sudden cardiac deaths in young adults (ages 26, 38, and 49) attributed to previously undiagnosed Lyme carditis. In all three, spirochetes were identified at autopsy in cardiac tissue by PCR, immunohistochemistry, or silver staining. None had been diagnosed with Lyme before death; two had had flu-like symptoms in the weeks prior; one had a transient rash the family did not recognize. Additional fatal cases have been reported in the medical literature since.
These deaths are vanishingly rare in absolute terms — a handful of cases per tens of thousands of annual Lyme infections — but they illustrate the stakes of missed diagnosis. Anyone in an endemic area presenting with unexplained syncope, near-syncope, or new bradycardia should have Lyme carditis actively considered and an ECG obtained the same day. The diagnostic threshold in endemic regions should be low, because the downside of missing it is catastrophic and the treatment is simple.
Distinguishing Lyme Carditis from Other Causes
New-onset AV block in an adult has a sizable differential. Features that point toward Lyme rather than the alternatives:
- Age and health. Lyme carditis favors young, otherwise-healthy adults. Ischemic heart block favors older adults with cardiovascular risk factors.
- Exposure history. Outdoor activity, known tick bite, time spent in an endemic region within the past month.
- Associated symptoms. Recent EM rash, viral-flu-like illness, new arthralgias, or facial nerve palsy strongly favor Lyme.
- Speed of recovery. Lyme heart block improves rapidly with antibiotics. Ischemic or idiopathic block does not.
- Echocardiogram. Typically normal structure and function in Lyme carditis. Wall motion abnormalities suggest ischemia; restrictive filling suggests amyloid or sarcoid.
Alternative causes to consider and rule out:
- Ischemic AV block (inferior wall myocardial infarction in particular) — rule out with troponin and ECG ischemic changes.
- Cardiac sarcoidosis — suggested by elevated ACE or extracardiac sarcoid features; diagnosed by cardiac MRI or FDG-PET.
- Giant cell myocarditis — rare, aggressive, often requires biopsy.
- Chagas disease — consider in patients with Latin American residence history.
- Medication-induced block — beta-blockers, calcium channel blockers, digoxin, amiodarone, clonidine.
- Congenital or idiopathic degenerative conduction disease (Lenegre-Lev syndrome) — usually older adults with slow progression.
Recovery and Follow-Up
After the acute episode, follow-up typically looks like this:
- Inpatient discharge occurs once the patient is off temporary pacing, the PR interval has improved below 300 ms, and there is no recurrence of high-grade block on telemetry for 24–48 hours.
- Outpatient ECG at 2 weeks and 4–6 weeks to confirm continued normalization of the PR interval.
- Event monitor or 30-day Holter if any residual palpitations or concern for intermittent block.
- Repeat echocardiogram at 3 months if myocarditis was present, to confirm recovery of ejection fraction.
- Return to exercise is typically cleared once ECG has normalized and any myocarditis has resolved — generally 4–8 weeks.
Long-term prognosis is excellent. The majority of treated patients have no residual cardiac disease and no increased long-term risk of heart block, arrhythmia, or cardiomyopathy. A small minority develop persistent first-degree block that remains asymptomatic and requires no treatment. Vanishingly few need a permanent pacemaker.
If fatigue, brain fog, or joint symptoms persist for months beyond antibiotic treatment, review the PTLDS article — persistent post-treatment symptoms are a distinct phenomenon from the acute carditis and are managed separately.
Key Research Papers
- Forrester JD, et al. Three sudden cardiac deaths associated with Lyme carditis — United States, November 2012–July 2013. MMWR Morb Mortal Wkly Rep. 2013;62(49):993–996.
- Yeung C, Baranchuk A. Diagnosis and Treatment of Lyme Carditis: JACC Review Topic of the Week. J Am Coll Cardiol. 2019;73(6):717–726.
- Steere AC, Strle F, Wormser GP, et al. Lyme borreliosis. Nat Rev Dis Primers. 2016;2:16090.
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. Clinical Practice Guidelines by the IDSA, AAN, and ACR: 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1–e48.
- Search PubMed
- Steere AC, Batsford WP, Weinberg M, et al. Lyme carditis: cardiac abnormalities of Lyme disease. Ann Intern Med. 1980;93(1):8–16.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on Lyme carditis epidemiology, diagnosis, and management:
- Lyme carditis and AV block
- Lyme carditis and sudden cardiac death
- SILC score for suspected Lyme carditis
- Ceftriaxone treatment in Lyme carditis
- Temporary pacing in Lyme carditis
- Lyme myocarditis and cardiomyopathy
- Borrelia burgdorferi and cardiac pathology
- Pediatric Lyme carditis
- Lyme disease and pericarditis
- Lyme carditis and permanent pacemaker outcomes
Connections
- Erythema Migrans Rash
- Antibiotic Treatment Protocols
- Lyme Testing Explained
- PTLDS and Chronic Lyme
- Lyme Disease Overview
- Lyme Neuroborreliosis
- Prevention and Tick Removal
- Tick Bite First Aid
- Tick-Borne Co-Infections
- Cardiovascular Disease
- Myocarditis
- Cardiomyopathy
- Arrhythmia
- Chest Pain
- Fatigue
- Endocarditis
- Lupus