Lyme Disease Testing Explained
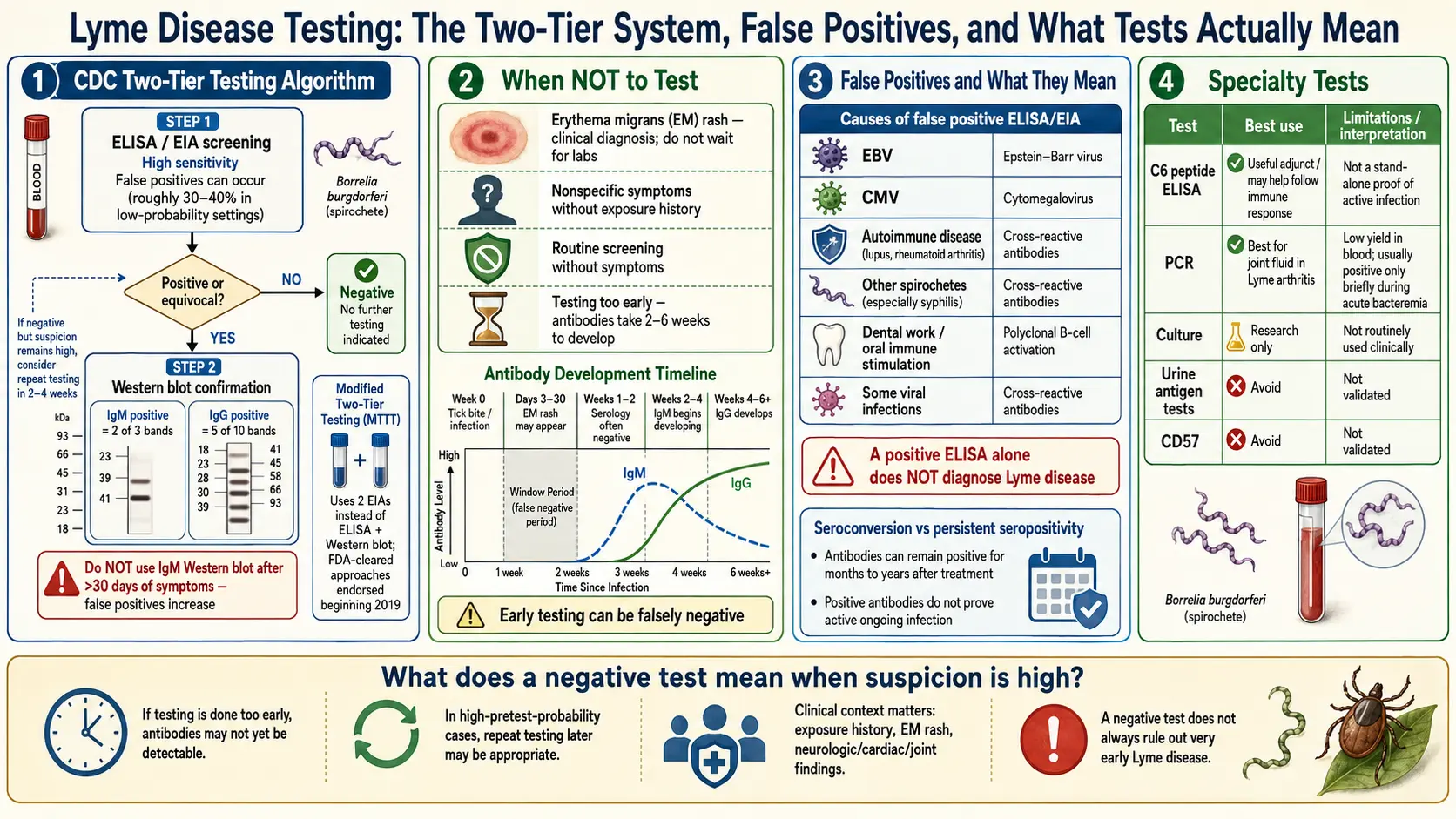
Table of Contents
- Why Lyme Testing Is Confusing
- Standard Two-Tier Testing (STTT)
- Modified Two-Tier Testing (MTTT)
- The Early-Window Problem
- Western Blot Band Interpretation
- False Positives — Other Causes
- When to Test — And When Not To
- PCR Testing
- Culture
- CSF Testing for Neuroborreliosis
- C6 Peptide ELISA
- "Chronic Lyme" Labs to Avoid
- Seronegative Lyme
- Post-Treatment Serology
- Special Populations
- Key Research Papers
- Connections
- Featured Videos
Why Lyme Testing Is Confusing
If you have spent any time trying to figure out whether you have Lyme disease, you have already collided with the central frustration of this illness: there is no simple blood test that directly looks for the bacterium. Standard Lyme testing does not detect Borrelia burgdorferi itself. It detects the antibodies your immune system makes against Borrelia, which is a very different thing.
This matters for three reasons. First, antibodies take weeks to appear, so a test run during the first infection window is often negative even when you clearly have Lyme. Second, antibodies persist for years after successful treatment, so you cannot retest later to prove the bacteria are gone. And third, other infections and autoimmune conditions can generate antibodies that cross-react with the Lyme assay, producing false positives.
Most of the confusion, controversy, and despair that surrounds Lyme diagnosis traces back to this single fact. The test is indirect. The clinical picture — the rash, the tick exposure, the pattern of symptoms, the season — carries more weight than the lab result, especially early on. A good Lyme workup is a physician reading the story and using serology as one piece of evidence, not as a yes/no verdict.
Standard Two-Tier Testing (STTT)
The U.S. Centers for Disease Control and Prevention (CDC) has recommended a two-step strategy since 1995. It is the protocol most hospital and commercial labs still run when your clinician orders a "Lyme panel."
Step 1 — ELISA or IFA screen. An enzyme-linked immunosorbent assay (ELISA) looks for antibodies against a mixture of Borrelia antigens. It is designed to be sensitive, meaning it casts a wide net and catches most true positives, accepting that it will also flag some people who do not actually have Lyme.
Step 2 — Western blot confirmation. If the ELISA is positive or equivocal, the same blood sample is run on a Western blot, which separates Borrelia proteins by size on a gel and checks which specific bands your antibodies are attacking. Two blots are run: an IgM blot (early-phase antibodies) and an IgG blot (mature antibodies that appear weeks later).
A negative ELISA ends the workup — no blot is run, and the result is reported simply as negative. This is the design that misses early Lyme: if you test in the first two weeks of infection before antibodies have developed, the ELISA is negative and no further testing happens, even though you may be acutely infected.
Modified Two-Tier Testing (MTTT)
In July 2019, the CDC endorsed an alternative: modified two-tier testing, which replaces the Western blot with a second ELISA that targets different antigens than the first. Both steps are now enzyme immunoassays; the second confirms the first by looking at a distinct set of Borrelia surface proteins (commonly VlsE and C6).
The MTTT offers real advantages. Sensitivity in early disease is meaningfully higher than STTT, because the newer assays pick up antibodies against antigens that appear earlier in infection. Interpretation is simpler — you get two clean positive/negative results instead of a long list of blot bands to count. And the second step is cheaper and faster to run, which lowers the turnaround time and the bill.
If your clinician is willing, the MTTT is usually the better choice for early or ambiguous presentations. Specificity (avoiding false positives) is roughly equivalent to STTT. Both are CDC-endorsed as of 2019, and both are accepted for surveillance case definitions.
The Early-Window Problem
This is the single most important point in Lyme diagnostics, and patients who do not hear it explained clearly often suffer for it: serology is not reliable during the first few weeks of infection. Seroconversion — the moment your immune system starts making detectable antibodies against Borrelia — takes roughly two to six weeks after exposure. Before that window closes, you can have a textbook erythema migrans (EM) rash and still test stone-cold negative.
The published numbers are brutal. In early-localized disease (the EM stage), two-tier testing misses somewhere between 50% and 70% of cases. In early-disseminated disease (weeks later, with multiple rashes or facial palsy), sensitivity climbs to 70–90%. Only in late disease — arthritis, chronic neurologic involvement — does sensitivity reach the 95–99% range.
The practical rule follows directly: if you have a clinical EM rash in an endemic area, you treat. You do not wait for blood work. The rash is itself diagnostic under CDC criteria. Ordering serology in this situation is actually counterproductive, because a negative result can wrongly be used to deny treatment or to second-guess a correct diagnosis. Save the testing for later manifestations, for ambiguous rashes, and for disseminated presentations where antibodies have had time to develop.
Western Blot Band Interpretation
When STTT is used, the Western blot turns your result into a pattern of bands, each corresponding to a Borrelia protein of a particular molecular weight (measured in kilodaltons, kDa). The CDC has standardized which bands "count."
IgM criteria (positive if any 2 of 3 bands are present): 23 kDa (OspC), 39 kDa (BmpA), and 41 kDa (flagellin). The 41 band is the least specific — many unrelated bacterial infections produce anti-flagellin antibodies — so a "41-only" result is not a positive blot.
IgG criteria (positive if any 5 of 10 bands are present): 18, 23 (OspC), 28, 30, 39 (BmpA), 41 (flagellin), 45, 58, 66, and 93 kDa.
A crucial caveat that patients almost always miss: the IgM blot is only interpretable in the first 30 days of illness. After a month, IgM antibodies that persist can reflect old, resolved infection, cross-reactivity, or nonspecific B-cell activity. Using a positive IgM blot to diagnose Lyme at four months of symptoms is a common lab error that leads to misdiagnosis. After 30 days, you need IgG positivity to call it Lyme.
False Positives — Other Causes
Antibody tests see shapes, not identity, and many proteins from unrelated organisms resemble Borrelia closely enough to trigger a positive ELISA or a few Western blot bands. Known sources of cross-reactivity include:
- Other spirochetes — Treponema pallidum (syphilis), Leptospira species, and oral spirochetes from periodontal disease all share flagellar and surface antigens.
- Epstein-Barr virus (EBV) and other herpesviruses during acute or reactivated infection.
- Autoimmune disease — lupus, rheumatoid arthritis, and other conditions with high antinuclear antibody (ANA) titers.
- Other tick-borne illnesses — some Borrelia relapsing-fever species, including the agent of southern tick-associated rash illness (STARI).
- Chronic dental infections producing anti-oral-spirochete antibodies that hit the 41 kDa flagellin band.
This is why a single band — especially the 41 band — is never enough to call a blot positive, and why isolated IgM findings late in an illness rarely mean what they appear to mean.
When to Test — And When Not To
Do not test: patients with a classic EM rash in an endemic region. The rash is the diagnosis. A negative test is misleading; a positive test adds nothing.
Do test:
- Suspected early-disseminated disease — multiple EM lesions, facial (Bell's) palsy, carditis with AV block, or meningitis in an endemic area.
- Suspected Lyme arthritis — one or a few joints (knee especially), large effusions, weeks to months after possible exposure.
- Late neurologic manifestations — radiculopathy, encephalopathy, peripheral neuropathy with possible exposure history.
- Any non-rash presentation where Borrelia is reasonably on the differential.
Do not use serology for screening in low-prevalence areas or in patients with only nonspecific fatigue and aches. The pretest probability is too low and false positives dominate the result.
PCR Testing
Polymerase chain reaction (PCR) directly amplifies Borrelia DNA, bypassing the antibody problem entirely. If you find the DNA, the organism is there. The catch is that Borrelia rarely circulates in the blood in high numbers and rapidly moves into tissues, so blood PCR is almost useless — sensitivity is in the single digits.
PCR is genuinely valuable on the right sample:
- Synovial fluid in Lyme arthritis — sensitivity 70–85%. The best confirmatory test when a knee effusion is tapped.
- Cerebrospinal fluid (CSF) in neuroborreliosis — sensitivity only around 10–30%, so a negative PCR does not rule it out, but a positive is highly specific.
- Skin biopsy of an EM lesion or acrodermatitis chronica atrophicans — very high sensitivity, but rarely needed in practice because the rash is already diagnostic.
A negative PCR on any sample does not exclude Lyme. A positive result on an appropriately chosen sample is highly meaningful.
Culture
Culturing B. burgdorferi from a patient is technically possible on specialized BSK-H medium but is not clinically useful. Culture takes weeks, requires reference-lab conditions, has poor sensitivity except on skin-biopsy material, and is used almost exclusively for research. If a clinician orders a "Lyme culture" on blood, be skeptical of what the lab is actually doing.
CSF Testing for Neuroborreliosis
When Lyme reaches the central nervous system — causing meningitis, radiculitis, cranial neuritis, or encephalopathy — a lumbar puncture is often necessary. See the neuroborreliosis article for the full clinical picture. Four CSF findings build the diagnosis:
- Pleocytosis — an elevated white blood cell count, typically lymphocytic, usually in the range of 10–500 cells/µL.
- Elevated protein — commonly 60–300 mg/dL.
- Normal or mildly low glucose.
- Intrathecal antibody production — this is the key confirmatory finding. The lab measures Borrelia antibodies in both CSF and serum, then calculates a CSF/serum antibody index. An index above 1.0 (some labs use 1.3) indicates antibodies are being produced inside the central nervous system, not simply leaking in from the bloodstream.
PCR on CSF adds specificity but not sensitivity. The antibody index is the workhorse of CNS Lyme diagnosis, especially in Europe where clinical neuroborreliosis is more common.
C6 Peptide ELISA
The C6 peptide ELISA is a single-tier immunoassay that targets a short invariant region of the VlsE protein. It has been extensively validated and offers sensitivity roughly comparable to STTT in early-disseminated and late disease, with a simple one-step workflow. Specificity is slightly lower than two-tier testing, so a positive C6 should generally be confirmed with a standard or modified two-tier algorithm before treatment decisions are made. It can be useful when lab turnaround matters and as one component of MTTT panels.
"Chronic Lyme" Labs to Avoid
This section is going to be blunt, and it is written for patients who are sick, scared, and being told by every mainstream doctor that their labs are "normal." You deserve honesty, not dismissal. But you also deserve to know what the tests you are spending thousands of dollars on actually measure.
Several specialty labs market Lyme panels that do not follow CDC criteria. The most commonly encountered include IGeneX, Galaxy Diagnostics, and Advanced Laboratory Services. Their reports often show bands or findings that sound damning — "positive IgM," "reactive bands 31 and 34," "detected by nanotrap" — and the interpretation paragraph frequently suggests active Lyme infection.
The problems with these panels are real and documented:
- Non-CDC band criteria. Some labs count bands (like 31 kDa/OspA and 34 kDa/OspB) that the CDC explicitly excluded because they cross-react with other organisms. Under their expanded criteria, healthy controls test positive at high rates.
- IgM interpretation past 30 days. Calling a six-month-ill patient "Lyme positive" based on a persistent IgM blot is not biologically sound.
- Unvalidated PCR and "urine antigen" tests. The FDA has warned about unvalidated Lyme urine antigen assays; peer-reviewed validation studies for most of these methods are absent or show very high false-positive rates.
- CD57 natural-killer cell counts. Promoted as a chronic-Lyme biomarker, but the peer-reviewed literature does not support CD57 as a specific indicator of Borrelia infection. Levels fluctuate with countless other factors.
- Cost. These panels typically run $400–$1,500 out of pocket, rarely covered by insurance.
None of this means your symptoms are imagined. Many patients with genuine post-treatment Lyme disease syndrome, ME/CFS, mast cell activation, dysautonomia, or untreated co-infections end up at these labs because nobody else is listening. The problem is not your search for answers. The problem is that a positive result from a lab using non-standard criteria is not the same kind of evidence as a positive CDC-validated test, and long courses of IV antibiotics based on those results carry real harm — Clostridioides difficile infection, line sepsis, fungal bloodstream infection, and gallbladder disease from ceftriaxone have all killed patients in this setting.
If you have already run these tests, bring the report to an infectious disease physician or Lyme-literate academic rheumatologist who will read it honestly with you rather than either rubber-stamping it or dismissing you. You deserve a careful second look, not a shrug.
Seronegative Lyme
Truly seronegative active Lyme disease — infection without detectable antibodies weeks into illness — is rare but real. It occurs most often in patients whose immune systems cannot mount a normal antibody response: those on B-cell-depleting drugs such as rituximab, patients with common variable immunodeficiency, and some post-transplant and HIV-infected patients.
Diagnosis in this setting leans on direct-detection methods: skin-biopsy PCR, synovial-fluid PCR, CSF findings, or characteristic imaging plus clinical picture. Empiric treatment is sometimes justified when the clinical story is strong enough despite negative serology. Outside this narrow immunocompromised context, a truly negative two-tier test weeks into an illness is strong evidence against active Lyme in an immunocompetent adult.
Post-Treatment Serology
This one catches patients repeatedly, and it causes enormous anxiety: antibodies against Borrelia persist for years — often for life — after successful treatment. A positive ELISA or blot six months, two years, or ten years after a cured infection does not mean the bacteria are still there. It simply means your immune system remembers.
The clinical corollary: do not re-test serology to "see if the Lyme is gone." The result cannot answer that question. It will stay positive, and you will be scared for no reason. If you have persistent symptoms after treatment, the evaluation is clinical and focuses on identifying post-treatment Lyme disease syndrome, missed co-infections, or alternative diagnoses — not on re-running antibody panels.
The one exception is CSF antibody index in suspected neuroborreliosis, which can decline after successful treatment and is occasionally used in Europe to monitor response. Even there, it is not a routine test.
Special Populations
Pediatric patients. Children respond to serology similarly to adults, but EM rashes may be more subtle and easier to miss on dark skin or in the scalp. A strong clinical presentation in an endemic region is treated empirically; laboratory diagnosis follows the same two-tier or modified two-tier algorithm.
Pregnancy. Serology is interpreted identically in pregnancy. Early treatment of suspected Lyme in pregnant women is particularly important because untreated maternal Lyme has been associated with adverse pregnancy outcomes. Amoxicillin and cefuroxime are the preferred antibiotics; doxycycline is generally avoided in pregnancy. See the antibiotic protocols article for details.
Immunocompromised patients. Reduced antibody production means higher rates of false-negative serology. Rituximab recipients are the classic example; patients with CVID, active chemotherapy, or advanced HIV are also at risk. Clinicians should have a lower threshold for direct-detection methods (PCR on appropriate samples) and empiric treatment when the picture fits.
Elderly patients. Serology performs well, but coexisting conditions (age-related ANA positivity, chronic infections) increase the rate of nonspecific bands on Western blots. Interpretation should lean on clinical features, not isolated serologic findings.
Key Research Papers
- Mead P, Petersen J, Hinckley A. Updated CDC Recommendation for Serologic Diagnosis of Lyme Disease. MMWR Morb Mortal Wkly Rep. 2019;68(32):703.
- Branda JA, et al. Two-Tiered Antibody Testing for Lyme Disease With Use of 2 Enzyme Immunoassays, a Whole-Cell Sonicate Enzyme Immunoassay Followed by a VlsE C6 Peptide Enzyme Immunoassay. Clin Infect Dis. 2018.
- Lantos PM, et al. Clinical Practice Guidelines by the IDSA, AAN, and ACR: 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1-e48.
- Nocton JJ, Dressler F, Rutledge BJ, Rys PN, Persing DH, Steere AC. Detection of Borrelia burgdorferi DNA by polymerase chain reaction in synovial fluid from patients with Lyme arthritis. N Engl J Med. 1994;330(4):229-234.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on Lyme disease diagnostics, serology interpretation, and direct-detection methods:
- Lyme disease two-tier testing
- Modified two-tier testing for Lyme disease
- Western blot Lyme disease criteria
- CSF Lyme neuroborreliosis and antibody index
- Borrelia burgdorferi PCR in synovial fluid
- Seronegative Lyme disease and immunocompromised hosts
- C6 peptide ELISA for Lyme disease
- Lyme disease serology false positives and cross-reactivity
Connections
- Lyme Neuroborreliosis
- Erythema Migrans Rash
- PTLDS and Chronic Lyme
- Antibiotic Treatment Protocols
- Tick-Borne Co-Infections
- Lyme Disease Overview
- Arthritis
- Prevention and Tick Removal
- Tick Bite First Aid
- Meningitis
- Lyme Carditis
- Peripheral Neuropathy
- Full Body MRI
- Fatigue
- Cat's Claw
- Alpha-Gal Syndrome