Dermatitis Herpetiformis: Celiac of the Skin
Dermatitis herpetiformis (DH) is celiac disease that shows up on your skin instead of — or in addition to — your gut. It is not "a rash that happens in celiac patients." It is the same disease, driven by the same gluten-triggered immune reaction, producing the same tissue transglutaminase antibodies, requiring the same lifelong gluten-free diet. The difference is where the antibody deposits choose to land: in DH, they accumulate in the tiny loops of connective tissue just under the top layer of skin (the dermal papillae), and the result is a maddeningly itchy, blistering eruption that can predate any digestive symptoms by years.
If you have been told "your biopsy was negative for DH" but you still itch every time you eat bread, keep reading — the most common reason the test fails is that it was taken from the wrong spot. This page explains what DH is, how it should be diagnosed, what dapsone does and does not do, why iodine is an under-recognized flare trigger, and why a strict gluten-free diet remains the only cure.
Table of Contents
- What Dermatitis Herpetiformis Is
- What the Rash Looks and Feels Like
- Pathogenesis: Why Gluten Attacks Your Skin
- Diagnosis: Direct Immunofluorescence Done Right
- The Gut You Can't See: Near-Universal Enteropathy
- Dapsone: Fast Relief, Real Risks
- Gluten-Free Diet: The Only Cure
- Iodine Sensitivity and Other Flare Triggers
- Differential Diagnosis: What It Isn't
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
What Dermatitis Herpetiformis Is
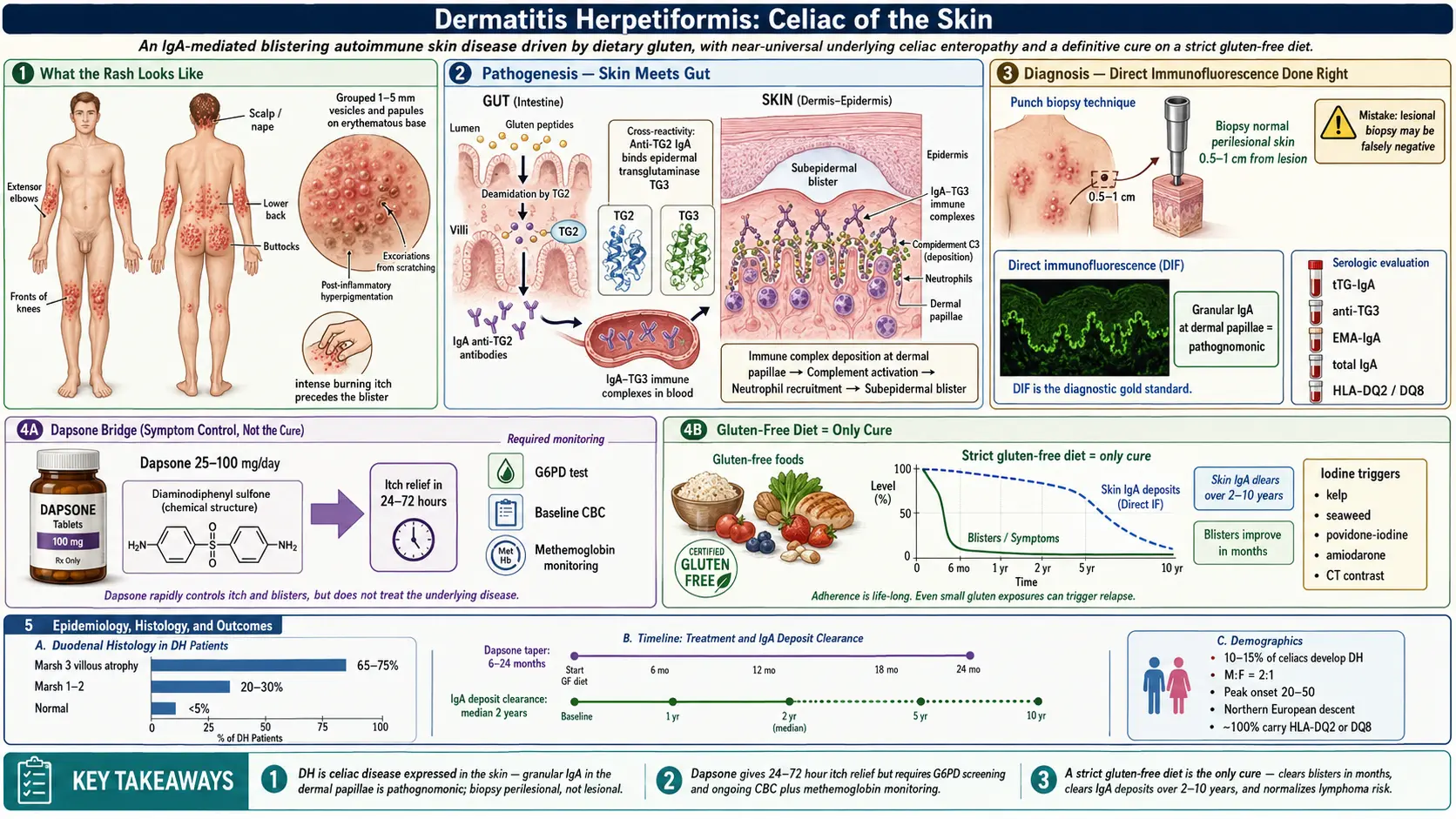
DH is an autoimmune skin disease that occurs almost exclusively in people with celiac disease. Roughly 10–15% of celiac patients develop DH at some point, and essentially 100% of DH patients have underlying celiac enteropathy on small-bowel biopsy — even when they have no stomach pain, no diarrhea, no bloating, nothing at all from the waist down.
The disease was first described by the American dermatologist Louis Duhring in 1884, which is why it is sometimes still called Duhring's disease. "Herpetiformis" refers to the shape of the eruption — grouped vesicles that resemble a herpes simplex outbreak — not any connection to the herpes virus. DH has nothing to do with any viral infection. It is purely immunologic, and the trigger is dietary gluten.
DH is more common in people of Northern European descent, roughly 2:1 in men over women (the reverse of most celiac demographics), and typically appears between ages 20 and 50, though childhood and late-life onset both occur.
What the Rash Looks and Feels Like
The classic DH eruption has five features that, together, are almost diagnostic on sight:
- Location. Symmetric and stereotyped: the extensor surfaces of the elbows, the fronts of the knees, the buttocks, the lower back, the scalp and nape of the neck, and sometimes the shoulders or face. If you draw a line down the middle of your body, DH tends to mirror itself side to side. Palms and soles are almost never involved.
- Lesion type. Small, grouped papules and vesicles (tiny fluid-filled blisters, typically 1–5 mm) on a reddish base. The vesicles are fragile and often scratched open before a doctor ever sees them, leaving crusted erosions, excoriations, and post-inflammatory pigmentation.
- Itch. Intense, burning, stinging itch that frequently precedes the visible blister by hours. Many patients describe scratching a spot raw and then watching a blister form at the same location. Sleep disruption is common.
- Course. Chronic and relapsing. Without treatment, crops of new lesions appear every few days to weeks for years.
- Scarring and pigmentation. Because patients scratch, healed lesions often leave hyperpigmented or hypopigmented spots that take months to fade.
One critical clue: DH almost never presents only on the trunk or only on the face. If the rash spares elbows, knees, and buttocks entirely, DH is unlikely.
Pathogenesis: Why Gluten Attacks Your Skin
The immune story connects the gut and the skin through a single family of enzymes called transglutaminases.
In celiac disease, gluten peptides in the small intestine are modified by tissue transglutaminase 2 (tTG or TG2). In HLA-DQ2 or DQ8 carriers, the immune system misreads this and produces IgA antibodies against tTG2. That is the foundation of classic celiac.
In DH, the dominant antibody target is a closely related enzyme: epidermal transglutaminase (eTG, also called TG3), expressed in the skin. The working model is that antibodies originally raised against tTG2 cross-react with TG3, or that TG3-specific IgA is generated in parallel. Either way, IgA-TG3 immune complexes circulate in the blood and deposit in the dermal papillae — the fingertip-shaped projections of connective tissue just under the epidermis.
Those deposits activate complement (particularly C3) and recruit neutrophils to the tips of the papillae, where they release enzymes that separate the epidermis from the dermis. The result is a microscopic subepidermal blister filled with neutrophils, perfectly located at the top of each papilla. Multiply that by hundreds of papillae across an inflamed patch of skin and you get the clinically visible vesicle.
This is why the diet works: cut off gluten, the gut stops producing the antibody, and over months to years the skin deposits clear and new blisters stop forming.
Diagnosis: Direct Immunofluorescence Done Right
The gold standard for DH diagnosis is direct immunofluorescence (DIF) of perilesional skin. A small punch biopsy (3–4 mm) is taken and stained with a fluorescent antibody against human IgA. In DH, the classic finding is granular IgA deposits along the dermal-epidermal junction, concentrated at the tips of the dermal papillae. This pattern is essentially pathognomonic.
The single most common reason DH is missed: the biopsy was taken from the wrong place. Remember this clearly:
- Biopsy the normal-appearing skin 0.5–1 cm next to an active lesion. This "perilesional" skin still contains the IgA deposits but has not yet been destroyed by the inflammatory cascade.
- Do not biopsy the blister itself. Inside the lesion, neutrophils and enzymes have degraded the IgA, and the DIF will come back falsely negative.
- Do not biopsy a healed or scratched-open crust. Same problem — the antigen is gone.
If your DIF was negative but your story sounds like DH, ask whether the biopsy came from lesional or perilesional skin. If it was lesional, the test needs to be repeated correctly before DH is ruled out.
Supporting blood work. In addition to DIF, order:
- Anti-tissue transglutaminase IgA (tTG-IgA) — positive in most DH patients, though titers are often lower than in classic celiac.
- Anti-epidermal transglutaminase IgA (anti-TG3) — the most specific serum marker for DH, though not available at every lab.
- Anti-endomysial IgA (EMA) — highly specific but labor-intensive.
- Total serum IgA — to rule out selective IgA deficiency, which can produce falsely negative IgA-based celiac tests. See the serology testing article for interpretation details.
- HLA-DQ2 and DQ8 typing — essentially 100% of DH patients carry one of these haplotypes. A negative result argues strongly against DH. See HLA-DQ2/DQ8 testing.
Do not start a gluten-free diet before testing. Serologies and skin DIF both become less reliable within weeks of eliminating gluten.
The Gut You Can't See: Near-Universal Enteropathy
If your DH is confirmed, you almost certainly have celiac small-bowel damage whether or not you have GI symptoms. Studies using duodenal biopsy in DH cohorts consistently find:
- ~65–75% have frank villous atrophy (Marsh 3) identical to classic celiac.
- ~20–30% have milder changes (Marsh 1–2): increased intraepithelial lymphocytes or crypt hyperplasia.
- Only a tiny minority have entirely normal small-bowel histology, and even those patients still respond to a gluten-free diet.
See the endoscopy and Marsh classification article for what those grades mean. The practical point: you do not necessarily need a duodenal biopsy to diagnose DH (skin DIF is enough), but you do need the same nutritional and bone-health surveillance as any celiac patient because the underlying malabsorption is there. See nutritional deficiencies and bone health for the work-up.
It also cuts the other direction: skin symptoms often predate GI symptoms by years or decades. Many DH patients describe chasing a mysterious itchy rash from dermatologist to dermatologist, being told it is eczema or scabies, and only discovering celiac when a sharp clinician finally orders DIF.
Dapsone: Fast Relief, Real Risks
A gluten-free diet is the definitive treatment, but it takes months to years to fully quiet the skin. In the meantime, the itch is unbearable. Dapsone (diaminodiphenyl sulfone) is the standard bridge therapy. It does not treat the underlying celiac disease — it suppresses the neutrophil-driven inflammation that forms each blister. Many patients notice dramatic itch relief within 24–72 hours of their first dose.
Typical dosing. Start at 25–50 mg orally once daily, titrated to the lowest dose that controls symptoms. Most adults settle at 50–100 mg/day, though some need up to 150–200 mg transiently. Children are dosed by weight (around 0.5–2 mg/kg/day). Once the gluten-free diet has worked for a year or two, the dapsone dose is tapered and usually stopped entirely.
Required before the first dose.
- G6PD enzyme level. Dapsone triggers acute hemolytic anemia in patients with glucose-6-phosphate dehydrogenase deficiency. Never start dapsone without documenting a normal G6PD level. The test is a simple blood draw, $20–$100, covered by insurance.
- Baseline CBC with differential. To detect any pre-existing anemia or low white count.
- Baseline liver function tests. Dapsone can cause hepatitis.
Required during therapy.
- CBC. Weekly for the first month, every 2 weeks for the next two months, then every 3–6 months. Watch for hemolytic anemia and, rarely, agranulocytosis (a sudden drop in neutrophils, usually in the first three months).
- Methemoglobin monitoring. Dapsone oxidizes hemoglobin iron from ferrous to ferric, producing methemoglobin that cannot carry oxygen. Mild methemoglobinemia (2–5%) is nearly universal and usually tolerated. Higher levels cause bluish lips, headache, fatigue, and shortness of breath. Any new dyspnea on dapsone needs a methemoglobin level and often a dose reduction. Severe cases are treated with IV methylene blue.
- LFTs every 3–6 months.
Other side effects to know. Peripheral neuropathy (usually motor, dose-dependent, reversible), dapsone hypersensitivity syndrome (fever, rash, hepatitis, eosinophilia — within the first 6 weeks; requires immediate drug cessation), and rarely psychosis.
If dapsone is not tolerated, alternatives include sulfapyridine (harder to obtain in the U.S.) and sulfasalazine. Topical steroids and antihistamines help with itch but do not control the eruption on their own.
Gluten-Free Diet: The Only Cure
A strict, lifelong gluten-free diet is the definitive treatment for DH. It is the only intervention that addresses the underlying antibody production. On a clean diet:
- New blister formation typically slows within weeks to a few months.
- Dapsone requirements drop progressively over 6–24 months and most patients come off the drug entirely.
- Full clearance of cutaneous IgA deposits on DIF takes 2–10 years, with a median around 2 years. The skin memory of this disease is long.
- Intestinal recovery parallels the skin recovery.
- The elevated risk of small-bowel lymphoma associated with untreated DH normalizes with strict adherence.
"Strict" means strict. Even trace gluten — a few crumbs from a shared toaster, oats processed in a wheat facility, a soy sauce splash on restaurant sushi — can reactivate the skin deposits and bring blisters back. Many DH patients are measurably more sensitive to cross-contamination than classic celiac patients are. See the gluten-free diet practical guide for kitchen setup, restaurant strategy, reading labels, and the surprising places gluten hides (lip balm, communion wafers, certain medications, beer, malt vinegar, some soy sauces, seitan, barley-based "natural flavor").
If the rash relapses after months of apparent control, the first question is always "what changed in the diet?" — not "do I need more dapsone?" A food diary for two weeks plus a repeat tTG-IgA usually identifies the breach.
Iodine Sensitivity and Other Flare Triggers
DH has an unusual and under-appreciated trigger: dietary iodine. Iodine does not cause DH — gluten does — but in someone with established DH, a sudden iodine load can precipitate a flare even on a clean gluten-free diet. The mechanism is not fully understood; iodine appears to act as a non-specific amplifier of the neutrophil response in skin already primed by IgA deposits.
High-iodine sources to be aware of if you flare without an obvious gluten exposure:
- Large amounts of seaweed, kelp, nori, or kelp-based supplements.
- Iodine-containing contrast used in CT scans or angiography.
- Povidone-iodine (Betadine) applied to large skin surfaces.
- Certain cough expectorants containing potassium iodide.
- Amiodarone (a cardiac antiarrhythmic with very high iodine content).
You do not need an iodine-restricted diet once you are stable. Normal iodized salt and ordinary seafood intake are fine. But if you are flaring, or if you have a CT with contrast scheduled, it is worth mentioning the DH to your physician so unexpected worsening is not a mystery.
Other triggers reported in case series include NSAIDs (occasional), stress, and occasionally hormonal shifts.
Differential Diagnosis: What It Isn't
Several common skin conditions look enough like DH to delay diagnosis. The most frequent imposters:
- Scabies. Also intensely itchy, also involves the buttocks and extensor surfaces. But scabies favors finger webs, wrists, and genitalia; burrows are visible under magnification; and household contacts also itch. Scrape and microscopy distinguish the two.
- Atopic dermatitis (eczema). Itchy, chronic, symmetric — but typically favors flexural surfaces (inside of elbows and knees), not extensors. No vesicles. Personal or family atopy history usually present.
- Bullous pemphigoid. An autoimmune subepidermal blistering disease of older adults (usually 70+). Blisters are larger and tenser, itch is less prominent, and DIF shows linear IgG (not granular IgA) at the basement membrane.
- Linear IgA bullous dermatosis. Similar blistering, but DIF shows linear IgA rather than granular IgA in the papillae. Not associated with celiac.
- Papular urticaria, insect bite reactions, and folliculitis. Usually more asymmetric and more episodic.
- Neurotic excoriations. Self-induced scratching without an underlying eruption; biopsy shows only excoriation.
Any patient whose "eczema" concentrates on elbows, knees, and buttocks, itches violently, and has not responded to topical steroids deserves a DH work-up.
Key Research Papers
- Reunala T, Salmi TT, Hervonen K, Kaukinen K, Collin P. Dermatitis herpetiformis: a common extraintestinal manifestation of coeliac disease. Nutrients. 2018;10(5):602.
- Salmi TT. Dermatitis herpetiformis. Clin Exp Dermatol. 2019;44(7):728–731.
- Caproni M, Antiga E, Melani L, Fabbri P. Guidelines for the diagnosis and treatment of dermatitis herpetiformis. J Eur Acad Dermatol Venereol. 2009;23(6):633–638.
- Zone JJ. Skin manifestations of celiac disease. Gastroenterology. 2005;128(4 Suppl 1):S87–S91.
- Sárdy M, Kárpáti S, Merkl B, Paulsson M, Smyth N. Epidermal transglutaminase (TGase 3) is the autoantigen of dermatitis herpetiformis. J Exp Med. 2002;195(6):747–757.
- Fry L. Dapsone in dermatitis herpetiformis — a historical and clinical review. Br J Dermatol. 1985;112(1):124. (classic review of dapsone use in DH)
PubMed Topic Searches
For deeper reading, the following PubMed searches return current peer-reviewed work on DH biology, diagnosis, and management:
- Dermatitis herpetiformis review articles
- DH and direct immunofluorescence technique
- Epidermal transglutaminase (TG3) autoantigen
- Dapsone therapy in dermatitis herpetiformis
- Gluten-free diet outcomes in DH
- DH and iodine sensitivity
- DH and small-bowel enteropathy
- HLA-DQ2/DQ8 in DH
- DH and lymphoma risk on and off diet
- Dapsone safety: G6PD and methemoglobin monitoring
Connections
- Dermatitis Herpetiformis (Dermatology) — the same disease written as a dermatology monograph — Duhring’s 1884 description, epidemiology and risk factors, the histopathology, and long-term monitoring.
- Celiac Disease Overview
- Gluten-Free Diet: A Practical Guide
- Nutritional Deficiencies and Bone Health
- Celiac Serology Testing: tTG, DGP, EMA
- Endoscopy, Biopsy, and Marsh Classification
- HLA-DQ2 and HLA-DQ8 Genetic Testing
- Non-Celiac Gluten Sensitivity
- Associated Autoimmune Conditions
- Refractory Celiac Disease and EATL
- Hashimoto's Thyroiditis
- Psoriasis
- Iodine
- Gut-Brain Axis
- Vitamin D3