Non-Celiac Gluten Sensitivity (NCGS)
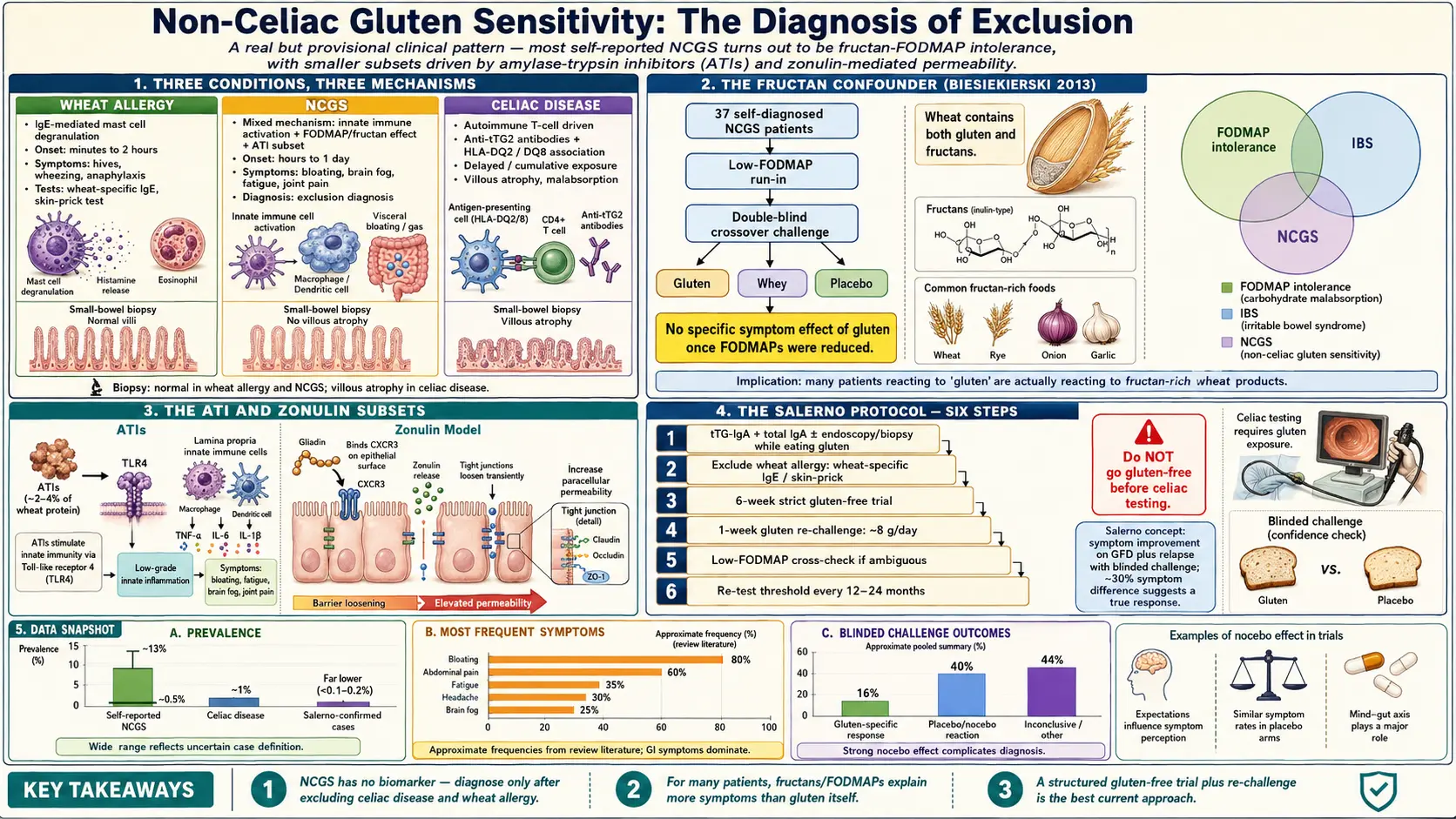
Table of Contents
- What NCGS Is (and What It Is Not)
- The Salerno Experts' Criteria (2014)
- Symptom Profile
- How Common Is It? The 0.5-to-10% Problem
- The Monash Fructan Finding — Why "Gluten" May Not Be Gluten
- The ATI Hypothesis — A Real Non-Celiac Wheat Reaction
- Zonulin and Leaky Gut — The Emerging Subset
- How to Diagnose NCGS — The Salerno Protocol
- Self-Trialing Risks
- Wheat Allergy vs NCGS vs Celiac
- Why the Stakes Are Lower Than Celiac
- Overlap with MCAS, Hashimoto's, and Fibromyalgia
- When "Better Off Gluten" Is Really "Less Ultra-Processed Food"
- Practical Stance
- Key Research Papers
- Connections
- Featured Videos
What NCGS Is (and What It Is Not)
Non-celiac gluten sensitivity is the name given to people who feel clearly worse when they eat gluten-containing foods (wheat, barley, rye), yet do not have celiac disease and do not have a classical wheat allergy. It is a diagnosis of exclusion. Your gastroenterologist cannot order a blood test to confirm it, cannot biopsy for it, and cannot point to a single validated biomarker. NCGS exists as a clinical pattern — an honest shrug that says: "Something about wheat bothers this patient, but it is not the two things we know how to measure."
For decades, skeptical physicians dismissed NCGS as anxiety or fad dieting. That has shifted. Gastroenterology now broadly accepts NCGS as a real phenomenon — but also accepts that the label is a provisional umbrella over several different biological processes, and that many people who believe they have NCGS actually have something else entirely. The practical task is to sort out which group you fall into, because the answer changes what you need to avoid, what you can re-introduce safely, and how strictly you have to read labels.
The clean negative definition: NCGS is not celiac disease (no tissue transglutaminase antibodies, no villous atrophy on duodenal biopsy while eating gluten), it is not wheat allergy (no wheat-specific IgE, negative skin prick test, no hives or anaphylaxis on exposure), and it is not irritable bowel syndrome alone (though these can coexist). What remains is a patient whose gut and nervous system change state predictably on and off wheat.
The Salerno Experts' Criteria (2014)
In 2014 an international panel convened in Salerno, Italy, to agree on a minimum standard for diagnosing NCGS. The published consensus — Catassi and colleagues, 2015 — is still the reference framework and is usually called the Salerno Experts' Criteria. The criteria boil down to three requirements:
- Celiac disease must be ruled out while the patient is still eating gluten. That means tissue transglutaminase IgA (tTG-IgA) must be negative and duodenal biopsy — if performed — must show a normal Marsh classification (Marsh 0, normal villi). A gluten-free trial before this step sabotages the workup, because both serology and biopsy can normalize within weeks off gluten.
- Wheat allergy must be ruled out. Skin prick test and wheat-specific IgE negative.
- Symptoms must respond to gluten withdrawal and recur on gluten re-challenge in a structured way — ideally double-blind and placebo-controlled, though in everyday practice a careful open challenge with a symptom diary is more realistic.
The Salerno protocol also specifies a symptom-scoring instrument (a modified Gastrointestinal Symptom Rating Scale plus extra-intestinal items), a six-week gluten-free run-in, and a one-week re-challenge with at least 8 g of gluten per day (roughly two slices of wheat bread) against a placebo of gluten-free bread. A symptom-score change of at least 30% between arms is considered positive. Few patients ever get this full protocol outside research studies, but understanding the logic is useful — it explains why your doctor is not satisfied when you say "I just know gluten wrecks me."
Symptom Profile
NCGS symptoms fall into two camps, and most patients have some of each.
Gastrointestinal. Bloating is the near-universal complaint — a distended belly a few hours after a wheat meal, often visible enough that patients describe "pregnancy belly" or having to unbutton their pants. Abdominal pain, cramping, and altered bowel habits are common: some patients run toward diarrhea, others toward constipation, and a large subset alternate between the two. Nausea, reflux, and excess gas round out the picture. In pure form, this overlaps heavily with IBS — and that overlap is not accidental (see the Biesiekierski section below).
Extra-intestinal. This is where NCGS diverges most clearly from plain IBS and becomes interesting. Reported symptoms include:
- Brain fog — slowed thinking, word-finding difficulty, a feeling of being wrapped in cotton that clears within days off gluten.
- Fatigue — disproportionate to sleep, often worse a few hours after a wheat meal.
- Headache and migraine.
- Joint and muscle pain — diffuse, migratory, without swelling or measurable inflammation.
- Dermatitis — eczema-like rash, sometimes prurigo or an urticaria-like picture (distinct from dermatitis herpetiformis, which is a celiac-specific rash).
- Anxiety and low mood — real and reproducible in some patients, likely gut-brain axis driven.
- Numbness or tingling in hands and feet in a minority.
Symptom onset is typically hours to a day after a gluten exposure and resolves within a few days off gluten. This fast-on/fast-off pattern is one reason NCGS presents differently from celiac, where damage and symptoms accumulate over months.
How Common Is It? The 0.5-to-10% Problem
Prevalence estimates for NCGS range from under 1% to more than 10% of the adult population depending on how the question is asked. Self-report surveys — "Do you feel worse when you eat gluten?" — yield the 6-to-13% range. Rigorous double-blind placebo-controlled challenge studies shrink that number dramatically, often to under 20% of the self-reported group — implying a true biological NCGS prevalence closer to 1–2%.
That is a twenty-fold gap between what people report and what challenge testing confirms. Two honest interpretations coexist:
- A large fraction of self-reported NCGS is non-gluten wheat reactivity (FODMAPs, ATIs) or a nocebo/expectation effect.
- Challenge protocols are short, artificial, and probably miss real but delayed reactions.
Both are partially true. The clinical consequence is humility: if you feel better off gluten, that is meaningful, but the reason you feel better may not be gluten.
The Monash Fructan Finding — Why "Gluten" May Not Be Gluten
The single most important study in the NCGS literature is Biesiekierski and colleagues, published in Gastroenterology in 2013, from the Monash University FODMAP research group. They took 37 patients who had already self-diagnosed as NCGS, placed them on a low-FODMAP diet for two weeks, and then challenged them — double-blind, crossover — with gluten, whey (control), or low-FODMAP placebo.
The result surprised the field. On the low-FODMAP background, almost no one reacted specifically to gluten. Symptoms improved on the low-FODMAP run-in regardless of whether gluten was reintroduced later. The conclusion was that the wheat sensitivity reported by this group was driven primarily by fructans — short-chain fermentable carbohydrates concentrated in wheat, rye, onion, and garlic — rather than by gluten itself.
Wheat contains both. When a patient cuts gluten-containing grains, they simultaneously cut fructans. It has always been confounded. If the real trigger is fructans, then the correct diagnosis is IBS with fructan intolerance, and the correct intervention is a structured low-FODMAP diet, not lifelong gluten avoidance. That distinction matters enormously — fructan tolerance can be rebuilt in stages using a reintroduction protocol, whereas people who believe themselves gluten-sensitive often police traces of gluten for life.
A practical tell: if small amounts of garlic, onion, or inulin-fortified foods also cause bloating, fructans are a strong suspect. If 100% spelt sourdough (long-fermented, naturally fructan-reduced) is tolerated while standard wheat bread is not, that also points at fructans, because long fermentation degrades fructans but does not remove gluten.
The ATI Hypothesis — A Real Non-Celiac Wheat Reaction
A smaller subset of patients appears to react to wheat even when FODMAPs are controlled. The leading candidate molecules are amylase-trypsin inhibitors (ATIs) — plant defense proteins that make up roughly 2–4% of the protein in modern wheat. Detlef Schuppan's laboratory at Johannes Gutenberg University in Mainz has shown that ATIs activate Toll-like receptor 4 (TLR4) on intestinal immune cells, triggering a low-grade innate immune response without the autoimmune T-cell cascade of celiac.
This matters because modern hexaploid bread wheat has been bred for high ATI content (ATIs contribute to pest resistance and baking properties), and because it offers a plausible mechanism distinct from both celiac and FODMAP intolerance. ATI-driven inflammation could explain the extra-intestinal symptoms — joint pain, brain fog, fatigue — that a simple FODMAP story struggles with.
ATIs are present in wheat, rye, and barley but are low in einkorn, spelt (to a lesser extent), rice, oats, and gluten-free grains. Some patients who react to modern wheat tolerate einkorn or traditional long-fermented sourdoughs, which is consistent with an ATI mechanism rather than a gluten-peptide mechanism.
Zonulin and Leaky Gut — The Emerging Subset
Alessio Fasano's group at Massachusetts General Hospital has proposed that a subset of NCGS patients show elevated serum zonulin, a regulator of intestinal tight junctions, and increased intestinal permeability on lactulose/mannitol testing. In their model, gluten (specifically the gliadin peptide) binds the CXCR3 receptor on gut epithelial cells and transiently opens tight junctions in susceptible individuals, allowing food antigens and bacterial products into the lamina propria where they drive low-grade systemic inflammation.
The zonulin story is biologically appealing and fits patient reports of systemic symptoms, but the evidence is still preliminary, zonulin assays have reproducibility problems, and permeability testing is not a routine clinical tool. It is a hypothesis worth watching, not a diagnostic test worth ordering.
How to Diagnose NCGS — The Salerno Protocol
If you suspect NCGS, the sequence matters. Do these steps in order.
Step 1 — Stay on gluten and rule out celiac first. Before you cut a single slice of bread, get tTG-IgA and total IgA (to exclude IgA deficiency, which invalidates the tTG test). If those are suspicious or borderline, add deamidated gliadin peptide antibodies (DGP-IgG) and endomysial antibodies (EMA). If any serology is positive, proceed to upper endoscopy with four to six duodenal biopsies plus one or two from the bulb while still eating gluten. See the serology article and endoscopy article. This step is non-negotiable. Going gluten-free first is the single most common mistake and it can cost you a definitive diagnosis for years.
Step 2 — Rule out wheat allergy. Allergist referral for wheat skin prick and specific IgE, especially if you have any history of hives, throat tightness, or exercise-induced anaphylaxis after eating wheat.
Step 3 — Structured six-week gluten-free trial. Strict elimination of all wheat, barley, and rye (and, to be safe, contaminated oats) for six full weeks. Keep a daily symptom diary rated 0–10 across bloating, pain, stool form (Bristol 1–7), fatigue, brain fog, headache, joint pain, and mood. Do not change other variables — no new supplements, no sudden workout plan, no low-FODMAP overlay yet. You want to isolate the gluten variable.
Step 4 — Gluten re-challenge. After six weeks of clear benefit, re-introduce gluten at roughly 8 g per day (two to three slices of regular wheat bread, or equivalent) for up to a week. The Salerno protocol recommends double-blind placebo-controlled challenge with special baked goods; in the real world, an open challenge with the same symptom diary is acceptable. A clear recurrence of symptoms within a week supports NCGS.
Step 5 — If ambiguous, do a low-FODMAP cross-check. If the gluten-free benefit was modest or if you also react to garlic, onion, apples, and legumes, trial a structured low-FODMAP diet (ideally with a registered dietitian). If your symptoms resolve on low-FODMAP regardless of gluten, the diagnosis is IBS with fructan-dominant intolerance, not NCGS.
Step 6 — Re-test periodically. Unlike celiac, NCGS is not necessarily lifelong. Every 12–24 months, consider a controlled re-introduction to see whether your threshold has shifted. Some patients tolerate small amounts again, particularly if gut health is otherwise improved.
Self-Trialing Risks
The most important practical warning: do not go gluten-free before celiac testing. A few weeks off gluten can normalize tTG-IgA and begin healing duodenal villi. If your celiac workup happens after that, it will come back falsely reassuring, and if you have true celiac you will walk around with ongoing silent damage — to bone density, micronutrient absorption, and long-term cancer risk — while believing you have merely "non-celiac sensitivity."
If you have already gone gluten-free and now want definitive testing, the only path is a gluten challenge: eating at least 3 g of gluten daily (one to two slices of wheat bread) for 6–8 weeks before serology and biopsy. This is miserable for someone who knows wheat makes them sick, but it is the only way to reach a diagnostic answer. An alternative in ambiguous cases is HLA-DQ2/DQ8 genetic testing — a negative result essentially excludes celiac and spares you the challenge; a positive result is consistent with celiac but does not confirm it, since 30–40% of the general population carries these haplotypes without disease. See the HLA-DQ2/DQ8 article.
Other self-trial traps:
- The "gluten-free aisle" substitution. Replacing regular bread with gluten-free bread, cookies, and pasta often adds refined starches, gums, and emulsifiers. If you feel better, it may be because you are eating less wheat-based ultra-processed food, not because gluten was the villain.
- Placebo and nocebo. Blinded challenge studies reliably show placebo responses in the 30–40% range. Expectation is powerful. This does not mean your symptoms are imaginary — it means the causal attribution may be wrong.
- Missing a real diagnosis. A gluten-free diet can mask symptoms of celiac, microscopic colitis, SIBO, bile acid malabsorption, pancreatic insufficiency, lactose intolerance, or inflammatory bowel disease — each of which has specific treatments you would be delaying.
Wheat Allergy vs NCGS vs Celiac
These three conditions get collapsed in everyday speech but are biologically distinct. Knowing the differences helps you explain your situation to family, restaurants, and skeptical clinicians.
| Feature | Wheat Allergy | NCGS | Celiac Disease |
|---|---|---|---|
| Mechanism | IgE-mediated allergy | Innate immune / FODMAP / ATI (mixed) | Autoimmune (T-cell, tTG, HLA-DQ2/DQ8) |
| Onset after exposure | Minutes to 2 hours | Hours to a day | Days to years of cumulative damage |
| Hallmark symptoms | Hives, wheeze, swelling, anaphylaxis | Bloating, brain fog, fatigue, joint pain | Diarrhea, weight loss, deficiencies, or silent |
| Diagnostic test | Skin prick, wheat-specific IgE | Exclusion + structured challenge | tTG-IgA, DGP, EMA, duodenal biopsy |
| Villous atrophy? | No | No | Yes (Marsh 3) |
| Cross-contamination risk | High (trace can trigger anaphylaxis) | Low (symptoms dose-dependent) | High (20 ppm threshold, silent damage) |
| Long-term complications | Anaphylaxis if not avoided | None clearly established | Osteoporosis, anemia, lymphoma, infertility |
| Strict 20 ppm required? | Depends on threshold | No | Yes |
| Reintroduction possible? | Rarely, under oral immunotherapy | Yes, periodically | No, lifelong |
Why the Stakes Are Lower Than Celiac
This is one of the most important practical points in the whole conversation. NCGS, as currently understood, does not cause villous atrophy, nutrient malabsorption, demonstrable bone density loss, or the increased small-bowel lymphoma risk seen in untreated celiac disease. The nearest long-term data, including Lebwohl and colleagues' 2015 BMJ analysis and subsequent cohort work, suggest that self-reported gluten avoiders without celiac do not develop those complications.
The practical implications for someone with confirmed NCGS are substantial:
- The 20 parts-per-million cross-contamination threshold that defines "gluten-free" for celiac patients is not strictly required for NCGS. Most NCGS patients tolerate trace cross-contamination without symptoms.
- You generally do not need separate toasters, dedicated cutting boards, or deep cleaning of shared cookware.
- You can eat at restaurants that cannot guarantee a celiac-safe kitchen, as long as the dish itself is gluten-free.
- Periodic small exposures (a slice of wedding cake, a communion wafer, a bite of your kid's sandwich) do not accumulate long-term damage.
- You do not need annual serology monitoring or follow-up endoscopy.
This is emphatically not permission to ignore how you feel. It is permission to calibrate strictness to symptoms rather than to the much higher celiac safety standard.
Overlap with MCAS, Hashimoto's, and Fibromyalgia
NCGS rarely travels alone. Three overlaps are worth knowing.
Mast Cell Activation Syndrome (MCAS). Wheat is a histamine liberator — it does not contain high histamine itself, but it can prompt mast cells to degranulate in susceptible people. Patients with MCAS often describe "gluten reactions" that on closer inspection are histamine reactions to wheat, fermented sauces, or aged cheeses. If your NCGS symptoms include flushing, itching, palpitations, or post-meal urticaria, ask an allergist about MCAS workup. Treatment (H1/H2 antihistamines, mast cell stabilizers) can dramatically shrink food sensitivity lists.
Hashimoto's thyroiditis. Patients with autoimmune thyroid disease often report feeling better on a gluten-free or grain-free diet. Proposed mechanisms include molecular mimicry between gliadin and thyroid peroxidase, and shared HLA-DQ2/DQ8 susceptibility. The evidence is mixed — clear for coexisting celiac (which is more common in Hashimoto's patients than in the general population), less clear for NCGS alone. Many Hashimoto's patients elect a trial elimination anyway and document the effect on TPO antibodies and symptoms. See Hashimoto's thyroiditis and the AIP and gluten elimination deep dive.
Fibromyalgia and chronic fatigue. A meaningful minority of fibromyalgia patients report substantial improvement in widespread pain and fatigue on a gluten-free diet even in the absence of celiac. Small uncontrolled trials support this; rigorous blinded trials are sparse. The honest framing is: worth a structured six-week trial, not worth expensive branded gluten-free products if no benefit appears.
When "Better Off Gluten" Is Really "Less Ultra-Processed Food"
Here is an uncomfortable but commonly true explanation for why people feel better on a gluten-free diet. The Standard American Diet is dominated by wheat-based ultra-processed food: breakfast cereals, packaged bread, crackers, cookies, pastries, pasta, pizza, frozen meals, fast-food buns. When you "go gluten-free" and do the job seriously, you typically replace that category with whole foods — rice, potatoes, vegetables, eggs, meat, fish, fruit — because the gluten-free processed substitutes are expensive and often unsatisfying. The actual change in your diet is not the removal of a single protein. It is the removal of a large block of refined carbohydrate, industrial emulsifiers, seed oils, and caloric density.
If that is what is really happening, two predictions follow. First, you will feel as good on a whole-food diet that includes traditionally prepared wheat (sourdough, pasta made fresh, plain bread eaten with protein and vegetables) as you do on a gluten-free diet of whole foods. Second, a "gluten-free Oreo" diet will not feel any better than a regular Oreo diet. Many patients discover this when they start eating gluten-free snack foods regularly and find their symptoms creep back.
This is not an argument against gluten avoidance — it is an argument for clean experimental design. If a structured trial with a careful symptom diary shows a clear gluten effect independent of overall diet quality, believe it. If the trial is muddy, suspect the refined-carbohydrate variable.
Practical Stance
A reasonable summary of where to stand if you suspect NCGS:
- Always rule out celiac first. On a gluten-containing diet. No exceptions.
- Rule out wheat allergy if you have ever had hives, wheeze, or throat tightness with wheat.
- Run a clean six-week gluten-free trial with a daily symptom diary. Do not change other variables.
- Re-challenge deliberately. Without the challenge step, you do not have a diagnosis, you have a hypothesis.
- If the picture is muddy, trial low-FODMAP. Many NCGS diagnoses are really fructan-dominant IBS and respond better to a structured FODMAP reintroduction than to lifelong gluten avoidance.
- Calibrate strictness to symptoms. You are not celiac. Trace cross-contamination is not silently harming you. Adjust your social and travel life accordingly.
- Re-test every year or two. Tolerance can shift as gut health improves.
- Watch for overlapping diagnoses — MCAS, Hashimoto's, fibromyalgia, SIBO — which may be the actual driver or a co-driver of your symptoms.
- Do not assume gluten-free packaged food is healthier. Often it is less filling, more processed, and worse for blood sugar than a whole-food diet that includes modest amounts of traditionally prepared wheat.
Key Research Papers
- Catassi C, et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts' Criteria. Nutrients. 2015;7(6):4966-77.
- Biesiekierski JR, et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology. 2013;145(2):320-8.
- Sapone A, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012;10:13.
- Lebwohl B, et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: prospective cohort study. BMJ. 2017;357:i1892.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on NCGS biology, diagnosis, and overlap with IBS and autoimmune disease:
- Non-celiac gluten sensitivity and the Salerno criteria
- NCGS double-blind placebo-controlled challenge studies
- Wheat fructans, FODMAPs, and IBS
- Amylase-trypsin inhibitors, wheat, and TLR4 activation
- Zonulin, intestinal permeability, and gluten
- NCGS extra-intestinal symptoms and brain fog
- Gluten-free diet and Hashimoto's thyroiditis
- Gluten challenge protocols for celiac diagnosis
Connections
- Celiac Disease Overview
- Gluten-Free Diet: A Practical Guide
- Celiac Serology Testing: tTG, DGP, EMA
- Endoscopy, Biopsy, and Marsh Classification
- HLA-DQ2 and HLA-DQ8 Genetic Testing
- Nutritional Deficiencies and Bone Health
- Associated Autoimmune Conditions
- MCAS
- Hashimoto's Thyroiditis
- AIP and Gluten Elimination
- Irritable Bowel Syndrome
- Low-FODMAP Diet for IBS
- Elimination Diet
- SIBO
- Dermatitis Herpetiformis
- Refractory Celiac and EATL