MASLD (Fatty Liver Disease) — Formerly NAFLD
If you arrived here searching for NAFLD, non-alcoholic fatty liver disease, fatty liver, or NASH, you are in the right place. These are all names for the condition now formally called MASLD — metabolic dysfunction-associated steatotic liver disease. In 2023, the world's liver societies retired the old names: NAFLD became MASLD, and its inflammatory form NASH became MASH (metabolic dysfunction-associated steatohepatitis). The disease did not change. The name did — and the new name finally says what the illness actually is.
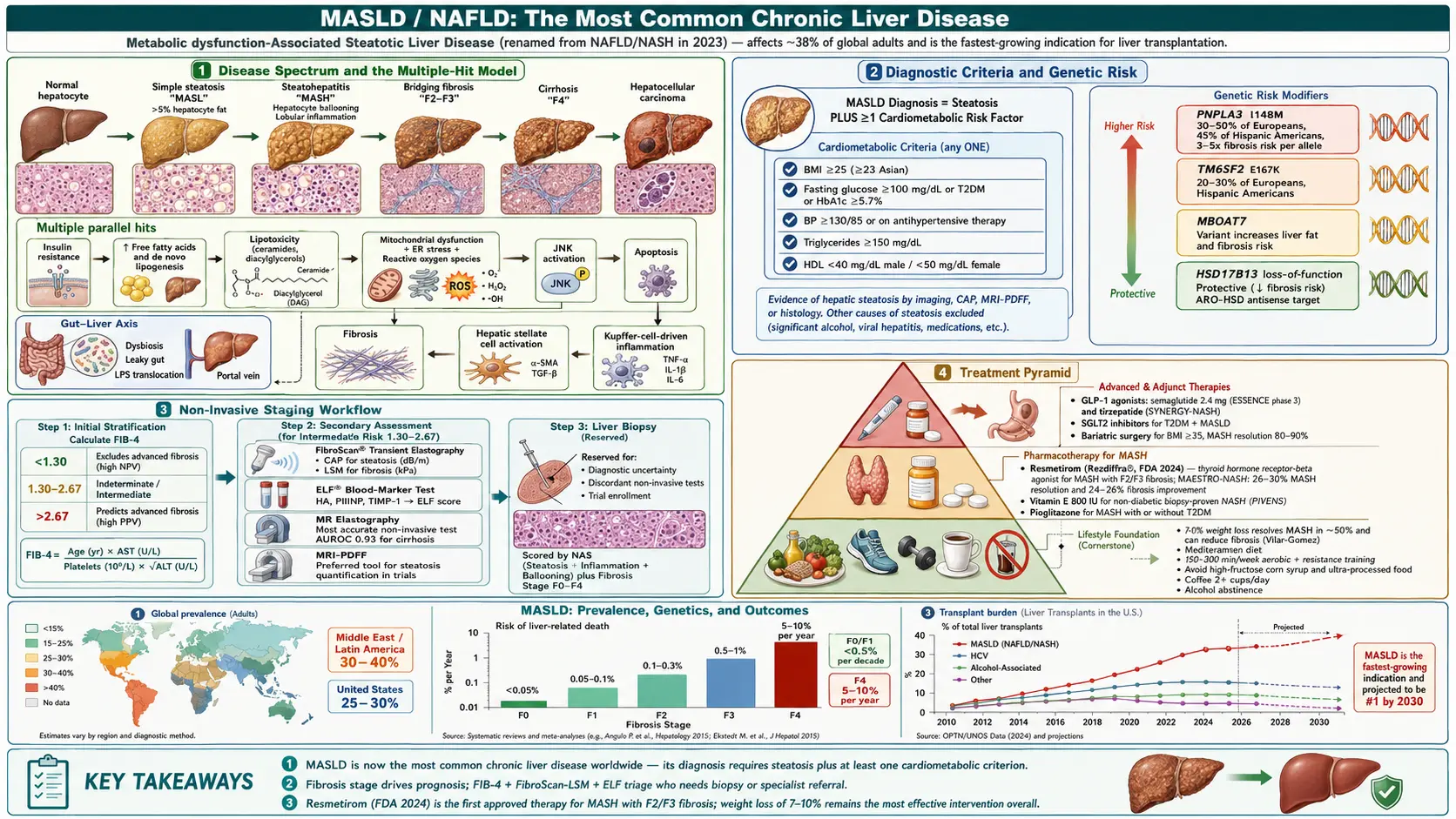
MASLD means excess fat stored inside liver cells (steatosis, affecting more than 5% of hepatocytes) in a person who has at least one cardiometabolic risk factor — extra weight, high blood sugar, high blood pressure, high triglycerides, or low HDL. It is the most common chronic liver disease on earth. Most people who have it do not know, because for years it causes no symptoms at all.
Table of Contents
- The 2023 Name Change: NAFLD → MASLD
- The Disease Spectrum
- Pathophysiology: The Multiple-Hit Model
- Epidemiology
- Risk Factors and Genetics
- Symptoms and Clinical Presentation
- Diagnosis, FIB-4, and Elastography
- Treatment: Weight Loss, Diet, and Exercise
- Drug Treatment: Resmetirom and GLP-1s
- Complications
- Prognosis and Surveillance
- Prevention
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
1. The 2023 Name Change: NAFLD → MASLD
In June 2023, a multi-society Delphi consensus — coordinated by the American Association for the Study of Liver Diseases (AASLD), the European Association for the Study of the Liver (EASL), the Asian Pacific Association for the Study of the Liver (APASL), ALEH, and dozens of allied organizations — formally replaced the old vocabulary. This is the single most important thing to understand about this disease right now, because it changes what you will read, what your doctor writes in your chart, and what you should search for.
The old names and the new ones
- NAFLD (non-alcoholic fatty liver disease) → MASLD (metabolic dysfunction-associated steatotic liver disease)
- NASH (non-alcoholic steatohepatitis) → MASH (metabolic dysfunction-associated steatohepatitis)
- NAFL (simple fatty liver, no inflammation) → MASL (metabolic dysfunction-associated steatotic liver)
Why the name changed
The rename was not cosmetic. It fixed two real problems with the old label:
- "Non-alcoholic" defined the disease by what it was not. Naming an illness for a substance the patient is not consuming is a diagnosis of exclusion dressed up as a diagnosis. It told you nothing about the mechanism, it pushed clinicians to think of the liver in isolation, and it made the condition sound like a lesser cousin of alcoholic liver disease rather than a metabolic disease in its own right.
- The word "fatty" was judged stigmatising. Patient advocacy groups involved in the consensus reported that the term was experienced as blaming and shaming, and that stigma discourages people from seeking care for a disease that is silent, common, and treatable when caught early.
The new name does the opposite: it names the actual driver — metabolic dysfunction. MASLD is now a diagnosis of inclusion: you must have hepatic steatosis plus at least one cardiometabolic criterion. It is something you positively have, not something you merely fail to be.
The five cardiometabolic criteria
To diagnose MASLD, an adult needs steatosis on imaging or biopsy plus at least one of the following:
- BMI ≥25 kg/m² (≥23 kg/m² in Asian populations), or waist circumference >94 cm (men) / >80 cm (women)
- Fasting glucose ≥100 mg/dL, 2-hour post-load glucose ≥140 mg/dL, HbA1c ≥5.7%, type 2 diabetes, or treatment for type 2 diabetes
- Blood pressure ≥130/85 mmHg, or antihypertensive treatment
- Plasma triglycerides ≥150 mg/dL, or lipid-lowering treatment
- HDL cholesterol ≤40 mg/dL (men) / ≤50 mg/dL (women), or lipid-lowering treatment
The wider family: SLD, MetALD, and ALD
The 2023 framework also built a house around the diagnosis. Steatotic liver disease (SLD) is the umbrella term for fat in the liver from any cause. Underneath it sit:
- MASLD — steatosis + at least one cardiometabolic criterion, with alcohol intake below the threshold (under 140 g/week in women, under 210 g/week in men — roughly under 20 g/day and 30 g/day respectively)
- MetALD — a genuinely new and useful category: people who meet MASLD criteria and drink moderately (140–350 g/week in women, 210–420 g/week in men). These patients are extremely common in the real world, and the old NAFLD definition simply excluded them from research, leaving a large group of people effectively unstudied. Metabolic dysfunction and alcohol injure the liver together, and MetALD finally names that overlap.
- ALD — alcohol-related liver disease, above the MetALD thresholds
What the rename does not change
It is worth being clear about this, because the change has caused some confusion: the rename does not alter the underlying biology, the treatment, or the prognosis. A person with NAFLD in 2022 and MASLD in 2026 has the same disease and needs the same care. What changes is the label, the diagnostic logic (inclusion rather than exclusion), and the recognition of MetALD. Note also that the great majority of people previously diagnosed with NAFLD — around 98% in validation studies — also meet MASLD criteria, so the two populations overlap almost entirely.
You should also expect a long transition. Decades of research, drug trials, clinical guidelines, insurance codes, and electronic health records are indexed under NAFLD and NASH. Both vocabularies will appear side by side for years, which is why this page uses both.
A related term: MAFLD
You may also encounter MAFLD (metabolic-associated fatty liver disease), proposed by a separate international group in 2020. MAFLD and MASLD overlap heavily but are not identical: MAFLD requires steatosis plus overweight, diabetes, or metabolic dysregulation, and — unlike MASLD — does not exclude people with heavy alcohol intake. MASLD is the term adopted by the 2023 multi-society consensus and is the one now used by AASLD and EASL guidelines.
2. The Disease Spectrum
MASLD is not one condition but a ladder of them, and the rungs carry wildly different risks. Understanding where you sit on this ladder matters more than any other single fact about your liver.
Steatosis (MASL) — simple fatty liver
Fat in more than 5% of liver cells, without meaningful inflammation or scarring. This is where most people with MASLD sit, and for most of them it stays that way. The annual risk of progressing to MASH is roughly 4%, and the ten-year risk of cirrhosis is low. Simple steatosis is not harmless — it still signals the metabolic trouble that drives heart disease — but on its own it is unlikely to destroy your liver.
Steatohepatitis (MASH) — the dangerous form
MASH is steatosis plus two things a pathologist can see: lobular inflammation and hepatocyte ballooning (liver cells swollen with injury). Roughly 20–30% of people with MASLD have MASH. This is the form that scars. It is graded with the NAFLD Activity Score (NAS), which sums steatosis (0–3), lobular inflammation (0–3), and ballooning (0–2); a NAS of 5 or more, with at least one point in each category, is consistent with MASH. Fibrosis is scored separately — NAS measures current activity, fibrosis measures accumulated damage.
Fibrosis (F0–F4) — the stage that actually predicts your future
Scarring is staged from F0 to F4:
- F0 — no fibrosis
- F1 — perisinusoidal or periportal fibrosis
- F2 — both perisinusoidal and periportal (significant fibrosis)
- F3 — bridging fibrosis, where scar tissue connects structures across the liver (advanced fibrosis)
- F4 — cirrhosis
Here is the single most important prognostic fact in this disease: fibrosis stage — not the amount of fat, not the level of inflammation, not your ALT — is what predicts liver-related death. This was established definitively by Angulo and colleagues, whose landmark study was titled, bluntly, "Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes," and confirmed by Ekstedt's cohort followed for up to 33 years and by Taylor's meta-analysis. In MASLD, fibrosis is the thing that kills you. Everything else is a means to that end.
MASLD fibrosis begins in a characteristic place — a perisinusoidal, pericellular "chicken-wire" pattern around the central veins (zone 3) — which distinguishes it from the portal-based scarring of viral hepatitis.
Cirrhosis (F4)
Advanced, architecturally distorted scarring. Once cirrhosis develops, the complications of portal hypertension can follow: esophageal and gastric varices (dilated veins that can bleed catastrophically), ascites (fluid in the abdomen), spontaneous bacterial peritonitis, hepatorenal syndrome, and hepatic encephalopathy (confusion from ammonia the liver can no longer clear). Some fibrosis can regress with sustained treatment; established cirrhosis with architectural distortion is much harder to reverse, though it is no longer considered categorically irreversible.
Hepatocellular carcinoma (HCC)
MASLD is now a leading cause of liver cancer in the United States and much of Europe. It carries one dangerous peculiarity: a substantial share of MASLD-related HCC arises in people who never developed cirrhosis. Published estimates of that share vary widely — from roughly 10% to as high as 40% depending on the population and how it was counted — and we would rather tell you the range honestly than invent a precise-sounding number. The clinical consequence is real either way: standard HCC surveillance is triggered by a cirrhosis diagnosis, so non-cirrhotic MASLD cancers are often found late. In MASH cirrhosis, the annual HCC risk is roughly 1–2%.
3. Pathophysiology: The Multiple-Hit Model
The old explanation was the "two-hit" hypothesis: fat accumulates (hit one), then some insult — oxidative stress, a gut-derived toxin — inflames the fatty liver (hit two). It was elegant and it was wrong, or at least badly incomplete. The current framework is the "multiple parallel hits" model: many insults act at once, on a genetically susceptible person, and their combination determines who progresses from bland fat to inflammation to scar.
Insulin resistance and de novo lipogenesis
Insulin resistance is the central defect. It floods the liver with fat by three routes at once:
- De novo lipogenesis (DNL) — the liver manufactures brand-new fatty acids out of carbohydrate. High insulin and glucose activate the transcription factors SREBP-1c and ChREBP, switching on a pathway that should be quiet. In healthy people DNL contributes only a few percent of liver triglyceride; in MASLD it can supply roughly a quarter of it. Fructose is an especially potent trigger, because it bypasses the phosphofructokinase checkpoint that normally throttles glucose entering this pathway — which is precisely why sugar-sweetened drinks and high-fructose corn syrup punch so far above their calorie weight.
- Free fatty acid flux from fat tissue — insulin normally restrains lipolysis. Insulin-resistant visceral fat ignores it, and pours free fatty acids straight into the portal vein, which delivers them to the liver first.
- Impaired fat disposal — mitochondrial beta-oxidation is blunted, and VLDL export (the liver's way of packaging fat and shipping it out) becomes inadequate. Fat arrives faster than it can be burned or exported.
Lipotoxicity: why fat becomes injury
Stored triglyceride is comparatively inert — it is arguably the liver's attempt to render a toxic surplus safe. The damage comes from toxic lipid intermediates: ceramides, diacylglycerols (DAG), and lysophosphatidylcholine. Saturated fatty acids such as palmitate and stearate drive:
- Endoplasmic reticulum (ER) stress and the unfolded protein response (UPR) — chronic activation recruits CHOP and caspase pathways that kill hepatocytes
- Mitochondrial dysfunction and oxidative stress — reactive oxygen species from overloaded beta-oxidation and CYP2E1-mediated microsomal oxidation cause lipid peroxidation and mitochondrial DNA damage, in a self-amplifying loop
- Activation of inflammatory kinases — notably c-Jun N-terminal kinase (JNK) and IKKβ/NF-κB, central mediators of hepatocyte apoptosis in MASH
Dying hepatocytes release danger signals (DAMPs such as HMGB1 and extracellular vesicles) that recruit and activate Kupffer cells — the liver's resident macrophages — which pour out TNF-α, IL-1β, and IL-6.
The gut–liver axis
People with MASLD reliably show gut dysbiosis and increased intestinal permeability. A leakier gut lets bacterial products — lipopolysaccharide (LPS), lipoteichoic acid, and microbial metabolites — cross into the portal circulation and reach the liver directly. There they activate toll-like receptors (TLR4, TLR9) on Kupffer cells and stellate cells, and trigger the NLRP3 inflammasome. Altered bile-acid signalling through FXR adds another layer. The gut and the liver share a bloodstream, and in MASLD that intimacy works against you.
Fibrogenesis: how the scar forms
Hepatic stellate cells (HSCs) are the liver's fibrosis engine. Normally quiescent, storing vitamin A, they transform under chronic injury signals — TGF-β1, PDGF, leptin — into myofibroblasts that lay down collagen types I and III. Adipokine imbalance tilts the same way: leptin rises and promotes fibrosis, while protective adiponectin falls. The result is progressive, patterned scarring.
Genetics: why two people with identical waistlines get different livers
Genetics explain a substantial share of who progresses. Twin studies show high concordance even after adjusting for metabolic factors, and a handful of common variants do most of the work:
- PNPLA3 I148M (rs738409) — the strongest and most reproducible genetic risk variant in the disease. The methionine-for-isoleucine substitution cripples the protein's lipid-remodelling activity in hepatocytes and stellate cells, trapping triglyceride in the liver. It raises the risk of steatosis, MASH, fibrosis, and HCC. Crucially, it is much more common in Hispanic populations and less common in people of African ancestry — which is a large part of why MASLD prevalence tracks ethnicity in ways that obesity rates alone cannot explain.
- TM6SF2 E167K (rs58542926) — reduces VLDL secretion, so fat stays in the liver instead of being exported. It raises steatohepatitis and fibrosis risk while, paradoxically, lowering cardiovascular risk — less fat exported means less circulating atherogenic lipid. A striking illustration that "good for the liver" and "good for the heart" are not always the same axis.
- MBOAT7 (rs641738) — alters phospholipid remodelling; associated with more hepatic fat and fibrosis.
- HSD17B13 (rs72613567) — a loss-of-function variant that is protective: carriers get less steatohepatitis and less fibrosis despite the fat. Losing this protein appears to spare the liver, which has made it an attractive drug target — silencing it deliberately is being explored therapeutically.
- GCKR (rs1260326) — increases hepatic glucokinase activity and pushes carbohydrate toward DNL.
4. Epidemiology
MASLD is the most common chronic liver disease in the world, and it is still growing.
The most careful global meta-analysis (Younossi and colleagues, 2023, pooling 92 studies and over 9 million people) found an overall global prevalence of about 30% across the whole 1990–2019 study window — but the trend inside that window is the real story. Prevalence rose by roughly 50% in a single generation, from about 25.3% in 1990–2006 to about 38.0% in 2016–2019. The widely quoted "38% of adults" figure is that most-recent-period estimate, not the all-years average, and it is worth being precise about which is which.
Where it is worst
Prevalence by region, from the same analysis:
- Latin America — about 44%, the highest in the world
- Middle East and North Africa — about 37%
- South Asia — about 34%; South-East Asia — about 33%
- North America — about 31%
- East Asia — about 30%; Asia Pacific — about 28%
- Western Europe — about 25%
Who has it
- Among people with obesity, prevalence runs above 50%, and higher still with severe obesity
- Among people with type 2 diabetes, roughly 60–70% have MASLD
- MASH — the progressive form — affects roughly 20–30% of those with MASLD. In the United States, an estimated ~15 million adults have MASH
- Hispanic Americans carry the highest US prevalence, driven substantially by the PNPLA3 I148M variant; Black Americans have notably lower prevalence despite higher rates of obesity and diabetes — a genuine paradox that genetics largely explains
Children
Pediatric MASLD is rising with childhood obesity and is now a serious public health problem in its own right, affecting an estimated 10% or so of children overall and a far higher share of children with obesity. Pediatric disease is not merely adult disease in a smaller body: the histology often shows a portal/periportal (zone 1) predominance rather than the adult zone 3 pattern, and progression can be faster.
Transplant
MASLD/MASH cirrhosis is among the leading indications for liver transplantation in the United States and is one of the fastest-growing. Given the trajectory of obesity and diabetes, it is widely projected to become the leading indication.
5. Risk Factors and Genetics
Metabolic drivers
- Visceral obesity — belly fat matters far more than total weight. Visceral fat drains directly into the portal vein, delivering free fatty acids and inflammatory adipokines (TNF-α, resistin) straight to the liver while secreting less protective adiponectin.
- Type 2 diabetes — the single strongest predictor of progression. Diabetes roughly doubles the risk of advancing to cirrhosis, and it is the risk factor that should most urgently prompt fibrosis screening.
- Metabolic syndrome — MASLD is essentially its hepatic manifestation.
- Dyslipidemia — high triglycerides and low HDL.
- Hypertension.
Hormonal and systemic contributors
- Polycystic ovary syndrome (PCOS) — markedly raises MASLD risk independent of BMI, via hyperinsulinemia and androgen excess.
- Hypothyroidism — thyroid hormone drives hepatic fat oxidation; too little of it slows fat burning and promotes steatosis. (This is not a coincidence — it is exactly why the first approved drug for MASH is a thyroid receptor agonist.)
- Obstructive sleep apnea — intermittent nocturnal hypoxia independently promotes hepatic oxidative stress and fibrosis, beyond shared obesity.
- Sarcopenia — low muscle mass worsens insulin resistance; muscle is a major site of glucose disposal.
- Rapid weight loss or protein malnutrition — paradoxically can provoke steatohepatitis by mobilising a flood of adipose fatty acids and impairing lipoprotein export.
Dietary and lifestyle
- High intake of added fructose, especially from sugar-sweetened beverages
- Ultra-processed foods and refined carbohydrate
- Low fibre, low omega-3 intake
- Physical inactivity and prolonged sedentary time
Genetic risk
The variants described in the Pathophysiology section — above all PNPLA3 I148M and TM6SF2 E167K, with MBOAT7 and GCKR adding risk and HSD17B13 loss-of-function conferring protection — are the best-established genetic determinants. Genetic testing is not currently standard of care, but it is plausible that PNPLA3 genotyping will eventually be used to stratify who needs closer surveillance, particularly for liver cancer.
6. Symptoms and Clinical Presentation
Most people with MASLD have no symptoms whatsoever. Roughly 75–80% are entirely asymptomatic, which is precisely what makes this disease dangerous: it can scar a liver quietly for decades. It is usually discovered by accident — an ultrasound ordered for gallstones, a routine blood panel with a mildly raised ALT, a metabolic workup for diabetes.
When symptoms do appear
- Fatigue — the most common complaint, and the most easily dismissed. It is non-specific and overlaps with every metabolic condition that travels with MASLD.
- Right upper quadrant discomfort — a dull ache or sense of fullness under the right ribs, from stretching of the liver capsule as the organ enlarges. It is an ache, not a crisis; severe pain points elsewhere (gallstones, hepatitis).
- Hepatomegaly — a smooth, non-tender, enlarged liver edge.
- Acanthosis nigricans — dark, velvety skin at the nape of the neck or in the armpits: a visible marker of insulin resistance.
Signs of advanced disease
Once cirrhosis develops, the picture changes to that of end-stage liver disease: jaundice, ascites, peripheral edema, spider angiomata, palmar erythema, splenomegaly, muscle wasting, and hepatic encephalopathy (confusion, asterixis). Bleeding esophageal varices are a medical emergency.
A critical caveat about liver enzymes
Mildly elevated ALT and AST (typically 1–4 times the upper limit of normal, with ALT usually higher than AST — the reverse of alcohol-related disease, where AST:ALT commonly exceeds 2) are the usual laboratory trigger for investigation. But you must not read a normal ALT as reassurance:
Normal liver enzymes do not exclude MASH, and they do not exclude advanced fibrosis or even cirrhosis. A large fraction of people with significant fibrosis have entirely normal transaminases. As fibrosis advances, the AST:ALT ratio tends to rise above 1 — because the ALT-producing hepatocytes are progressively being replaced by scar. A "normal" liver panel has sent an enormous number of people home with a disease they still have.
7. Diagnosis, FIB-4, and Elastography
Diagnosis has three jobs: confirm there is fat, exclude other liver diseases, and — most importantly — find out whether there is fibrosis. That last job is what actually changes your future.
Initial evaluation
- Liver panel: ALT, AST, ALP, GGT, bilirubin, albumin, INR and platelets (albumin, INR and platelet count speak to synthetic function and portal hypertension)
- Metabolic workup: fasting glucose, HbA1c, fasting lipids, BMI, waist circumference
- Exclude the mimics: a careful alcohol history; hepatitis B and C serology; ANA and anti-smooth-muscle antibody (autoimmune hepatitis); ferritin and transferrin saturation (hemochromatosis); ceruloplasmin in patients under 40 (Wilson disease); thyroid function; celiac serology. Ferritin is often mildly raised in MASH itself and correlates with fibrosis — it does not by itself mean iron overload.
FIB-4 — the first test everyone should get
The FIB-4 index is the workhorse of MASLD care. It is free, it uses labs you almost certainly already have, and it is recommended as the first-line fibrosis triage step by AASLD, EASL, AGA, and ACG:
FIB-4 = (Age × AST) ÷ (Platelet count × √ALT)
- FIB-4 <1.30 — low risk of advanced fibrosis. The negative predictive value is high (around 90%). This is genuine reassurance, and these patients can generally be managed in primary care and rechecked in a few years.
- FIB-4 1.30–2.67 — indeterminate. This is not a result; it is a referral for a second test (elastography or ELF).
- FIB-4 >2.67 — high risk of advanced fibrosis (F3–F4). Refer to hepatology.
Age matters, and this is a common trap. FIB-4 contains age in its numerator, so it drifts upward with age all by itself. In patients over 65, the standard 1.30 lower cutoff produces far too many false positives — a lower threshold of about 2.0 and an upper threshold of about 3.25 are more appropriate. In patients under 35, FIB-4 performs poorly in the other direction. Applying adult-average cutoffs blindly across all ages is one of the most frequent errors in MASLD triage.
Elastography (FibroScan) and CAP
Vibration-controlled transient elastography (VCTE / FibroScan) measures liver stiffness in kilopascals as a proxy for fibrosis, and simultaneously reports CAP (controlled attenuation parameter, in dB/m) as a measure of fat. It is quick, non-invasive, and done at the point of care.
- Liver stiffness <8 kPa — advanced fibrosis is unlikely
- 8–12 kPa — indeterminate; needs further assessment
- >12 kPa — advanced fibrosis is likely
- Higher values (roughly >17–20 kPa) increasingly suggest cirrhosis and portal hypertension
Caveats that matter in practice: readings are falsely elevated by recent eating (fast at least 2–3 hours), by active inflammation with high transaminases, and by hepatic congestion from heart failure. Severe obesity reduces reliability and may require the XL probe. A single high reading in a patient who just had lunch is not a diagnosis of cirrhosis.
Other non-invasive tools
- Ultrasound — the usual first imaging test. It shows a bright, echogenic liver, but it only reliably detects steatosis once roughly 20–30% of hepatocytes are involved, and it cannot stage fibrosis at all.
- MRI-PDFF (proton density fat fraction) — the most accurate non-invasive measure of liver fat, sensitive down to about 5%. It is the standard endpoint in modern MASH drug trials. Expensive; mostly research and specialist centres.
- MR elastography (MRE) — the most accurate non-invasive fibrosis test, better than FibroScan in obese patients and in ascites.
- Enhanced Liver Fibrosis (ELF) test — a blood panel of three matrix-turnover markers (hyaluronic acid, PIIINP, TIMP-1). Useful as the second-line test when FIB-4 lands in the indeterminate zone.
- NAFLD Fibrosis Score (NFS) — an older score using age, BMI, glucose, AST/ALT, albumin, and platelets; performs comparably to FIB-4.
When biopsy is still used
Liver biopsy remains the reference standard — it is still the only test that can definitively distinguish MASH from simple steatosis and stage fibrosis precisely. But it is invasive, it costs money, it carries a small but real risk of serious bleeding, and it samples perhaps one fifty-thousandth of the organ, so sampling error is genuine. It is no longer a routine part of diagnosis. It is reserved for when it will actually change what happens next:
- Non-invasive tests are discordant or stubbornly indeterminate, and the answer would change management
- A competing diagnosis (for example autoimmune hepatitis) cannot be excluded any other way
- Enrolment in a clinical trial requires it
- Confirming the fibrosis stage needed to justify a specific drug
8. Treatment: Weight Loss, Diet, and Exercise
Lifestyle change is not the consolation prize you are offered while waiting for a real drug. It remains the foundation of treatment, it is the intervention with the best evidence for reversing fibrosis, and it has no side effects.
The weight-loss ladder — and the 7–10% threshold
The relationship between weight lost and liver healed is dose-dependent, and the numbers below are the most actionable in this entire article. They come principally from Vilar-Gomez's landmark 52-week lifestyle study and Promrat's randomised trial:
- 3–5% of body weight — reduces liver fat (steatosis)
- 7–10% of body weight — this is the threshold that resolves MASH. Inflammation and ballooning improve; the NAS falls. If you remember one number from this page, remember this one.
- ≥10%, sustained — the level at which fibrosis itself regresses, in roughly 45% of patients, with MASH resolution in the large majority
For a 200-pound person, 7–10% is 14–20 pounds. That is a hard target but a human one — and it is worth knowing that it is the liver threshold, not a cosmetic one. A standard approach is a deficit of roughly 500–1,000 kcal/day. Adherence matters more than the precise macronutrient split.
The Mediterranean diet
The Mediterranean diet has the strongest evidence of any dietary pattern in MASLD and is the pattern recommended in guidelines. Olive oil, fish, legumes, whole grains, vegetables, fruit, and nuts; little red meat, little processed food, little added sugar. Its most remarkable property is that it reduces liver fat even without weight loss — through monounsaturated fat, omega-3s, fibre that feeds a healthier microbiome, and polyphenols that act on PPARα, AMPK and SIRT1 to push the liver toward burning fat rather than storing it.
Cut fructose and sugar-sweetened drinks
If there is a single highest-yield specific dietary change, this is it. Fructose is metabolised almost entirely in the liver and bypasses the regulatory checkpoint that limits glucose flowing into fat synthesis — so it drives de novo lipogenesis more or less unopposed, while also generating uric acid. Sodas, energy drinks, sweetened coffees, and fruit juice are the main sources. Whole fruit is fine: the fibre slows absorption and changes the whole picture.
Other dietary approaches
- Low-carbohydrate diets — produce rapid falls in liver fat, often measurable within about two weeks and before meaningful weight loss, by suppressing DNL. Particularly effective in the strongly insulin-resistant. Long-term adherence is the limiting factor, and fibrosis outcome data are thin.
- Omega-3 fatty acids — reduce liver fat in trials (fatty fish, or fish oil). Effects on MASH histology have been less consistent, so treat them as part of a good overall pattern rather than a targeted therapy.
- Coffee — 2 or more cups a day is consistently associated with less fibrosis and lower mortality in MASLD, across many populations and preparation methods. This is observational data, not a trial, so it does not warrant prescribing coffee — but it is a good reason not to tell an existing coffee drinker to stop.
Exercise — and why it works even if you don't lose weight
This is one of the most encouraging facts in the disease: exercise reduces liver fat independently of weight loss. If the scale is not moving, your liver may still be improving.
- 150–300 minutes per week of moderate aerobic exercise — brisk walking, cycling, swimming
- Resistance training 2–3 times per week — adds independent benefit and builds muscle, the body's largest glucose sink
- Break up prolonged sitting; the sedentary hours between workouts matter too
Alcohol
Even moderate drinking accelerates fibrosis in someone who already has steatohepatitis. No safe threshold has been established in MASLD, and the MetALD category exists precisely because alcohol and metabolic dysfunction compound each other. Complete abstinence is recommended for anyone with MASH or any degree of fibrosis.
Supplements: what the evidence supports, and what it doesn't
Several nutrients and botanicals have a plausible mechanism and some human data in fatty liver. None is a substitute for weight loss, and the evidence for all of them is weaker than for the interventions above — mostly small trials using liver enzymes or imaging as endpoints, rather than biopsy-proven MASH resolution. With that honest framing:
- Choline — genuinely required for the liver to package and export fat as VLDL. Choline deficiency can cause fatty liver; this is a well-established mechanism rather than a marketing claim. Eggs and liver are the richest dietary sources. It is a reason to be adequately nourished, not a reason to megadose.
- Silymarin (milk thistle) — antioxidant and anti-inflammatory, with some randomised evidence for modest reductions in liver enzymes. No large trial with histological endpoints has been done, so its effect on fibrosis is simply unknown.
- Berberine — a plant alkaloid that activates AMPK; trial evidence for reduced liver fat and improved enzymes. It interacts with a number of medications and is not benign — discuss it with a clinician rather than adding it silently.
- Omega-3 fatty acids — as above: they reduce liver fat, with inconsistent effects on MASH histology.
Note the asymmetry running through this whole section: the interventions with the strongest evidence — losing 7–10% of your body weight, the Mediterranean pattern, exercise, cutting sugary drinks — are the ones nobody sells you.
Things to avoid
- Sugar-sweetened beverages — the strongest specific dietary risk factor
- Alcohol, as above
- Potentially hepatotoxic supplements — high-dose niacin, concentrated green tea extract (catechins), kava, comfrey, and pennyroyal have all been linked to liver injury. "Natural" is not a synonym for "safe for a damaged liver," and a liver supplement aisle is a strange place to treat liver disease.
Bariatric and metabolic surgery
For people with severe obesity who cannot achieve or hold the necessary weight loss, bariatric surgery is the most reliable route to sustained improvement. Roux-en-Y gastric bypass and sleeve gastrectomy both improve MASH histology, and Lassailly's long-term work has demonstrated durable MASH resolution and fibrosis regression years after surgery. It is contraindicated in decompensated cirrhosis, and requires careful risk–benefit judgment in compensated cirrhosis.
9. Drug Treatment: Resmetirom and GLP-1s
For decades this disease had no approved drug at all. That has changed twice in two years, and MASLD is now one of the fastest-moving areas in medicine.
Resmetirom (Rezdiffra) — the first approved MASH drug
Resmetirom was approved by the FDA in March 2024 — the first drug ever approved specifically for MASH. It received accelerated approval for use alongside diet and exercise in adults with non-cirrhotic MASH with moderate-to-advanced fibrosis (stages F2–F3).
- Mechanism: a liver-directed, selective thyroid hormone receptor-beta (THR-β) agonist. THR-β is the dominant thyroid receptor in the liver, where it drives fatty acid oxidation and suppresses de novo lipogenesis. Selecting for THR-β over THR-α — which predominates in heart and bone — is the whole design idea: you get the liver's thyroid response without the cardiac and skeletal consequences of simply giving thyroid hormone.
- Evidence (MAESTRO-NASH, phase 3, 966 patients with F1B–F3 fibrosis): MASH resolution with no worsening of fibrosis was achieved in 25.9% at 80 mg and 29.9% at 100 mg, versus 9.7% on placebo. Fibrosis improvement by at least one stage with no worsening of the activity score occurred in 24.2% at 80 mg and 25.9% at 100 mg, versus 14.2% on placebo. LDL cholesterol also fell by roughly 14–16%.
- Dosing: weight-based — 80 mg once daily under 100 kg; 100 mg once daily at 100 kg or above.
- Side effects: mostly diarrhea and nausea, usually mild and early.
- Cautions: not for decompensated cirrhosis. It interacts with statins (dose limits apply for some) and with strong CYP2C8 inhibitors; thyroid function is monitored.
Read those numbers honestly. Roughly a quarter of patients improved their fibrosis — against 14% who improved on placebo alone. This is a genuine, historic advance and it is not a cure. It works alongside diet and exercise, not instead of them.
Semaglutide (Wegovy) — the second approved MASH drug
In August 2025, the FDA granted accelerated approval to semaglutide 2.4 mg (Wegovy) for non-cirrhotic MASH with moderate-to-advanced fibrosis (F2–F3) — making it the first GLP-1 receptor agonist approved for this disease. Many sources written before that date still say "no GLP-1 is approved for MASH." That is now out of date.
- Evidence (ESSENCE, phase 3): 1,197 patients with biopsy-defined MASH and F2–F3 fibrosis; the pre-planned 72-week interim analysis of the first 800 found resolution of steatohepatitis without worsening fibrosis in 62.9% on semaglutide versus 34.3% on placebo, and fibrosis improvement without worsening steatohepatitis in 36.8% versus 22.4%. Mean weight loss was 10.5% versus 2.0%.
- Not for patients with cirrhosis, and — like resmetirom — it is approved for use with a reduced-calorie diet and increased physical activity, not as a substitute for them.
- Cautions: avoid with a personal or family history of medullary thyroid carcinoma or MEN2. Gastrointestinal side effects are common.
Note the important nuance on the earlier evidence: the well-known 2021 phase 2 semaglutide trial (Newsome and colleagues) used once-daily semaglutide 0.4 mg — not the weekly 2.4 mg dose — and while it produced striking MASH resolution (59% vs 17%), its fibrosis endpoint was not statistically significant (43% vs 33%, P=0.48). It was the larger phase 3 ESSENCE trial that finally demonstrated a fibrosis benefit. Sources that quote the phase 2 resolution figure as though the fibrosis question was settled in 2021 are overstating it.
Other GLP-1 based agents
- Tirzepatide (Mounjaro/Zepbound) — a dual GIP/GLP-1 agonist. The SYNERGY-NASH trial was a phase 2 study (a point several summaries get wrong), randomising 190 patients with F2–F3 MASH. MASH resolution without worsening fibrosis reached 44%, 56% and 62% at 5, 10 and 15 mg respectively, versus 10% on placebo; fibrosis improvement was around 51–55% versus 30% on placebo. Promising, and not yet approved for MASH.
- Liraglutide — the phase 2 LEAN trial showed MASH resolution in 39% versus 9% on placebo. Superseded in practice by more effective agents.
Older options that still have a role
- Pioglitazone — a PPARγ agonist that improves MASH histology, including in patients with type 2 diabetes. Guideline-supported for selected patients. Limitations are real: weight gain, fluid retention, bone loss in women.
- Vitamin E (800 IU/day alpha-tocopherol) — improved MASH histology in the PIVENS trial, but only in non-diabetic, non-cirrhotic adults, and it showed no fibrosis benefit. Long-term high-dose vitamin E carries safety concerns (an all-cause mortality signal in meta-analyses, and increased prostate cancer risk in the SELECT trial). It is a reasonable option for a narrow group, with the risks disclosed — not a general-purpose liver supplement.
- SGLT2 inhibitors — reduce liver fat and are excellent drugs in MASLD patients who also have type 2 diabetes, chiefly for their cardiovascular and renal benefits. Not approved for MASH itself.
What does not work, and what failed
- Metformin — improves metabolic markers but does not improve liver histology. It is not a MASLD treatment.
- Statins — do not treat MASH, but are safe in MASLD and should not be withheld because of mildly elevated liver enzymes. This is a persistent and harmful myth: patients with fatty liver are at high cardiovascular risk, and cardiovascular disease is what most of them will die of. Withholding a statin from them to "protect the liver" gets the risk calculus exactly backwards.
- Obeticholic acid — an FXR agonist that improved fibrosis in the REGENERATE trial but was not approved for MASH; development for this indication was discontinued after regulatory rejection, with pruritus and LDL elevation among the concerns.
The pipeline
Several agents are in advanced development, including lanifibranor (a pan-PPAR agonist, positive in the phase 2 NATIVE trial and now in phase 3) and FGF21 analogues such as efruxifermin. Given how quickly this field is moving, treat any list of "investigational" drugs — including this one — as perishable.
Managing everything else
Because cardiovascular disease is the leading killer in MASLD, aggressive treatment of blood pressure, LDL cholesterol, and glucose is not a side quest — it is central to treating this patient, whatever their fibrosis stage.
10. Complications
- Cardiovascular disease — the leading cause of death in MASLD, ahead of liver disease itself. MASLD is an independent cardiovascular risk factor over and above the shared metabolic risks, through atherogenic dyslipidemia, systemic inflammation, endothelial dysfunction, and increased coagulability. Most people with fatty liver die of their heart, not their liver — which is why the cardiology in this article is not a digression.
- Cirrhosis and liver failure — the feared hepatic endpoint, and the reason fibrosis staging matters so much.
- Hepatocellular carcinoma — roughly 1–2% per year in MASH cirrhosis, and — uniquely among the common liver diseases — a meaningful fraction arising without cirrhosis.
- Type 2 diabetes — the relationship is bidirectional: MASLD roughly doubles the risk of developing diabetes, and diabetes accelerates MASLD.
- Chronic kidney disease — independently increased in MASLD, through shared insulin resistance, inflammation, and dyslipidemia.
- Extrahepatic cancers — increased risk of colorectal and other cancers; keep age-appropriate cancer screening current.
- Sarcopenia — muscle loss worsens insulin resistance and predicts worse outcomes in advanced disease.
11. Prognosis and Surveillance
Prognosis is governed by fibrosis stage. Almost nothing else on the pathology report changes your outlook nearly as much.
Outlook by fibrosis stage
- F0–F1 (none or minimal fibrosis) — excellent liver prognosis; liver-related death is rare. Cardiovascular risk still applies and still needs treating.
- F2 (significant fibrosis) — meaningful liver risk begins here. This is also the stage at which approved drug therapy becomes an option.
- F3 (advanced/bridging fibrosis) — substantially elevated liver-related mortality; HCC risk begins before cirrhosis is reached.
- F4 (cirrhosis) — the highest risk, with annual decompensation and cancer risk. Survival falls sharply once decompensation (ascites, variceal bleeding, encephalopathy) occurs.
Across cohorts, each additional fibrosis stage carries a stepwise increase in liver-related mortality — the central finding of Angulo's cohort, Ekstedt's 33-year follow-up, and Taylor's meta-analysis.
How fast does it progress?
Slowly, and unevenly. On average, fibrosis advances roughly one stage every seven years in MASH — but the average conceals enormous variation. A large minority of patients never progress at all over years of follow-up, while others advance rapidly. Type 2 diabetes is the strongest predictor of fast progression. Progression is also not one-way: fibrosis can and does regress when the metabolic driver is removed.
One curiosity worth knowing: "burned-out" MASH. In some people who reach cirrhosis, the original steatosis and inflammation quietly disappear, leaving scar tissue with no fat and no MASH on biopsy. Their cirrhosis then looks "cryptogenic" — of unknown cause — when in fact MASLD caused it and then covered its tracks. A meaningful share of so-called cryptogenic cirrhosis is burned-out MASH.
Surveillance
- Cirrhosis: liver ultrasound (with or without AFP) every 6 months for HCC. In severe obesity, where ultrasound quality is poor, cross-sectional imaging may be needed.
- Varices: endoscopy at the time of cirrhosis diagnosis, then per guideline; non-selective beta-blockers for prophylaxis where indicated.
- Advanced fibrosis without cirrhosis (F3): HCC surveillance is individualised — there is no firm consensus, and this is an area of genuine and active debate, precisely because MASLD cancers do occur pre-cirrhosis.
- Transplant: referral when decompensation occurs or MELD rises. After transplant, MASLD frequently recurs in the new liver if the metabolic syndrome that caused it is not addressed — a transplant replaces the organ, not the disease.
12. Prevention
- Find it early with FIB-4. The highest-yield systemic intervention available today: calculate FIB-4 in everyone with type 2 diabetes, obesity, or metabolic syndrome. It costs nothing, uses labs already drawn, and identifies the people heading for cirrhosis while there is still time to act.
- Treat the metabolic syndrome — glucose, blood pressure, lipids, weight. The liver follows the metabolism.
- Eliminate sugar-sweetened beverages — individually and, at population level, through policy. This is the modifiable exposure with the clearest mechanistic line to the liver.
- Mediterranean dietary pattern and 150+ minutes per week of moderate activity.
- Limit or avoid alcohol, particularly once metabolic risk factors are present.
- Be cautious with hepatotoxic drugs and supplements where alternatives exist.
- Surveillance for those at highest risk — advanced fibrosis and cirrhosis, as above.
13. Key Research Papers
Every citation below has been checked against PubMed; the linked year/volume/pages resolves to the paper named.
- Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78(6):1966–1986. PMID: 37363821 — the paper that renamed the disease.
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797–1835. PMID: 36727674
- European Association for the Study of the Liver (EASL), EASD, EASO. EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Journal of Hepatology. 2024;81(3):492–542. PMID: 38851997
- Harrison SA, Bedossa P, Guy CD, et al. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis (MAESTRO-NASH). New England Journal of Medicine. 2024;390(6):497–509. PMID: 38324483 — the trial behind the first approved MASH drug.
- Sanyal AJ, Newsome PN, Kliers I, et al.; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. New England Journal of Medicine. 2025;392(21):2089–2099. PMID: 40305708 — the trial behind the semaglutide approval.
- Loomba R, Hartman ML, Lawitz EJ, et al.; SYNERGY-NASH Investigators. Tirzepatide for metabolic dysfunction-associated steatohepatitis with liver fibrosis. New England Journal of Medicine. 2024;391(4):299–310. PMID: 38856224 — a phase 2 trial, despite frequent misdescription as phase 3.
- Newsome PN, Buchholtz K, Cusi K, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. New England Journal of Medicine. 2021;384(12):1113–1124. PMID: 33185364
- Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN). The Lancet. 2016;387(10019):679–690. PMID: 26608256
- Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis (PIVENS). New England Journal of Medicine. 2010;362(18):1675–1685. PMID: 20427778
- Francque SM, Bedossa P, Ratziu V, et al. A randomized, controlled trial of the pan-PPAR agonist lanifibranor in NASH (NATIVE). New England Journal of Medicine. 2021;385(17):1547–1558. PMID: 34670042
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology. 2015;149(2):367–378. PMID: 25865049 — the source of the 7–10% weight-loss threshold.
- Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51(1):121–129. PMID: 19827166
- Lassailly G, Caiazzo R, Ntandja-Wandji LC, et al. Bariatric surgery provides long-term resolution of nonalcoholic steatohepatitis and regression of fibrosis. Gastroenterology. 2020;159(4):1290–1301. PMID: 32553765
- Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. Journal of Hepatology. 2017;67(4):829–846. PMID: 28545937
- Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology. 2015;149(2):389–397. PMID: 25935633 — fibrosis stage is what matters.
- Ekstedt M, Hagström H, Nasr P, et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology. 2015;61(5):1547–1554. PMID: 25125077
- Taylor RS, Taylor RJ, Bayliss S, et al. Association between fibrosis stage and outcomes of patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterology. 2020;158(6):1611–1625. PMID: 32027911
- Younossi ZM, Golabi P, Paik JM, et al. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–1347. PMID: 36626630 — the source of the 30% pooled / 38% recent-period prevalence figures.
- Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease — meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. PMID: 26707365
- Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nature Reviews Gastroenterology & Hepatology. 2018;15(1):11–20. PMID: 28930295
- Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nature Genetics. 2008;40(12):1461–1465. PMID: 18820647 — the PNPLA3 discovery paper.
- Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ. Mechanisms of NAFLD development and therapeutic strategies. Nature Medicine. 2018;24(7):908–922. PMID: 29967350
- Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease (the NAFLD Activity Score). Hepatology. 2005;41(6):1313–1321. PMID: 15915461
- Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. PMID: 16729309 — the original FIB-4 paper.
- Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. PMID: 17393509
- Eslam M, Sanyal AJ, George J, et al. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014. PMID: 32044314
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the AASLD. Hepatology. 2018;67(1):328–357. PMID: 28714183
14. PubMed Topic Searches
These links open live PubMed queries — results update as new studies are indexed.
- MASLD — metabolic dysfunction-associated steatotic liver disease
- MASH / NASH treatment and fibrosis
- NAFLD — non-alcoholic fatty liver disease (legacy term)
- Resmetirom for MASH with fibrosis
- Semaglutide and GLP-1 agonists in MASH
- FIB-4 score and non-invasive fibrosis assessment
- Elastography / FibroScan in fatty liver
- PNPLA3 and TM6SF2 genetic variants
- Insulin resistance and de novo lipogenesis
- Mediterranean diet and fatty liver
- MASLD, HCC, and non-cirrhotic liver cancer
- Fatty liver and cardiovascular mortality
Connections
- History of Fatty Liver Disease
- Liver Disease
- Cirrhosis
- Hepatic Encephalopathy
- Alcoholic Hepatitis
- Autoimmune Hepatitis
- Hepatitis C
- Hemochromatosis
- Liver Cancer (HCC)
- Metabolic Syndrome
- Insulin Resistance
- Type 2 Diabetes
- Obesity
- Polycystic Ovary Syndrome
- Hypothyroidism
- Cardiovascular Disease
- Hypertension
- SIBO
- Pancreatitis
- Gallstones
- GLP-1 Receptor Agonists
- Mediterranean Diet
- Exercise
- Fasting
- Liver Function Tests
- GGT
- Coffee and Liver Disease
- Olive Oil
- Salmon (omega-3)
- Resistant Starches for Fatty Liver
- Ultra-Processed Foods
- Milk Thistle (silymarin)
- Berberine
- Vitamin E
- Choline
- Phosphatidylcholine