Vitamin B12 for Vegans and Absorption Issues
B12 has the most fragile absorption pathway of any vitamin — a five-step cascade that requires stomach acid, haptocorrin, intrinsic factor, the cubilin-amnionless ileal receptor, and transcobalamin II to deliver a single molecule to its target cell. Any of these steps can fail. The two highest-prevalence failure modes are insufficient dietary intake (universal in strict vegans without supplementation, because no plant food reliably contains bioactive B12) and impaired absorption (PPI users, metformin users, post-bariatric patients, atrophic gastritis in 30% of adults over 60). This deep-dive walks through why strict vegan diets cause near-universal deficiency, why nori and spirulina B12 is mostly inactive analogues, the mechanism of PPI- and metformin-induced deficiency, atrophic gastritis in the elderly, optimal supplementation strategies for high-risk groups, and the methylcobalamin vs. cyanocobalamin debate.
Interactive Visualization Vitamin B12’s Impossible Journey Five stages, two carrier proteins, a working stomach and one specific stretch of gut. Break any link — a PPI, metformin, pernicious anaemia — and absorption collapses. Launch →
Table of Contents
- Vegan Deficiency Is Essentially Universal
- Nori, Spirulina, and the Inactive-Analogue Problem
- PPIs and H2 Blockers
- Metformin-Induced B12 Deficiency
- Atrophic Gastritis in the Elderly
- Post-Bariatric and Gastric Surgery
- Supplementation Strategies by Risk Group
- The Methylcobalamin vs Cyanocobalamin Debate
- Cautions
- Key Research Papers
- Connections
- Featured Videos
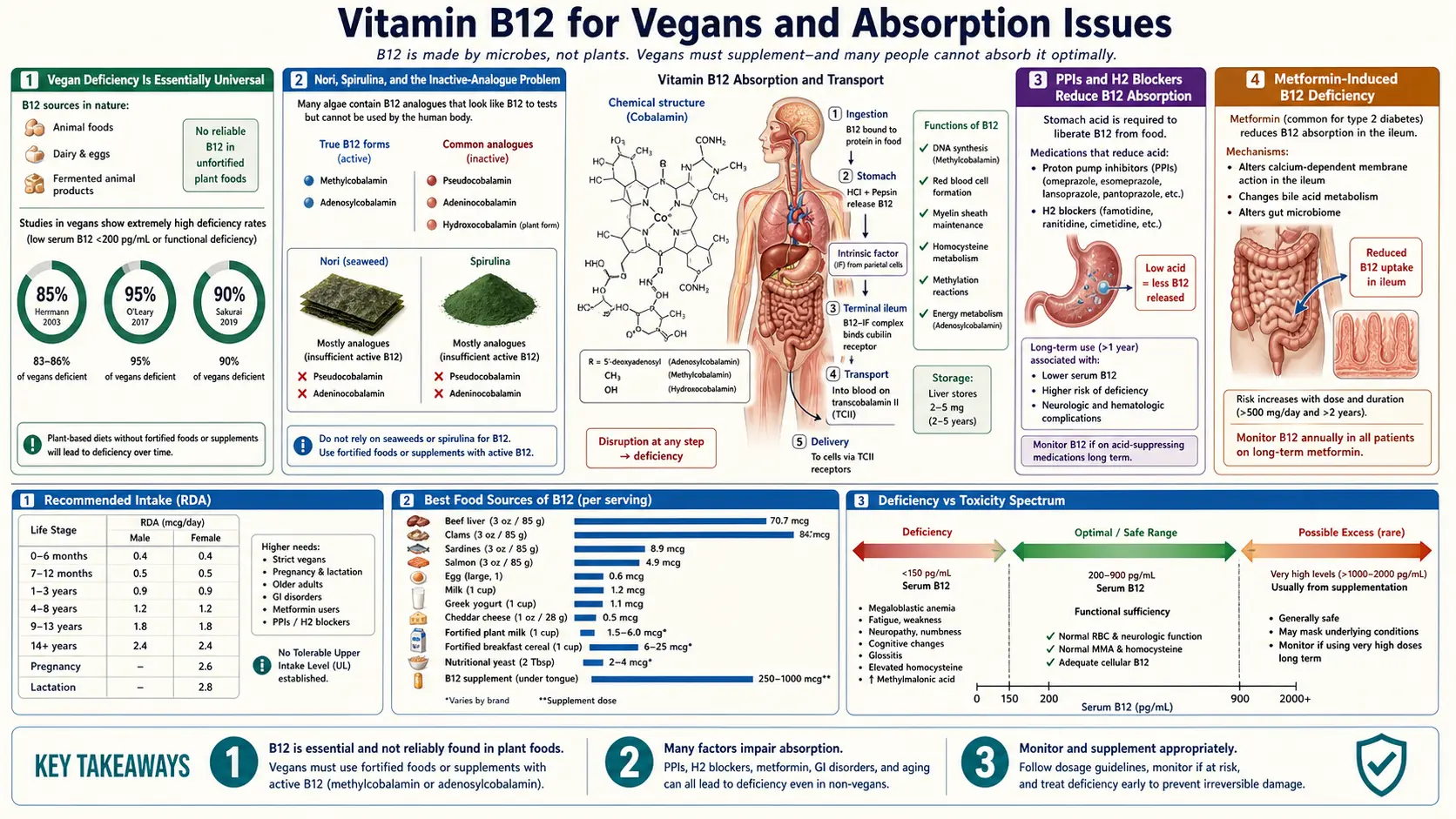
Vegan Deficiency Is Essentially Universal
B12 is the only vitamin that cannot be reliably obtained from any plant food. The reason is biological: B12 is produced exclusively by certain bacteria and archaea, not by plants or animals. Animals that eat B12-producing bacteria (or eat other animals that did) accumulate B12 in their tissues. Plants do not.
The clinical consequence: any diet that excludes all animal foods (meat, fish, eggs, dairy) without supplementation will eventually produce B12 deficiency. The timeline depends on starting reserves (healthy adults store 2-5 mg of B12 in the liver, which is enough for 3-5 years of demand), but the trajectory is the same: serum B12 falls, then MMA rises, then symptoms appear.
The evidence is consistent across studies:
- Studies of unsupplemented long-term vegans show B12 deficiency prevalence in the range of 50-90% depending on the diagnostic threshold used
- Even self-described "well-supplemented" vegans frequently have inadequate B12 status when measured rigorously with MMA and holoTC
- Infants born to and breastfed by B12-deficient vegan mothers can develop severe, sometimes irreversible neurological injury within months of birth — this is a recognized medical emergency described in pediatric case reports from around the world
- Long-term vegetarians (lacto-ovo) have lower but still meaningfully elevated rates of B12 deficiency compared to omnivores — egg and dairy consumption alone is usually insufficient unless intake is high and regular
The bottom line, accepted by every major nutrition society including the Academy of Nutrition and Dietetics (US), the British Dietetic Association, the German Society for Nutrition, and the Vegan Society itself: every strict vegan must supplement B12, without exception.
Practical recommendations for vegans:
- Methylcobalamin or cyanocobalamin 250-1000 mcg daily, or 2000 mcg twice weekly
- Sublingual or oral routes are equivalent for most people
- Check serum B12 + MMA every 1-2 years to confirm adequacy
- Vegan pregnant and breastfeeding women should be particularly careful — their B12 needs are elevated and their infants depend entirely on maternal B12 status
- Vegan infants and children should receive age-appropriate B12 supplementation; in infants under 6 months exclusively breastfed by vegan mothers, the maternal supplementation must be aggressive and the infant's B12 status should be checked at 6 months
Nori, Spirulina, and the Inactive-Analogue Problem
The persistent claim that certain plant foods — particularly nori, spirulina, chlorella, tempeh, miso, and other fermented foods — contain "natural" B12 sufficient for vegan needs is one of the most damaging pieces of misinformation in alternative nutrition. The truth is more complicated.
Most B12 measurements use microbiological assays or chemiluminescence assays that detect "corrinoids" — molecules with the cobalt-corrin ring structure of B12. The problem is that not all corrinoids are bioactive in humans. Bacteria produce many different corrinoid variants, some of which have minor chemical modifications that prevent them from binding to human intrinsic factor and methionine synthase. These molecules show up as "B12" on standard assays but cannot fulfill B12's metabolic role — they are called inactive B12 analogues or pseudovitamin B12.
Specifics:
- Spirulina — up to 80% of its measured "B12" is pseudovitamin B12. The remaining 20% that is bioactive is in small enough amounts that spirulina cannot reliably meet B12 needs. Worse, the inactive analogues may actually compete with true B12 for binding sites, potentially worsening deficiency. Spirulina is not a reliable B12 source and should not be used as one.
- Chlorella — some chlorella strains do contain detectable bioactive B12 (apparently of bacterial origin from the culture medium), but the amounts vary widely between batches and producers, and clinical reliability is poor. Not recommended as a primary B12 source.
- Nori (Porphyra) — certain varieties of nori, particularly dried nori from Japanese producers, do contain bioactive B12 in measurable amounts. However, the bioavailability is uncertain, the amounts are inconsistent, and the quantity of nori needed to meet daily B12 requirements is unrealistically large for most diets. Useful as a contributing source for some vegans but not a substitute for supplementation.
- Fermented foods (tempeh, miso, sauerkraut, kimchi) — trace amounts of B12 from fermentation bacteria can be detected in some products, but the amounts are too small and too variable to meaningfully contribute to B12 status. Not a reliable source.
- Mushrooms — some mushroom varieties (especially shiitake grown on B12-enriched substrates) contain small amounts of B12, but again the amounts are insufficient and inconsistent.
- Fortified plant milks, fortified nutritional yeast, fortified breakfast cereals — these contain added cyanocobalamin or methylcobalamin and are reliable sources. Read the label: unfortified nutritional yeast contains no B12.
The take-home message: fortified foods and supplements are the only reliable B12 sources for vegans. Whole plant foods alone, including all of the much-touted "natural" plant sources, are not sufficient.
This is not a controversial statement among practicing nutrition scientists. It is one of the rare topics in nutrition where the evidence is so clear and so consistent that even the most plant-positive organizations agree.
PPIs and H2 Blockers
Proton pump inhibitors (PPIs) — omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, dexlansoprazole — and H2 receptor blockers — famotidine, ranitidine (now withdrawn in many countries), nizatidine, cimetidine — reduce gastric acid output. They are among the most commonly prescribed medications in the world, used for GERD, peptic ulcer disease, Barrett's esophagus, prevention of NSAID-related ulcers, and many other indications.
Gastric acid is the first essential step in B12 absorption. B12 in food is bound to proteins; gastric acid plus pepsin liberates B12 from these protein carriers so it can bind to haptocorrin and proceed through the absorption cascade. When gastric acid is suppressed, this liberation step fails. Synthetic B12 in supplements (already free, not protein-bound) bypasses this problem — only food-bound B12 absorption is impaired.
Clinical implications:
- Long-term PPI use (>2 years) is associated with a significantly increased risk of B12 deficiency — multiple large cohort studies have confirmed this
- The effect is dose-dependent and duration-dependent — higher doses and longer use produce greater deficiency risk
- H2 blockers carry a similar but typically smaller risk because their acid suppression is less complete
- Older adults on PPIs are at particularly elevated risk because their baseline B12 absorption is already reduced by age-related atrophic gastritis
Practical management:
- Patients on PPIs for >1 year should have B12 status checked annually
- Daily supplemental B12 (250-1000 mcg) is appropriate prophylaxis for long-term PPI users — this bypasses the absorption problem because synthetic B12 doesn't need to be liberated from food
- Consider periodic PPI deprescribing trials — many patients can step down to H2 blockers or to as-needed PPI use, reducing the chronic absorption impairment
- Methylcobalamin, hydroxocobalamin, or cyanocobalamin all work for PPI users — the form is less important than the consistent daily supplementation
Metformin-Induced B12 Deficiency
Metformin is the most widely prescribed diabetes medication worldwide and the first-line drug for type 2 diabetes. It also reduces B12 absorption through a complex mechanism that appears to involve calcium-dependent disruption of the cubilin-amnionless receptor in the terminal ileum. Long-term metformin users develop B12 deficiency at rates of approximately 10-30% depending on duration, dose, and the diagnostic threshold used.
The clinical risk is particularly important because:
- Metformin is taken long-term — often for decades
- The diabetic patient population is already at high risk for peripheral neuropathy (from the diabetes), and B12 deficiency adds an entirely separate cause of peripheral neuropathy
- The neuropathy that develops is frequently attributed to "diabetic neuropathy" when in reality some or all of it is B12 deficiency from the metformin
- B12 deficiency is treatable; diabetic neuropathy is much harder to treat
The American Diabetes Association now recommends periodic B12 monitoring for all patients on long-term metformin, particularly those with peripheral neuropathy, anemia, or other suggestive findings.
Practical management:
- All metformin users should have a baseline B12 level checked, repeated annually thereafter
- Consider routine B12 supplementation (500-1000 mcg/day) for any patient on metformin >1 year, particularly older adults and those with elevated MMA
- If neuropathic symptoms develop in a metformin-treated diabetic patient, check B12 and MMA before assuming the symptoms are from the diabetes — the B12-deficient subgroup may have completely reversible symptoms with repletion
- Calcium supplementation (1200-1500 mg/day) has been shown to partially reverse the metformin-induced B12 malabsorption — the mechanism is thought to involve calcium-dependent restoration of the ileal receptor function. However, this should not substitute for B12 supplementation; both can be used
Atrophic Gastritis in the Elderly
Atrophic gastritis — the thinning and partial loss of the gastric glandular lining — affects approximately 30% of adults over age 60. The condition is often asymptomatic but produces clinically meaningful reduction in gastric acid secretion and intrinsic factor production. It is the most common cause of B12 deficiency in the elderly and a major contributor to the broader picture of late-life cognitive decline, peripheral neuropathy, and fatigue.
Causes of atrophic gastritis:
- Autoimmune (pernicious anemia) — the body-predominant type with anti-parietal-cell and anti-intrinsic-factor antibodies
- H. pylori-related — the antrum-predominant type from chronic H. pylori infection that has eradicated the gastric glandular tissue over years; an underappreciated cause of B12 deficiency in older adults with prior H. pylori exposure
- Environmental / age-related — the multifactorial type that develops gradually with aging without a clear single cause
Clinical presentation: often nothing — many patients are entirely asymptomatic. When symptoms occur, they may include dyspepsia, early satiety, postprandial fullness, and slow gastric emptying. The clinical hallmark of severe atrophic gastritis is its consequences: B12 deficiency, iron deficiency (from impaired acid-dependent iron solubilization), reduced absorption of other micronutrients, and elevated gastric cancer risk.
Diagnosis: serum gastrin (markedly elevated in autoimmune atrophic gastritis), pepsinogen I (low) and pepsinogen I/II ratio (suppressed), anti-IF and anti-parietal-cell antibodies, and confirmatory upper endoscopy with body and antrum biopsies. The non-invasive "GastroPanel" combines gastrin-17, pepsinogen I, pepsinogen II, and anti-H. pylori antibodies into a single test that can stratify atrophic gastritis risk without requiring endoscopy.
Management for B12: the same as for pernicious anemia — lifelong B12 supplementation, either parenteral or high-dose oral. The atrophic gastritis itself is generally not reversible (though H. pylori eradication can stop progression and sometimes produce partial regeneration), but the B12 deficiency it causes is fully treatable.
Recommendation: every patient over age 60 with unexplained fatigue, peripheral neuropathy, cognitive decline, or unexplained anemia should have B12 (with MMA if borderline) checked. The cost is trivial and the diagnostic yield is meaningful.
Post-Bariatric and Gastric Surgery
Bariatric surgery (Roux-en-Y gastric bypass, sleeve gastrectomy, biliopancreatic diversion) fundamentally alters B12 absorption anatomy. The mechanisms vary by procedure:
- Roux-en-Y gastric bypass — bypasses most of the stomach (reduced acid and intrinsic factor production) and the duodenum/proximal jejunum, with the food stream rejoining the digestive enzymes in the mid-jejunum. The combined acid + IF + transit-time effect is substantial. B12 deficiency develops in 30-50% of patients within 5 years if not supplemented.
- Sleeve gastrectomy — removes a large portion of the stomach (reducing acid and IF) but preserves the rest of the GI tract. B12 deficiency is less common than after Roux-en-Y but still elevated, with rates of 10-20% over 5 years.
- Biliopancreatic diversion (now uncommon) — severe macro- and micronutrient malabsorption; high rates of multiple vitamin and mineral deficiencies including B12.
- Subtotal or total gastrectomy (for gastric cancer or severe ulcer disease) — eliminates intrinsic factor production entirely. Lifelong B12 supplementation is mandatory, equivalent to pernicious anemia management.
Universal recommendation: all post-bariatric patients require lifelong B12 supplementation. Standard protocols:
- Sublingual or oral methylcobalamin/cyanocobalamin 1000-2000 mcg daily, OR
- Intramuscular hydroxocobalamin 1000 mcg every 1-3 months
- Annual B12 monitoring + MMA + CBC
- Concurrent iron, calcium + vitamin D, and other micronutrient monitoring (these patients are at risk for multiple deficiencies, not just B12)
Supplementation Strategies by Risk Group
Healthy Omnivore (Maintenance / Insurance)
- Optional B-complex supplement containing 100-500 mcg B12 several times weekly
- Most healthy omnivores with good appetite for meat, fish, dairy, and eggs do not need to supplement
- Consider checking serum B12 once in middle age to establish a baseline
Vegetarian (Lacto-Ovo)
- Methylcobalamin or cyanocobalamin 250-500 mcg daily, or 1000 mcg several times weekly
- Check serum B12 + MMA every 2-3 years
- Particularly important if egg/dairy consumption is sporadic
Vegan
- Methylcobalamin or cyanocobalamin 250-1000 mcg daily, OR 2000 mcg twice weekly
- Check serum B12 + MMA every 1-2 years (every 6-12 months in pregnancy / lactation)
- Mandatory for life — no exceptions
Long-term PPI / H2 Blocker User
- Methylcobalamin or cyanocobalamin 500-1000 mcg daily (bypasses acid-dependent absorption step)
- Annual B12 + MMA monitoring
- Periodic deprescribing trial to reduce or eliminate PPI use if clinically feasible
Long-term Metformin User
- Methylcobalamin or cyanocobalamin 500-1000 mcg daily
- Annual B12 + MMA monitoring (recommended by ADA)
- Consider calcium 1200 mg/day for partial restoration of ileal absorption
Adults Over 60
- Methylcobalamin or cyanocobalamin 250-500 mcg daily (Institute of Medicine recommendation for adults >50)
- Periodic B12 + MMA monitoring, every 2-3 years
- If cognitive symptoms, fatigue, or neuropathy emerges, check B12 status promptly
Pernicious Anemia
- Initial IM hydroxocobalamin/methylcobalamin daily for 1-2 weeks, then weekly for 4-8 weeks
- Maintenance: IM hydroxocobalamin 1000 mcg every 1-3 months, OR daily high-dose oral methylcobalamin 2000 mcg
- Lifelong; never stop
- Periodic monitoring of B12, MMA, CBC, thyroid function
- Endoscopic gastric cancer surveillance every 3-5 years
Post-Bariatric Surgery
- Sublingual or oral methylcobalamin 1000-2000 mcg daily, OR IM hydroxocobalamin every 1-3 months
- Annual B12 + MMA + CBC + iron studies + vitamin D + parathyroid hormone
- Lifelong
The Methylcobalamin vs Cyanocobalamin Debate
One of the most persistent debates in the natural medicine community concerns the choice between methylcobalamin (the methylated coenzyme form) and cyanocobalamin (the synthetic, cyanide-containing form) for general supplementation. Both reach essentially the same end — raising tissue B12 levels — but they take different paths to get there.
The case for methylcobalamin:
- Already in the active coenzyme form — no metabolic conversion required
- Directly participates in the methionine synthase reaction
- Preferred in patients with neurological involvement (per the integrative neurology literature)
- Preferred in smokers (no cyanide load)
- Preferred in patients with renal impairment (slowed cyanide clearance)
- Preferred in patients with MTHFR variants or chronic methylation issues
- Has slightly better tissue retention in some pharmacokinetic studies
The case for cyanocobalamin:
- Vastly more studied — nearly all of the 60+ years of clinical evidence for B12 therapy used cyanocobalamin
- Substantially cheaper (often 5-10x less expensive than methylcobalamin)
- More stable in storage (less degradation from light, heat, oxygen)
- Equally effective at raising serum B12 and correcting hematological deficiency
- The "cyanide" concern is overstated — the amount of cyanide released from a 1000 mcg dose is approximately 20 mcg, which is trivial compared to the daily cyanide exposure from food (almonds, apricot kernels, leafy greens contain measurable cyanide naturally)
The case for hydroxocobalamin:
- Naturally occurring form (produced by bacteria, including those in the gut)
- Longest tissue retention — the standard for IM injection in Europe
- No cyanide concern
- Scavenges excess nitric oxide (relevant for some inflammatory conditions)
- Now available in many countries as the IM injection of choice
Practical resolution:
- For healthy people with no special concerns: any form works. Choose based on cost and availability.
- For neurological involvement, MTHFR variants, smokers, renal impairment, or "biochemical sensitivity": methylcobalamin or hydroxocobalamin preferred over cyanocobalamin.
- For IM injection: hydroxocobalamin preferred (longer interval between doses) but cyanocobalamin also acceptable.
- For maximum natural medicine pedigree: hydroxocobalamin (the bacterial-natural form).
- The choice matters less than consistent supplementation — taking any form of B12 reliably every day is far better than choosing the "perfect" form and missing doses.
Cautions
- Vegan pregnancy and infants — the highest-stakes B12 scenario. Vegan and unsupplemented vegetarian mothers can have infants with severe, sometimes permanent neurological injury within months of birth. Ensure aggressive maternal supplementation throughout pregnancy and lactation, and check infant B12 status at 6 months. If breastfeeding a vegan diet, give the infant direct B12 supplementation (consult a pediatrician for age-appropriate dosing).
- Do not rely on spirulina, chlorella, nori, fermented foods, or unfortified nutritional yeast — these are not adequate B12 sources regardless of what online vegan communities claim.
- Do not stop PPIs or metformin without medical guidance — these drugs are prescribed for important reasons. Add B12 supplementation rather than discontinuing the medication unless the physician advises otherwise.
- Check for combined deficiencies — vegans, atrophic gastritis patients, post-bariatric patients, and the elderly are at risk for multiple deficiencies (iron, vitamin D, calcium, zinc, omega-3, vitamin B6, vitamin B2) not just B12. A comprehensive nutritional assessment is warranted.
- Methylated forms can occasionally cause overstimulation — in patients with COMT slow variants or histamine sensitivity, high-dose methylcobalamin (especially combined with high-dose methylfolate) can produce anxiety, insomnia, or irritability. Start at the lower end and titrate.
- Acne flares — rarely, high-dose B12 (cyanocobalamin in particular) can trigger acne or rosacea flares. Switching to methylcobalamin or hydroxocobalamin usually resolves the issue.
- Nitrous oxide — B12 deficiency is precipitated or worsened by nitrous oxide exposure (recreational "whippets" or repeated dental anesthesia). Patients with marginal B12 status should ensure aggressive supplementation before any planned N2O exposure and should avoid recreational use entirely.
Key Research Papers
- Pawlak R et al. (2014). The prevalence of cobalamin deficiency among vegetarians assessed by serum vitamin B12: a review of literature. Eur J Clin Nutr. — PubMed
- Watanabe F (2007). Vitamin B12 sources and bioavailability. Exp Biol Med. — the canonical review of plant B12 analogue issues. — PubMed
- Yamada K et al. (1999). Falsely high values for vitamin B12 of spirulina-based supplements: pseudovitamin B12 reactivity. J Agric Food Chem. — PubMed
- Lam JR et al. (2013). Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. — large cohort study definitively establishing PPI risk. — PubMed
- de Jager J et al. (2010). Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. — PubMed
- Aroda VR et al. (2016). Long-term metformin use and vitamin B12 deficiency in the Diabetes Prevention Program Outcomes Study. J Clin Endocrinol Metab. — PubMed
- Allen LH (2009). How common is vitamin B-12 deficiency? Am J Clin Nutr. — PubMed
- Andres E et al. (2004). Vitamin B12 (cobalamin) deficiency in elderly patients. CMAJ. — PubMed
- Russell RM (1992). Changes in gastrointestinal function attributed to aging. Am J Clin Nutr. — atrophic gastritis epidemiology in the elderly. — PubMed
- Stein J et al. (2014). The nutritional and pharmacological consequences of obesity surgery. Aliment Pharmacol Ther. — PubMed
- Rizzo G et al. (2016). Vitamin B12 among vegetarians: status, assessment and supplementation. Nutrients. — PubMed
- Wile DJ, Toth C (2010). Association of metformin, elevated homocysteine, and methylmalonic acid levels and clinically worsened diabetic peripheral neuropathy. Diabetes Care. — PubMed
PubMed Topic Searches
- PubMed: vegan vegetarian B12 deficiency
- PubMed: spirulina pseudovitamin B12
- PubMed: PPI B12 deficiency
- PubMed: metformin B12 deficiency long-term
- PubMed: atrophic gastritis elderly B12 iron
- PubMed: methylcobalamin vs cyanocobalamin
Connections
- Vitamin B12’s Impossible Journey — interactive animation
- Vitamin B12 Overview
- B12 Benefits Hub
- B12 for Nerve Health
- B12 for Anemia
- B12 for Cognition & Methylation
- B12 Deficiency Diagnosis
- B12 and Nervous System
- Vitamin B12 Test
- Homocysteine
- Complete Blood Count
- Anemia
- SIBO
- Celiac Disease
- Crohn's Disease
- Diabetes (Metformin)
- Metformin — blocks B12 uptake at the ileal receptor.
- Organ Meats
- Eggs
- Salmon