Vitamin B12 for Anemia and Hematology
Pernicious anemia was the first disease for which B12 was identified as the cure — it earned the Nobel Prize in Medicine in 1934. Before B12 was characterized, pernicious anemia was uniformly fatal: a relentless progression of fatigue, neurological deterioration, and death over 1-3 years. Today it remains the most well-known clinical context for B12 therapy, but the picture is wider than autoimmune intrinsic factor deficiency alone: megaloblastic anemia from any cause (vegan diet, malabsorption, drug-induced) responds to B12. This deep-dive walks through the molecular mechanism of the megaloblastic defect, the autoimmune pathophysiology of pernicious anemia, the historical Schilling test and its modern replacements, the IM injection protocols, and the surprising clinical reality that high-dose oral B12 works even in pernicious anemia.
Interactive Visualization Vitamin B12’s Impossible Journey Five stages, two carrier proteins, a working stomach and one specific stretch of gut. Break any link — a PPI, metformin, pernicious anaemia — and absorption collapses. Launch →
Table of Contents
- Megaloblastic Anemia Mechanism
- Pernicious Anemia
- Schilling Test and Its Replacements
- Modern Diagnostic Workup
- IM Injection Protocols
- High-Dose Oral (Berlin Protocol)
- Response Monitoring
- Combined Iron + B12 + Folate Deficiency
- Cautions
- Key Research Papers
- Connections
- Featured Videos
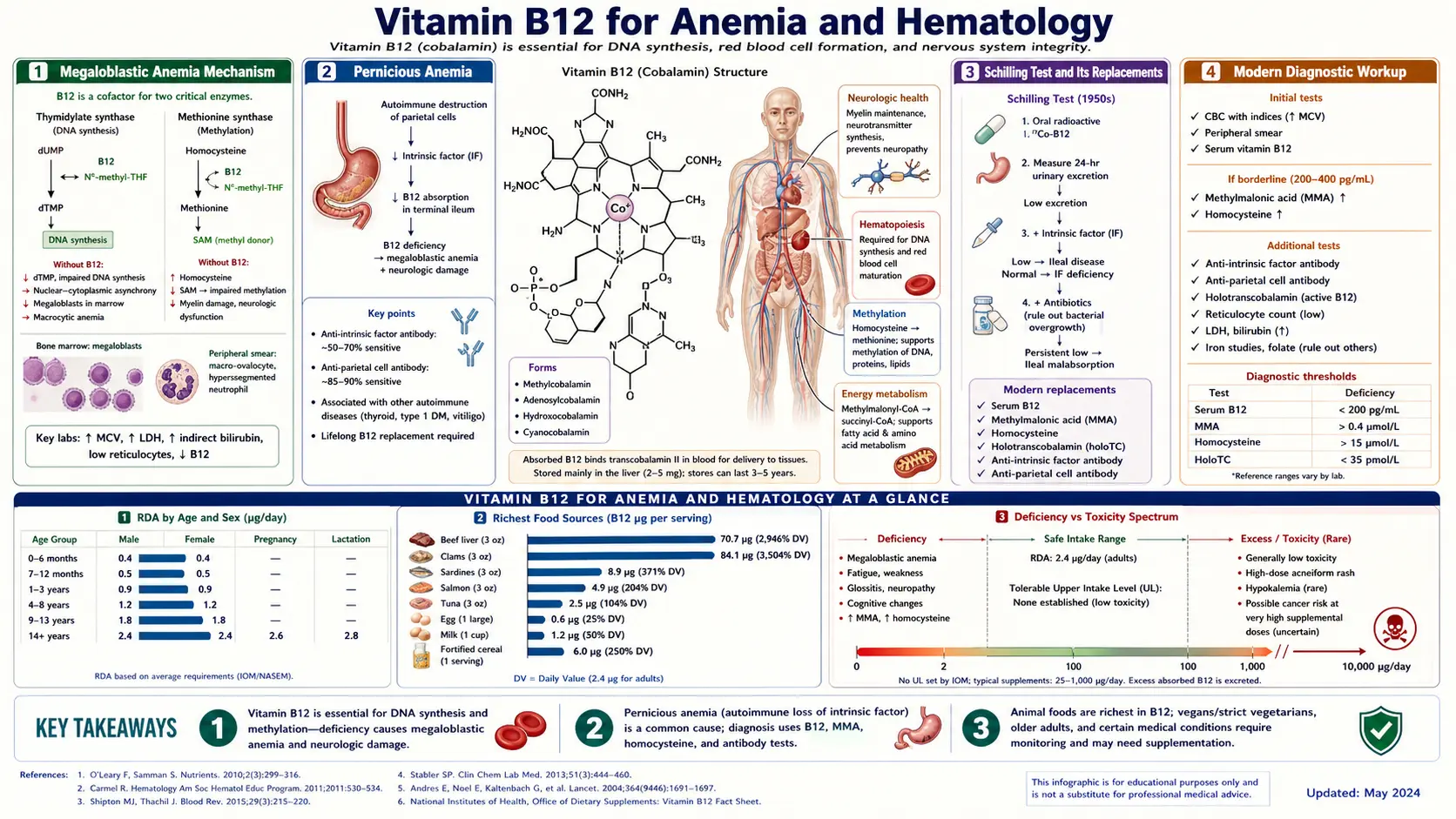
Megaloblastic Anemia Mechanism
Megaloblastic anemia is defined by abnormally large, immature red blood cell precursors in the bone marrow (megaloblasts) and abnormally large mature red blood cells in the peripheral blood (macrocytes, or more specifically macro-ovalocytes). The mean corpuscular volume (MCV) is elevated, typically above 100 fL and often above 110 fL in severe cases.
The underlying defect is impaired DNA synthesis in rapidly dividing cells. Erythroblasts in the bone marrow are among the fastest-dividing cells in the body — producing roughly 200 billion new red blood cells every day in a healthy adult. This proliferative burst requires intact synthesis of thymidine, one of the four nucleotide building blocks of DNA. Thymidine is made by the methylation of deoxyuridine monophosphate (dUMP) to deoxythymidine monophosphate (dTMP) by the enzyme thymidylate synthase, which uses 5,10-methylenetetrahydrofolate as its methyl donor.
Here is where B12 enters the picture. The body's largest pool of folate is in the form of 5-methyltetrahydrofolate (5-MTHF). To enter the thymidine synthesis pathway, 5-MTHF must first donate its methyl group to homocysteine via the methionine synthase reaction, regenerating tetrahydrofolate (THF), which can then be reconverted to 5,10-methylenetetrahydrofolate for thymidine synthesis. Methionine synthase requires B12. When B12 is deficient, 5-MTHF cannot donate its methyl group, folate becomes trapped in the methylated form (the "methyl trap"), and the active folate pool needed for thymidine synthesis collapses.
The consequence: erythroblasts cannot synthesize enough thymidine to replicate their DNA. They continue to grow and accumulate cytoplasmic contents (including hemoglobin), but their nuclei lag behind. The result is a giant cell with abundant cytoplasm and an immature, oversized nucleus — the megaloblast. Many of these cells die in the bone marrow (ineffective erythropoiesis); those that mature into circulating red blood cells are oversized, oval-shaped, and short-lived. The patient becomes profoundly anemic despite a hyperactive bone marrow.
Because the defect is upstream of all three blood-cell lineages, severe B12 deficiency can also produce leukopenia (low white blood cells), thrombocytopenia (low platelets), and ultimately pancytopenia (low everything). White blood cells show the same nuclear immaturity defect — hypersegmented neutrophils (5 or more nuclear lobes) are an early and sensitive sign of the megaloblastic process, often present before MCV elevation becomes obvious.
Folate deficiency produces an identical hematological picture through a different mechanism (depletion of folate substrate). This is why supplementing folate alone can correct the anemia of B12 deficiency — folate bypasses the methyl trap by providing fresh folate substrate downstream. The danger: folate supplementation corrects the blood picture but does not fix the methylation defect, so neurological damage continues to progress silently while the patient and clinician think the problem is resolved. This is one of the most important principles in B12 medicine and the reason every patient with macrocytic anemia must have both B12 and folate measured before folate supplementation is started.
Pernicious Anemia
Pernicious anemia (PA) is the classic and most studied cause of B12 deficiency. It is an autoimmune disease in which the immune system attacks the gastric parietal cells (the cells of the stomach that produce intrinsic factor and stomach acid) or intrinsic factor itself. Two antibody types are characteristic:
- Anti-parietal cell antibodies (APCA) — present in ~85% of PA patients but also present in 5-10% of the healthy elderly population without disease. Sensitive but not specific.
- Anti-intrinsic factor antibodies (AIFA) — present in 50-70% of PA patients and highly specific for the disease. Very rarely found outside PA. Less sensitive but more specific.
Two clinical sub-types of anti-IF antibody exist: type I (blocks B12 binding to IF) and type II (blocks the IF-B12 complex from binding to its ileal receptor). Either pattern produces the same clinical result: B12 cannot be absorbed through the normal physiological pathway, and over years to decades the patient's hepatic B12 stores deplete, leading to the classic triad of macrocytic anemia + neurological symptoms + glossitis.
PA is strongly associated with other autoimmune conditions, particularly:
- Hashimoto's thyroiditis (most common association)
- Graves' disease
- Vitiligo
- Type 1 diabetes mellitus
- Addison's disease
- Premature ovarian failure
- Primary biliary cholangitis
The "polyglandular autoimmune syndrome" clusters explain why a patient with one autoimmune disease should be screened for B12 deficiency periodically, and why a patient with newly diagnosed pernicious anemia should have thyroid function, fasting glucose, and adrenal function checked.
PA also carries a significantly elevated risk of gastric cancer (approximately 2-3 fold), related to the chronic atrophic gastritis that develops from autoimmune parietal cell destruction. Endoscopic surveillance every 3-5 years is recommended in established PA, particularly if the diagnosis was made before age 50.
Treatment is lifelong B12 supplementation — the underlying autoimmune disease does not remit, and the intrinsic factor deficiency does not reverse. Without sustained B12 replacement, the anemia and neurological complications return inexorably.
Schilling Test and Its Replacements
The Schilling test was the gold standard for diagnosing B12 absorption defects from the 1950s through the early 2000s. It involved giving the patient an oral dose of radioactive cyanocobalamin (cobalt-57 or cobalt-58 labeled), followed by a large parenteral "flushing" dose of unlabeled B12. The radioactive B12 absorbed from the gut would be excreted in the urine over 24 hours; the amount of urinary radioactivity reflected the patient's intrinsic absorptive capacity.
If urinary excretion was low, suggesting absorption defect, the test was repeated with intrinsic factor added to the oral dose. Normalization indicated pernicious anemia (intrinsic factor deficiency); persistent low excretion indicated ileal disease or bacterial overgrowth.
The Schilling test was retired in most clinical settings in the early 2000s because:
- The radioactive material became difficult to source
- Better and safer alternatives became available
- Treatment decisions can usually be made without precisely localizing the absorption defect
The modern replacements:
- Anti-intrinsic factor antibodies (AIFA) — highly specific for pernicious anemia. A positive AIFA in a patient with B12 deficiency essentially confirms PA without needing further testing.
- Anti-parietal cell antibodies (APCA) — sensitive but less specific; suggests autoimmune gastritis and supports PA diagnosis when combined with other findings.
- Serum gastrin — markedly elevated in PA (typically >500 pg/mL) because parietal cell destruction removes the negative feedback that normally suppresses G-cell gastrin secretion.
- Pepsinogen I and the pepsinogen I/II ratio — pepsinogen I is low in PA reflecting parietal cell loss; the ratio is suppressed.
- Holotranscobalamin (holoTC) — measures the bioavailable B12 fraction; low in any B12 deficiency.
- Upper endoscopy with biopsy — demonstrates the body-predominant atrophic gastritis characteristic of PA; rules out gastric cancer.
For most patients, the combination of clinical picture (macrocytic anemia, neurological symptoms, autoimmune background), elevated MMA, and positive anti-IF antibody is sufficient to confirm pernicious anemia without invasive testing.
Modern Diagnostic Workup
The recommended workup for suspected B12 deficiency anemia:
- Complete blood count (CBC) with differential and peripheral blood smear — assess hemoglobin, MCV, MCH, white cell count, platelet count, and morphology. Look for macrocytosis, oval macrocytes, hypersegmented neutrophils.
- Serum B12 — the starting point. <200 pg/mL is clearly deficient; 200-400 pg/mL is borderline; 400-900 pg/mL is normal; >900 pg/mL is supraphysiological (usually supplementation).
- Serum folate and red cell folate — rule out concurrent folate deficiency (which is also a cause of macrocytic anemia). Always check before starting folate supplementation.
- Methylmalonic acid (MMA) — the most specific functional marker of B12 deficiency. Elevated MMA in the presence of borderline or low B12 confirms functional deficiency.
- Homocysteine — elevated in B12 deficiency, but also elevated in folate deficiency, B6 deficiency, and renal insufficiency. Sensitive but not specific.
- Reticulocyte count — usually inappropriately low in megaloblastic anemia (because erythropoiesis is ineffective).
- LDH and indirect bilirubin — elevated due to intramedullary hemolysis (red cell precursors dying in the bone marrow).
- Iron studies — rule out concurrent iron deficiency, which can mask the macrocytosis of B12 deficiency.
- TSH — rule out hypothyroidism, which is commonly associated with PA and also causes macrocytosis.
- If B12 deficiency confirmed: anti-intrinsic factor antibodies, anti-parietal cell antibodies, and serum gastrin to evaluate for pernicious anemia.
The pattern that confirms B12 deficiency anemia: low or borderline B12, elevated MMA, elevated homocysteine, macrocytic anemia with hypersegmented neutrophils. Pernicious anemia is confirmed by positive anti-IF antibody and/or elevated gastrin with hypopepsinogenemia.
IM Injection Protocols
Intramuscular B12 injection has been the standard treatment for pernicious anemia and severe B12 deficiency for over 70 years. The British Society for Haematology and most US hematology consensus protocols use a version of the following:
Induction Phase (severe deficiency with neurological symptoms)
- Hydroxocobalamin 1000 mcg IM daily for 1-2 weeks until clinical improvement begins
- OR cyanocobalamin 1000 mcg IM daily for 1-2 weeks (cheaper, equally effective hematologically, possibly less optimal for neurological involvement)
- Continue with the next phase based on response
Induction Phase (no neurological symptoms, hematological only)
- Hydroxocobalamin 1000 mcg IM three times weekly for 2 weeks
Continuation Phase
- Hydroxocobalamin 1000 mcg IM weekly until hematological parameters fully normalize (typically 4-8 weeks)
Maintenance Phase
- Hydroxocobalamin 1000 mcg IM every 2-3 months for life (UK NHS standard: every 3 months; US standard: every 1-3 months depending on individual response and severity of disease)
- OR cyanocobalamin 1000 mcg IM monthly for life
- OR transition to high-dose oral or sublingual B12 (see Berlin protocol below) if patient prefers and response is adequate
Hydroxocobalamin is preferred over cyanocobalamin for maintenance in Europe because its longer tissue retention allows less frequent dosing (every 2-3 months vs monthly for cyanocobalamin). Hydroxocobalamin is now widely available in the US as well; ask the prescribing physician to specify the form.
Injection technique: deep IM into the deltoid or vastus lateralis. Most patients can be trained to self-inject after the induction phase, dramatically reducing the burden of treatment. Subcutaneous injection (less painful, easier to self-administer) has been shown to produce equivalent absorption in several recent studies and is now used in some practices.
High-Dose Oral (Berlin Protocol)
The single most important development in B12 medicine over the past 30 years is the demonstration that high-dose oral B12 (1000-2000 mcg/day) works even in pernicious anemia. This was first established systematically in the "Berlin protocol" and subsequent randomized trials.
The biological basis: although the great majority of dietary B12 absorption requires intrinsic factor and the ileal cubilin-amnionless receptor, a small fraction (1-2%) of any oral B12 dose can be absorbed by simple passive diffusion across the intestinal mucosa, distributed throughout the small intestine. The percentage is tiny but the absolute amount becomes clinically meaningful at high doses: 2% of 2000 mcg is 40 mcg/day, which substantially exceeds the daily requirement (2.4 mcg) and is sufficient to maintain physiological serum B12 levels indefinitely.
The Berlin protocol and its successors have established:
- Oral cyanocobalamin or methylcobalamin 1000-2000 mcg/day is equivalent to IM 1000 mcg monthly for maintenance in pernicious anemia
- Hematological parameters (Hb, MCV, reticulocyte count) normalize equivalently with oral and IM therapy
- Serum B12 levels are similar or higher with daily oral high-dose than with monthly IM
- Methylmalonic acid normalizes equivalently
- The vast majority of pernicious anemia patients can be successfully managed with oral therapy alone after an initial IM induction
Practical Berlin-style protocol:
- Induction (1-2 months): Hydroxocobalamin or cyanocobalamin 1000 mcg IM every other day for 1-2 weeks, then weekly for 4-6 weeks. Use IM during this phase to ensure rapid tissue saturation, particularly if neurological symptoms are present.
- Transition to oral: After hematological response is established and patient is clinically stable, switch to oral methylcobalamin 2000 mcg daily.
- Maintenance: Oral methylcobalamin or cyanocobalamin 1000-2000 mcg daily indefinitely. Re-check serum B12 and MMA every 6-12 months to confirm adequacy.
- Patient choice: patients who prefer monthly IM injections can continue them indefinitely — both approaches are clinically valid.
Adherence is the key issue with oral therapy — daily lifelong supplementation is harder to remember than a quarterly injection. For patients with reliable adherence, oral is more convenient, cheaper, and equally effective.
Response Monitoring
The hematological response to B12 repletion follows a predictable timeline:
- Days 1-3: Subjective improvement in energy and well-being begins. Methylmalonyl-CoA levels begin to fall.
- Days 3-7: Reticulocyte count rises (reticulocytosis) as the bone marrow is suddenly able to produce competent red cells from the accumulated mature precursors. Peak reticulocyte response is typically at day 5-10 and confirms that the diagnosis was correct.
- Weeks 2-4: Hemoglobin begins to rise; MCV begins to fall toward normal; hypersegmented neutrophils disappear; LDH and indirect bilirubin normalize as ineffective erythropoiesis resolves.
- Weeks 4-8: Hemoglobin reaches the normal range; MCV normalizes; full hematological recovery achieved.
- Months 2-6: If neurological symptoms were present, gradual neurological recovery proceeds as discussed in the Nerve Health page.
If reticulocytosis does not occur within 10 days of starting parenteral B12, the diagnosis should be reconsidered. Failure to respond suggests:
- Concurrent iron deficiency (most common cause of failed reticulocyte response — check iron studies and supplement if needed)
- Concurrent folate deficiency (check serum folate)
- Concurrent thyroid disease
- Bone marrow disease (myelodysplastic syndrome can present with macrocytosis and pancytopenia and does not respond to B12)
- Wrong diagnosis
Monitoring during maintenance: check serum B12, MMA, and CBC at 3 months, 6 months, then annually if stable. Patients on oral maintenance should have at least one repeat MMA at 6-12 months after switching to confirm continued adequacy.
Combined Iron + B12 + Folate Deficiency
One of the most clinically important presentations is combined deficiency: simultaneous iron, B12, and/or folate deficiency. This is particularly common in:
- Elderly patients with atrophic gastritis (low iron absorption and low B12 absorption simultaneously)
- Patients with celiac disease, Crohn's disease, or post-bariatric surgery
- Patients with chronic alcohol use disorder
- Pregnant women with poor nutritional baseline
- Patients with chronic blood loss from any cause
The hematological picture in combined deficiency can be confusing — iron deficiency causes microcytic anemia (low MCV), while B12/folate deficiency causes macrocytic anemia (high MCV). The two opposing effects can produce a normal-appearing MCV (the so-called "dimorphic" picture) that masks both deficiencies. Examination of the peripheral blood smear is critical: a dimorphic population of small hypochromic cells alongside large oval macrocytes is the giveaway.
Treatment requires addressing each deficiency separately:
- Iron repletion (oral ferrous sulfate 325 mg or other iron form, ideally with vitamin C for absorption, taken on an empty stomach away from coffee/tea/dairy)
- B12 repletion (as above)
- Folate repletion (folic acid 1-5 mg/day, or methylfolate 1-7.5 mg/day in patients with MTHFR variants)
- If concurrent thyroid disease is present, address it as well
Iron deficiency frequently coexists with B12 deficiency because both require gastric acid for proper absorption, and both rise in the same at-risk populations (elderly, post-gastrectomy, atrophic gastritis, vegan/vegetarian). Always check iron studies in any B12-deficient patient, and check B12 in any iron-deficient patient over age 50.
Cautions
- Hypokalemia during induction — severe pernicious anemia patients can develop dangerously low potassium during rapid hematological response. Newly formed red cells take potassium into the intracellular compartment, dropping serum levels. Check potassium during the first 1-2 weeks of treatment and supplement if needed.
- Hypophosphatemia — similar mechanism; rapid cell proliferation depletes serum phosphate. Less common than hypokalemia but documented.
- Iron deficiency unmasked — B12 repletion drives a burst of erythropoiesis that consumes iron rapidly. Latent iron deficiency may become symptomatic. Check iron studies at week 2-4 if hemoglobin response is sluggish.
- Folate masking — folic acid supplementation can correct the anemia of B12 deficiency without addressing the neurological problem. Always check B12 status before high-dose folate.
- Gastric cancer surveillance — pernicious anemia patients have 2-3 fold increased gastric cancer risk. Discuss endoscopic surveillance every 3-5 years with the physician, particularly for diagnosis before age 50.
- Thyroid screening — check TSH at PA diagnosis and periodically thereafter. Hashimoto's thyroiditis and PA cluster together.
- Family screening — first-degree relatives of PA patients should consider periodic B12 screening, particularly if they have other autoimmune disease.
Key Research Papers
- Minot GR, Murphy WP (1934). Nobel Prize for the discovery that liver therapy cures pernicious anemia. — PubMed
- Kuzminski AM et al. (1998). Effective treatment of cobalamin deficiency with oral cobalamin. Blood. — the seminal trial showing oral B12 works in pernicious anemia. — PubMed
- Bolaman Z et al. (2003). Oral vs intramuscular cobalamin in megaloblastic anemia: a single-center, prospective, randomized trial. Clin Ther. — PubMed
- Vidal-Alaball J et al. (2005). Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev. — PubMed
- Toh BH et al. (1997). Pernicious anemia. NEJM. — PubMed
- Lahner E, Annibale B (2009). Pernicious anemia: new insights from a gastroenterological point of view. World J Gastroenterol. — PubMed
- British Society for Haematology guidelines on cobalamin and folate deficiency (Devalia 2014). — PubMed
- Annibale B et al. (1999). Atrophic body gastritis: distinct features associated with Helicobacter pylori infection. Helicobacter. — PubMed
- Carmel R (2008). How I treat cobalamin (vitamin B12) deficiency. Blood. — PubMed
- Hvas AM, Nexo E (2006). Diagnosis and treatment of vitamin B12 deficiency — an update. Haematologica. — PubMed
- Stabler SP (2013). Vitamin B12 deficiency. NEJM. — PubMed
- Sun AL et al. (2018). Risk of gastric cancer in pernicious anemia: a meta-analysis. Eur J Cancer Prev. — PubMed
PubMed Topic Searches
- PubMed: pernicious anemia intrinsic factor antibody
- PubMed: megaloblastic anemia B12 folate
- PubMed: oral vs IM B12 pernicious anemia
- PubMed: Schilling test cobalamin absorption
- PubMed: hydroxocobalamin pernicious anemia maintenance
Connections
- Vitamin B12’s Impossible Journey — interactive animation
- Vitamin B12 Overview
- B12 Benefits Hub
- B12 for Nerve Health & Neuropathy
- B12 for Cognition & Methylation
- B12 for Vegans & Absorption
- B12 Deficiency Diagnosis
- Anemia
- Complete Blood Count
- Vitamin B12 Test
- Homocysteine
- Iron
- Vitamin B9 (Folate)
- Hashimoto's Thyroiditis
- Celiac Disease
- Crohn's Disease
- SIBO
- Fatigue
- Pernicious Anemia — the autoimmune loss of intrinsic factor behind the classic B12-deficiency anemia.