Liver Phase 1 and Phase 2 Biotransformation
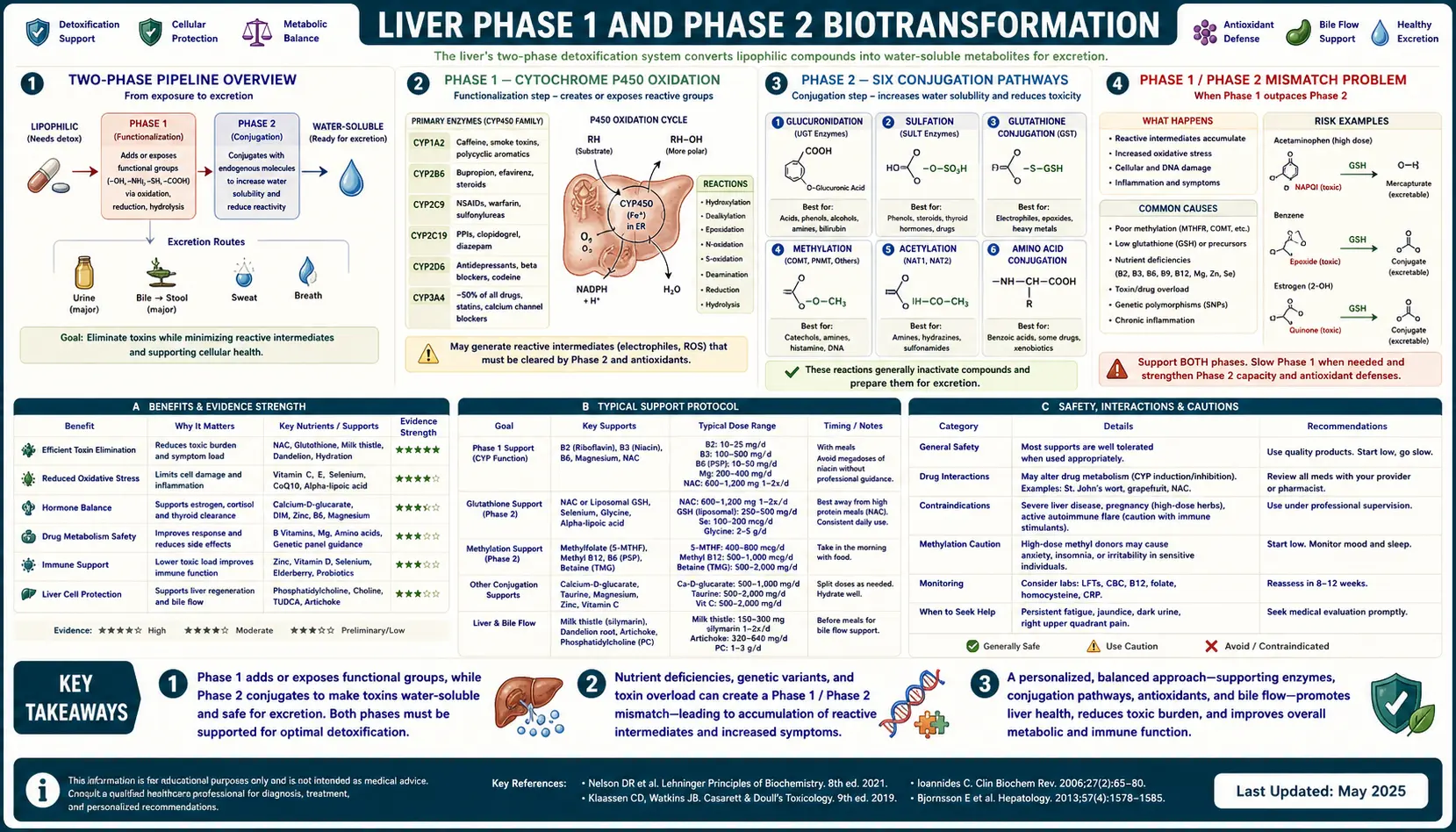
The liver runs a two-phase biotransformation pipeline that processes virtually every fat-soluble xenobiotic the body encounters — pharmaceutical drugs, alcohol, caffeine, hormones, pesticide residues, plasticizer leachates, mycotoxins, and combustion-byproduct aromatic hydrocarbons. Phase 1 is the cytochrome P450 (CYP450) oxidation cascade that adds reactive functional groups (-OH, -NH2, -COOH) to make the molecule more polar. Phase 2 is the conjugation cascade that attaches a large water-soluble group (glucuronic acid, sulfate, glutathione, glycine, acetyl, methyl) to make the molecule excretable in bile or urine. When Phase 1 outpaces Phase 2 — common in fast acetylators, in glutathione depletion, and during high alcohol or pharmaceutical load — the intermediate metabolites are often more reactive and more toxic than the original parent compound. Supporting both phases with the right cofactors is the foundation of any rational detoxification protocol.
Table of Contents
- The Two-Phase Pipeline Overview
- Phase 1: Cytochrome P450 Oxidation
- Phase 2: The Six Conjugation Pathways
- The Phase 1 / Phase 2 Mismatch Problem
- Genetic Polymorphisms (CYP, NAT2, COMT, GST)
- Nutrient Cofactor Requirements
- Supportive Foods, Herbs, and Supplements
- Drug-Drug-Food Interactions (the Practical Stakes)
- Testing Phase 1 / Phase 2 Function
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
The Two-Phase Pipeline Overview
The fundamental chemistry problem the liver solves is this: most xenobiotic toxins are fat-soluble (lipophilic), which is exactly why they cross cell membranes and accumulate in adipose tissue. The body excretes waste in two water-based fluids — urine and bile. To get a fat-soluble molecule into a water-based excretion stream, it must first be chemically transformed into something water-soluble.
That transformation is split into two consecutive enzymatic steps that take place primarily in hepatocyte smooth endoplasmic reticulum:
- Phase 1 (Functionalization) — cytochrome P450 enzymes add a reactive functional group (hydroxyl, amine, carboxyl) to the molecule. This is almost always an oxidation, and it almost always generates a reactive oxygen species (ROS) as a byproduct. The Phase 1 metabolite is usually more chemically reactive than the parent compound, and often more toxic. Phase 1 alone is not detoxification — it is activation.
- Phase 2 (Conjugation) — a large polar molecule (glucuronic acid, sulfate, glutathione, glycine, acetyl, methyl) is enzymatically attached to the Phase 1 functional group. The conjugated molecule is much more water-soluble, much less reactive, and now small enough to leave through the kidney's glomerulus or large enough to be actively pumped into bile by the canalicular transporters MRP2 and BSEP.
A third stage, sometimes called Phase 3 (transport), encompasses the ATP-driven efflux pumps (P-glycoprotein, MRP2, BCRP) that actively move the conjugated metabolite across the apical hepatocyte membrane into bile, or across the renal tubule cell into urine. Phase 3 is where many of the consequential drug-drug interactions actually occur, because P-glycoprotein in particular handles a huge fraction of pharmaceutical molecules.
Phase 1: Cytochrome P450 Oxidation
The cytochrome P450 superfamily is a set of ~57 functional human heme-thiolate enzymes that share a common reaction template: they use molecular oxygen and NADPH to insert one oxygen atom into a substrate while releasing one water molecule. The name "P450" refers to the 450-nm UV absorption peak of the reduced carbon-monoxide-bound enzyme.
For xenobiotic detoxification, the dominant CYPs are:
- CYP3A4 — metabolizes ~50% of all prescription drugs; the workhorse, expressed in both liver and small intestine. Induced by St John's Wort, rifampin, and the steroid hormones; inhibited by grapefruit furanocoumarins (bergamottin and 6',7'-dihydroxybergamottin), ketoconazole, ritonavir, clarithromycin.
- CYP2D6 — ~25% of drugs (codeine, tramadol, tamoxifen, many antidepressants, many antipsychotics, beta-blockers). Famously polymorphic — populations divide into poor, intermediate, extensive, and ultra-rapid metabolizers, with up to 13 functional gene copies in some Ethiopian and Saudi Arabian populations.
- CYP2C9 — warfarin, phenytoin, many NSAIDs, sulfonylurea diabetes drugs.
- CYP2C19 — proton pump inhibitors (omeprazole), clopidogrel activation (a known polymorphism reason for stent thrombosis in poor metabolizers).
- CYP1A2 — caffeine, theophylline, many polycyclic aromatic hydrocarbons (induced by char-grilled meat and cigarette smoke).
- CYP2E1 — ethanol, acetone, halogenated solvents (chloroform, vinyl chloride), the dangerous CYP that converts acetaminophen to NAPQI, the metabolite that kills the liver in overdose.
Phase 1 generates reactive intermediates that, if not promptly handled by Phase 2, will covalently bind to cellular proteins, lipids, and DNA — producing the carcinogenicity, hepatotoxicity, and idiosyncratic drug reactions that often define a compound's toxicity profile.
Phase 2: The Six Conjugation Pathways
Phase 2 attaches a polar group to the Phase 1 metabolite. There are six parallel pathways, each with its own enzyme family, its own substrate preferences, and its own cofactor requirement:
- Glucuronidation (UGT enzymes, cofactor UDP-glucuronic acid) — the highest-capacity Phase 2 pathway. Conjugates bilirubin, morphine, codeine, estrogens, acetaminophen, and many drugs. UGT1A1 polymorphisms cause Gilbert syndrome (mild bilirubin elevation in ~3-7% of the population).
- Sulfation (SULT enzymes, cofactor PAPS = 3'-phosphoadenosine-5'-phosphosulfate) — conjugates many small molecules, hormones, and phenolic compounds. PAPS is generated from cysteine and ATP, so sulfation is rate-limited by sulfur amino-acid intake (methionine, cysteine, taurine) and by ATP availability.
- Glutathione conjugation (GST enzymes, cofactor glutathione GSH) — the critical pathway for reactive electrophiles, alpha-beta unsaturated carbonyls, and the dangerous CYP2E1 metabolites including NAPQI from acetaminophen. Glutathione is the body's primary intracellular antioxidant and is depleted by alcohol, acetaminophen, oxidative stress, and chronic inflammation.
- Acetylation (NAT1, NAT2, cofactor acetyl-CoA) — conjugates aromatic amines and hydrazines (sulfa drugs, isoniazid, hydralazine, procainamide, caffeine). NAT2 has well-characterized "slow" and "fast" acetylator phenotypes that affect both drug clearance and bladder cancer risk from aromatic-amine exposures.
- Methylation (COMT, TPMT, PNMT, others; cofactor S-adenosylmethionine SAMe) — conjugates catecholamines, estrogens, thiopurine drugs, and many small molecules. SAMe is regenerated through the methylation cycle, which requires folate, B12, and B6. Common COMT polymorphisms (Val158Met) shift catecholamine and estrogen clearance.
- Amino acid conjugation (glycine, taurine, glutamine) — conjugates carboxylic acid xenobiotics including benzoic acid (food preservative) and salicylates. Glycine is the rate-limiter; a high carboxylic-acid load can deplete free glycine for other uses.
The Phase 1 / Phase 2 Mismatch Problem
The most clinically important pattern in liver biotransformation failure is not "low Phase 1" or "low Phase 2" in isolation — it is Phase 1 activity that exceeds Phase 2 capacity. This generates a pool of reactive intermediates that cannot be conjugated quickly enough, and that pool causes the cellular damage usually attributed to "the toxin" itself.
Several common scenarios produce this mismatch:
- Fast acetylator + high aromatic-amine exposure — NAT2 fast acetylators generate N-acetoxy intermediates of aromatic amines faster than other pathways can clear them; this is the mechanism for elevated bladder cancer risk in fast acetylators with occupational dye-industry exposure.
- CYP2E1 induction by chronic alcohol + acetaminophen — alcohol induces CYP2E1, which converts a higher fraction of an acetaminophen dose to the toxic intermediate NAPQI. NAPQI is normally conjugated and detoxified by glutathione, but chronic alcohol also depletes glutathione. The combination causes hepatotoxicity at acetaminophen doses far below the standard overdose threshold.
- CYP1A2 induction by char-grilled meat / smoking + low cruciferous vegetable intake — the polycyclic aromatic hydrocarbons (PAHs) in char and smoke are activated by CYP1A2 to mutagenic epoxides; cruciferous vegetables induce both glutathione S-transferases and UGTs that conjugate those epoxides. Without the Phase 2 induction, the Phase 1 activation is purely procarcinogenic.
- Estrogen metabolism through 4-hydroxylation — the 4-hydroxyestrogen intermediate is genotoxic if not promptly methylated by COMT. Slow COMT (Val158Met homozygotes) plus folate insufficiency leaves 4-hydroxyestrogen in circulation and is one mechanism proposed for increased estrogen-driven cancer risk.
The clinical implication is that "support Phase 1" and "support Phase 2" are not interchangeable. Adding a CYP inducer (like St John's Wort) without simultaneously supporting Phase 2 cofactors can worsen the toxic load by accelerating the activation step relative to the conjugation step.
Genetic Polymorphisms (CYP, NAT2, COMT, GST)
Biotransformation is one of the most genetically variable systems in human physiology. A short list of high-impact polymorphisms:
- CYP2D6 — null alleles (CYP2D6*4, *5) produce a poor-metabolizer phenotype in ~7% of Caucasians; ultra-rapid metabolizers with multiple gene copies (*1xN, *2xN) make up ~1-7% depending on ancestry (highest in East African and Saudi populations). Codeine ultra-rapid metabolizers convert codeine to morphine so fast they can experience opioid overdose at standard doses; this is the mechanism behind FDA warnings on codeine in nursing mothers.
- CYP2C19 — the *2 and *3 loss-of-function alleles produce poor-metabolizer phenotypes in ~3% of Caucasians and ~13-23% of East Asians. Clopidogrel (Plavix) requires CYP2C19 to convert from prodrug to active metabolite, so poor metabolizers have reduced anti-platelet effect and elevated stent thrombosis risk.
- NAT2 — the slow-acetylator phenotype is common (~40-60% of Caucasians, lower in East Asians). Isoniazid-induced hepatotoxicity, sulfa-drug allergy, and hydralazine-induced lupus are all enriched in slow acetylators.
- COMT Val158Met — the Met/Met homozygous variant produces a ~3-4x reduction in COMT enzyme activity, slowing catecholamine, estrogen, and L-DOPA methylation.
- GSTM1 and GSTT1 deletions — whole-gene deletions are common (~50% of Caucasians lack functional GSTM1; ~20% lack GSTT1) and are associated with elevated risk of several xenobiotic-driven cancers including bladder, lung, and colon.
- UGT1A1 (Gilbert syndrome) — the UGT1A1*28 promoter variant produces a ~30% reduction in UGT1A1 enzyme, causing benign unconjugated hyperbilirubinemia but also reduced clearance of irinotecan and a corresponding myelosuppression risk.
Commercial nutrigenomic panels (Genova Detoxigenomic Profile, 23andMe raw-data analyzers) report these polymorphisms, though clinical interpretation should always weigh the actual exposure context, not just the genotype.
Nutrient Cofactor Requirements
Each Phase 1 and Phase 2 enzyme requires specific cofactors. The complete cofactor map:
- Phase 1 (CYP450): NADPH (regenerated through the pentose phosphate pathway and ultimately requiring niacin, riboflavin), molecular oxygen, iron (heme), magnesium (electron transfer).
- Glucuronidation: UDP-glucose pathway derived from glucose; magnesium-dependent UDP-glucose dehydrogenase.
- Sulfation: ATP, methionine or cysteine (sulfate donor), molybdenum (sulfite oxidase regenerates sulfate from sulfite), B12.
- Glutathione conjugation: glutathione itself (synthesized from glutamate + cysteine + glycine), requiring cysteine as the rate-limiter; selenium for glutathione peroxidase; magnesium for the gamma-glutamylcysteine synthetase rate-limiting step.
- Acetylation: acetyl-CoA (derived from carbohydrate/fat metabolism), pantothenic acid (vitamin B5).
- Methylation: SAMe regenerated from methionine through the folate / B12 / B6 cycle; choline / betaine as backup methyl donors; magnesium for the methylation cycle enzymes.
- Amino acid conjugation: free glycine, taurine, glutamine pools; adequate protein intake.
A nutritionally adequate background diet supplies most of these in normal amounts, but high xenobiotic load (medication burden, alcohol, occupational exposure, mold exposure, chemotherapy) can deplete the rate-limiting cofactors faster than ordinary diet can replace them. The most commonly rate-limiting cofactors in clinical practice are glutathione (via cysteine/NAC), magnesium, and the methylation cycle B-vitamins (folate, B12, B6).
Supportive Foods, Herbs, and Supplements
Specific foods, herbs, and supplements have well-documented effects on Phase 1 and Phase 2:
- Cruciferous vegetables (broccoli, broccoli sprouts, kale, Brussels sprouts, cabbage) — sulforaphane and indole-3-carbinol activate Nrf2, the master transcription factor for Phase 2 enzymes. Broccoli sprouts contain ~100x more sulforaphane precursor (glucoraphanin) than mature broccoli. Daily intake measurably induces GST, UGT, and NQO1.
- Garlic and onions (allium family) — the organosulfur compounds (diallyl sulfide, diallyl disulfide) inhibit CYP2E1 (the dangerous acetaminophen-activating CYP) and induce Phase 2 conjugation enzymes.
- Milk thistle (silymarin / silibinin) — hepatoprotective via Kupffer cell modulation, antioxidant activity, and inhibition of inflammatory cytokine production. The intravenous formulation (Legalon SIL) is a recognized treatment for Amanita phalloides mushroom poisoning.
- Turmeric (curcumin) — induces Phase 2 detoxification enzymes including glutathione S-transferase and modulates Nrf2 signaling.
- Green tea (EGCG) — induces Phase 2 enzymes through Nrf2 activation; modest CYP1A2 inhibition.
- N-acetylcysteine (NAC) — cysteine donor for glutathione synthesis. FDA-approved as the antidote for acetaminophen overdose, given orally or intravenously to restore depleted glutathione.
- Glycine — rate-limiter for amino acid conjugation and a major component of glutathione. 3-5 g/day is commonly used as supportive supplementation.
- Methylation cofactors — methylfolate (5-MTHF) and methylcobalamin (methyl-B12) for individuals with MTHFR polymorphisms; betaine (trimethylglycine) as a methyl donor; B6 (P5P) as the active form.
Drug-Drug-Food Interactions (the Practical Stakes)
Liver biotransformation is the mechanism behind most clinically important drug interactions. A non-exhaustive list of consequential interactions:
- Grapefruit juice — the furanocoumarins (bergamottin and 6',7'-dihydroxybergamottin) irreversibly inactivate intestinal CYP3A4 for ~24 hours after a single 200-mL glass. Drug levels of statins (simvastatin, atorvastatin, lovastatin), calcium channel blockers (felodipine, nifedipine), some immunosuppressants (cyclosporine, tacrolimus), and many others can rise 2-10x.
- St John's Wort — potent inducer of both CYP3A4 and P-glycoprotein. Lowers serum levels of oral contraceptives (with breakthrough pregnancy reports), cyclosporine (graft rejection), warfarin (loss of anticoagulation), HIV protease inhibitors, and many SSRIs.
- Cigarette smoke (polycyclic aromatic hydrocarbons) — potent CYP1A2 inducer; smokers require ~30-50% higher doses of theophylline, clozapine, olanzapine, and caffeine to achieve equivalent serum levels. Smoking cessation can produce dangerous over-dosing of these drugs if doses are not adjusted.
- Rifampin — broad CYP and P-glycoprotein inducer; reduces serum levels of warfarin, oral contraceptives, statins, calcium channel blockers, and many anti-rejection drugs.
- Ritonavir — potent CYP3A4 inhibitor; used deliberately as a "boosting" agent to maintain serum levels of other HIV protease inhibitors. Also the reason for the long list of contraindicated medications with Paxlovid.
- Clarithromycin / erythromycin — CYP3A4 inhibitors; classic interaction with simvastatin produces rhabdomyolysis at standard simvastatin doses.
Anyone undertaking active liver-detox support while on multiple medications should review interactions with their prescriber, because supporting Phase 1 (inducer-like effect) can lower drug levels and supporting Phase 2 can raise the conjugated/inactive metabolite ratio for some drugs.
Testing Phase 1 / Phase 2 Function
Several laboratory approaches assess biotransformation capacity in clinical practice:
- Caffeine clearance test — oral caffeine load with timed salivary or urine measurement of caffeine and its metabolites; reports CYP1A2 activity and NAT2 acetylator phenotype.
- Urinary organic acid panels (Genova ION, NutrEval, Great Plains OAT) — report elevated benzoate, phenylacetate, or hippurate as proxies for amino acid conjugation load; elevated pyroglutamate as a marker of glutathione depletion.
- Detoxigenomic / nutrigenomic genotyping (Genova, 23andMe + Promethease) — reports CYP, GST, NAT2, COMT, and UGT polymorphisms.
- Plasma glutathione (reduced GSH and oxidized GSSG) — specialized labs (Doctor's Data, Genova); the GSH:GSSG ratio is a sensitive marker of systemic oxidative load.
- Liver enzymes (ALT, AST, GGT, ALP, bilirubin) — routine but coarse; elevated GGT in particular tracks with xenobiotic load and is a sensitive marker of hepatic oxidative stress.
Cautions and Contraindications
Several cautions apply to supporting Phase 1 / Phase 2 deliberately:
- Active narrow-therapeutic-window medication — warfarin, immunosuppressants (cyclosporine, tacrolimus), anti-rejection drugs, anti-seizure drugs (phenytoin, carbamazepine), oral contraceptives. CYP inducers (St John's Wort, milk thistle in some cases) and CYP inhibitors (grapefruit, some herbs) can change serum levels significantly. Coordinate with prescriber.
- Active acetaminophen use — particularly with concurrent alcohol, the safe daily acetaminophen dose drops well below the labeled 4 g/day. NAC supplementation may be protective.
- Active chemotherapy — antioxidant and Phase 2 inducer supplementation can theoretically reduce efficacy of chemo drugs that work through oxidative DNA damage. Coordinate timing with oncologist.
- Pregnancy — high-dose herbs and supplements should be reviewed; some are teratogenic or hormonally active.
- Glucose-6-phosphate dehydrogenase (G6PD) deficiency — reduced NADPH supply for Phase 1 and glutathione regeneration; certain "detox" interventions can trigger hemolysis.
Key Research Papers
- Guengerich FP, Cytochrome P450 and chemical toxicology — PubMed 18052394: Guengerich CYP toxicology
- Liska DJ, The detoxification enzyme systems Search PubMed
- Iyanagi T, Molecular mechanism of phase I and phase II drug-metabolizing enzymes Search PubMed
- Lieber CS, Cytochrome P-4502E1: its physiological and pathological role Search PubMed
- Egner PA et al., Rapid and sustainable detoxication of airborne pollutants by broccoli sprout beverage (Qidong randomized trial) — PubMed 24913818: Broccoli sprout Qidong trial
- Fahey JW et al., Broccoli sprouts and chemoprotective sulforaphane — PubMed 9294217: Fahey broccoli sprouts
- Saller R et al., The use of silymarin in the treatment of liver diseases — PubMed 11735632: Silymarin liver disease
- Hodges RE & Minich DM, Modulation of metabolic detoxification pathways using foods and food-derived components — PubMed 26167297: Hodges & Minich food detox
- Hu R et al., Cancer chemoprevention of intestinal polyposis in ApcMin/+ mice by sulforaphane, a natural product derived from cruciferous vegetable Search PubMed
- Smith MT, Advances in understanding benzene health effects and susceptibility (P450 + GST mechanism) — Search PubMed
- Hayes JD & Pulford DJ, The glutathione S-transferase supergene family — PubMed 8770536: GST supergene family
- Ingelman-Sundberg M, Pharmacogenomic biomarkers for drug toxicity (CYP variation review) — Search PubMed
Connections
- Detox Protocols Benefits Hub
- Detox Protocols (Main)
- Sweating and Sauna Therapy
- Binders: Charcoal & Chlorella
- Coffee Enemas
- N-Acetyl Cysteine (NAC)
- Glutathione
- Glycine
- Methionine
- Taurine
- Milk Thistle
- Turmeric
- Magnesium
- Selenium
- Molybdenum
- Vitamin B12
- Folate
- Vitamin B6
- Broccoli Sprouts
- Garlic
- Acetaminophen
- Alcohol
- Liver Enzymes