Binders: Charcoal, Chlorella, and Beyond
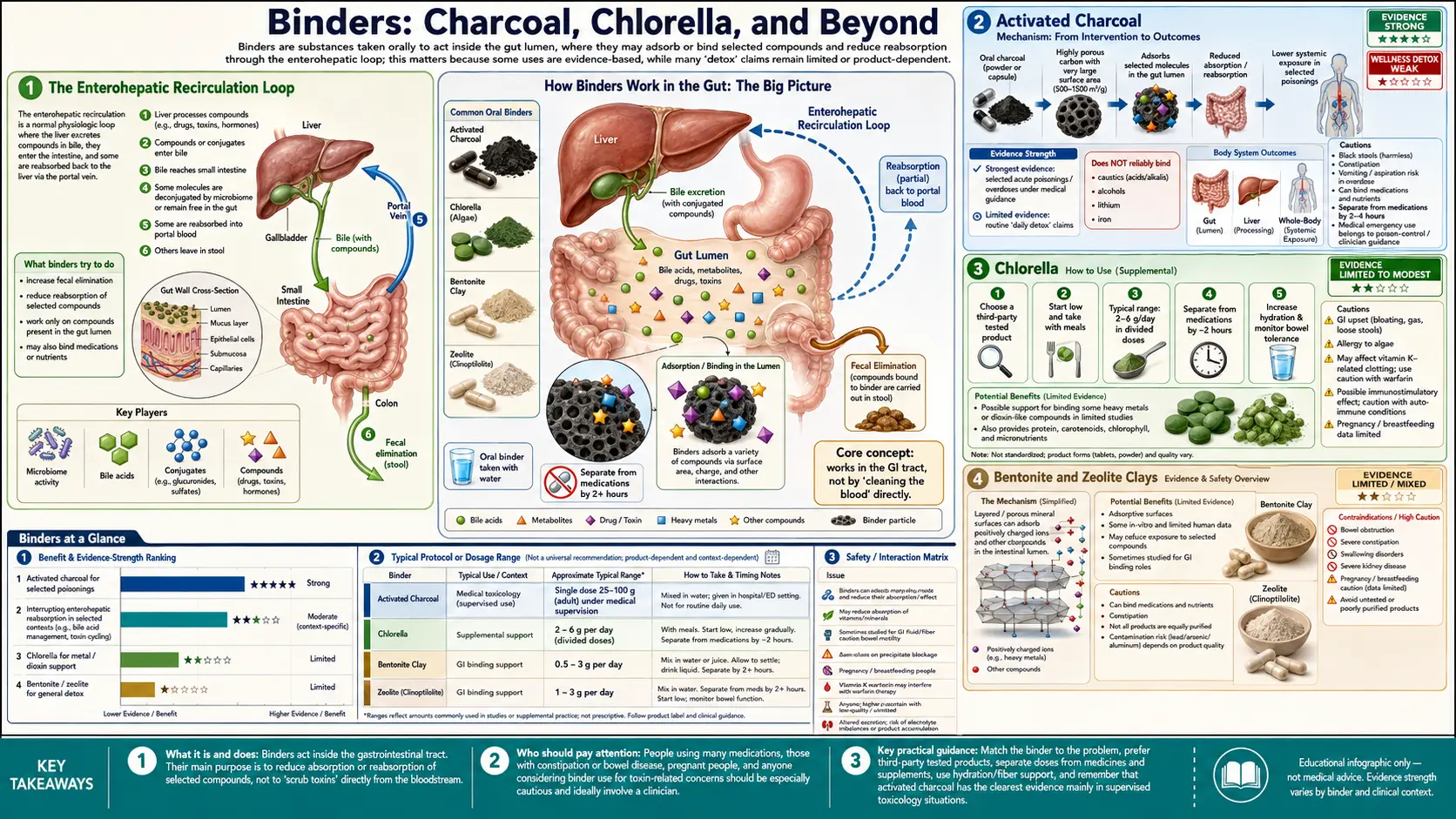
Intestinal binders are inert or semi-inert substances that physically adsorb toxins in the gut lumen and escort them out of the body in stool. They solve the enterohepatic recirculation problem: many liver-conjugated toxins are excreted in bile back into the small intestine, where they can be reabsorbed and recycled rather than eliminated. Activated charcoal — FDA-approved and the standard ER treatment for acute oral poisoning — has a surface area of roughly 1,000 m² per gram, giving it extraordinary nonspecific adsorption capacity. Chlorella binds heavy metals (especially methylmercury) through cell-wall cellulose-and-sporopollenin matrix. Bentonite clay (calcium montmorillonite) selectively binds aflatoxin and was validated in the Phillips trials in Ghana. Cholestyramine and colesevelam are prescription bile-acid sequestrants used by Shoemaker for chronic inflammatory response syndrome (CIRS) from mold biotoxins. Each binder has a different adsorption profile and a different appropriate use case — this page covers them all.
Table of Contents
- The Enterohepatic Recirculation Loop
- Activated Charcoal
- Chlorella
- Bentonite and Zeolite Clays
- Cholestyramine and Colesevelam
- Fiber, Pectin, and Chitosan
- Timing Relative to Food, Medications, and Other Supplements
- Constipation and Nutrient-Depletion Caveats
- Matching Binder to Toxin (Practical Use Cases)
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
The Enterohepatic Recirculation Loop
The liver excretes conjugated metabolites into bile, which empties into the duodenum at the ampulla of Vater. Bile is critical for fat digestion, so the body cannot afford to lose its bile acid pool; about 95% of bile acids and many of the conjugated metabolites carried in bile are reabsorbed in the terminal ileum, returned to the liver via the portal vein, and re-secreted — the enterohepatic circulation.
This is a problem for detoxification. Many toxins (mercury, lead, persistent organic pollutants, mold biotoxins, hormones in their conjugated form) are dumped into bile by the liver, then immediately reabsorbed in the ileum and returned to circulation. The body does the work of conjugation but never actually excretes the toxin — it just keeps recycling it.
Intestinal binders break the loop. A binder taken orally travels through the GI tract and arrives in the small intestine where biliary excretion happens. The binder physically adsorbs the conjugated toxin and prevents it from being reabsorbed. The bound complex then passes through the colon and exits in stool. This is the only reliable mechanism for getting many biliary-excreted toxins fully out of the body.
The phenomenon was first quantitatively demonstrated for bilirubin and digitalis in the 1970s: oral activated charcoal interrupts the enterohepatic circulation of those compounds and accelerates clearance. Subsequent work has extended the principle to mercury, mold biotoxins, ciguatera, and many other compounds.
Activated Charcoal
Activated charcoal is carbon that has been processed under high temperature with steam or chemical activation to create a microporous structure with enormous internal surface area — typically 800-1,500 m² per gram. A single tablespoon of activated charcoal has more surface area than a football field.
The medical pedigree is the most authoritative of any binder. Activated charcoal is FDA-approved and stocked in essentially every U.S. emergency department for the treatment of acute oral poisoning and drug overdose. The American Academy of Clinical Toxicology and the European Association of Poison Centres position statements (PubMed 15822755 single-dose, PubMed 10382554 multiple-dose) endorse single-dose oral activated charcoal as first-line for many oral poisonings ingested within 1-2 hours, and multiple-dose activated charcoal for selected ingestions (carbamazepine, dapsone, phenobarbital, quinine, theophylline) where enterohepatic recirculation extends clearance.
For chronic detoxification use (rather than acute poisoning), activated charcoal binds:
- Mycotoxins (aflatoxin, ochratoxin, mold byproducts in CIRS)
- Bile-recirculated heavy metals (mercury, lead)
- Drug residues
- Bacterial endotoxin (LPS, lipopolysaccharide)
- Many organic chemicals (BPA, phthalates, glyphosate to a limited extent)
Activated charcoal does NOT bind alcohol, lithium, iron, potassium, methanol, ethylene glycol, or strong acids/alkalis effectively — these require other interventions.
Practical dose: 500-2,000 mg taken 1-2 hours away from food, medications, and other supplements. Higher doses (10-50 g in water) are used for acute poisoning under medical supervision. Take with a full glass of water to minimize constipation. Form: capsules or loose powder; food-grade coconut or hardwood activated charcoal are commonly recommended for chronic use.
Chlorella
Chlorella is a single-celled freshwater green algae with a tough cellulose-and-sporopollenin cell wall. The cell wall contains chelating groups that bind heavy metals — particularly methylmercury (the form of mercury found in fish), aluminum, and cadmium — through ionic and chelating mechanisms. The cell wall must be mechanically broken (cracked-cell or broken-cell chlorella) for human digestion, or the cell passes through intact.
The research base on chlorella as a heavy-metal binder is smaller and lower-quality than for activated charcoal but is suggestive. The 2005 Pre-Park paper (PubMed 15735262) showed reduced cadmium absorption from the gut in chlorella-fed rats. The Uchikawa 2010 series demonstrated chlorella binding of methylmercury and dioxins in vitro and reduced fecal-to-urinary mercury ratio in chlorella-supplemented rats. Human clinical trials remain limited but include observational reports of reduced mercury and lead body burden in chlorella-treated dental-amalgam-removal patients.
Chlorella has secondary benefits beyond binding: it contains chlorophyll (which itself has modest binding affinity for some lipophilic toxins), B-vitamins including B12 (although chlorella B12 may be partially in pseudo-B12 form, with debated bioavailability), iron, magnesium, and complete amino acid profile.
Practical dose: 1-5 g/day, taken 1-2 hours away from food and medications. Chlorella has a noticeable taste; tablets are easier than powder for most people. Start at 500 mg/day and titrate up to assess tolerance (some people experience GI upset, headache, or "herxheimer-like" mobilization symptoms at higher doses).
Source matters: chlorella concentrates anything in its growing medium, including the heavy metals it's supposed to remove. Buy chlorella from manufacturers that publish independent third-party heavy-metal testing on every batch. Sun Chlorella, Yaeyama, and Prime Chlorella are commonly cited as well-tested brands.
Bentonite and Zeolite Clays
Bentonite (specifically calcium montmorillonite) and zeolite (clinoptilolite) are layered aluminosilicate clays with cation-exchange capacity that binds positively charged metal ions and certain mycotoxins. They are physically inert — they pass through the GI tract without absorption.
The strongest evidence is for bentonite (NovaSil) against aflatoxin. The Phillips group at Texas A&M validated NovaSil in animal studies and in the 2008 Ghana trial (PubMed 18286419), which demonstrated reduced aflatoxin biomarker levels in human subjects living in a region of endemic aflatoxin exposure. The mechanism is intercalation of aflatoxin into the clay layer.
Zeolite (clinoptilolite) has been promoted heavily in functional medicine for heavy metal detoxification, but the evidence base is thinner. The 2018 review (PubMed 29888846) found in-vitro evidence of heavy-metal binding but limited and inconsistent human clinical data.
Practical dose: 1-3 g/day food-grade bentonite or zeolite, mixed in water or capsule, taken 1-2 hours away from food and medications. Cosmetic-grade clay should not be ingested. Bentonite is the more conservative choice given the Phillips Ghana trial evidence; zeolite remains promising but less proven.
Cholestyramine and Colesevelam
Cholestyramine (Questran) and colesevelam (Welchol) are prescription bile-acid sequestrants — non-absorbable resins that bind bile acids in the gut and force the liver to make new bile from cholesterol, lowering serum LDL. They were originally developed in the 1960s-70s as cholesterol-lowering drugs and remain in use for that purpose, although they have been largely displaced by statins.
Their relevance for detoxification was identified by Ritchie Shoemaker in the early 2000s in his work on Chronic Inflammatory Response Syndrome (CIRS) from mold biotoxin exposure. Shoemaker observed that cholestyramine bound and removed mold biotoxins (ochratoxin, mycotoxins from water-damaged buildings) and that CIRS patients improved significantly on cholestyramine that they had not improved on other interventions. The Shoemaker protocol uses cholestyramine 4 g four times daily, separated from food, medications, and other supplements by at least 1-2 hours.
Cholestyramine also binds ciguatera toxin (PubMed 12132984), which is the marine biotoxin responsible for the most common form of seafood poisoning in tropical regions.
Colesevelam (Welchol) is a newer-generation bile-acid sequestrant that is better tolerated than cholestyramine (smaller dose, fewer GI side effects, less drug interaction) and is often used as the second-line in patients who cannot tolerate cholestyramine. The binding profile is similar but not identical; some practitioners prefer cholestyramine for mold biotoxin and reserve colesevelam for milder cases or for combination protocols.
Both drugs require prescription. Both have well-documented side effects: constipation, abdominal discomfort, and bile-acid-sequestration-related fat-soluble vitamin malabsorption (A, D, E, K) with prolonged use. Both have a long list of drug interactions because they will bind many oral medications taken in the same time window.
Fiber, Pectin, and Chitosan
Several food and supplement-grade fibers have binder-like properties:
- Modified citrus pectin (MCP) — a low-molecular-weight pectin derivative that has been shown to chelate lead, mercury, and arsenic in animal and human studies (PubMed 18435391). PectaSol-C is the most-studied brand. Dose 5-15 g/day in divided doses.
- Soluble fiber (psyllium, glucomannan) — not as potent as activated charcoal but adds bulk and binds bile acids and some lipophilic toxins. Useful for the constipation that often accompanies more aggressive binders.
- Chitosan — a polysaccharide derived from shellfish exoskeletons; binds fat-soluble compounds and some heavy metals. Contraindicated in shellfish allergy.
- Beta-glucan and inulin — prebiotic fibers that support beneficial gut bacteria; modest direct binding capacity but support overall intestinal health.
The classic Gerson protocol approach of "lots of fresh juice and high-fiber vegetables" works in part by providing pectin and fiber that bind biliary toxins in transit.
Timing Relative to Food, Medications, and Other Supplements
This is the single most-violated rule in binder use. Binders are nonspecific: they bind essentially anything in the gut lumen at the time, including:
- Prescription medications (statins, levothyroxine, anti-depressants, anti-seizure drugs)
- Vitamins and minerals
- Nutrients from food
- Beneficial polyphenols and antioxidants
- Probiotic organisms (charcoal in particular adsorbs bacteria)
The standard rule: take binders at least 1-2 hours away from food, medications, and other supplements. A common pattern is binder first thing in the morning (in water, before any food or pills), or at bedtime, well after dinner. If multiple binders are stacked, give each a separate window or take them together at one window.
Practical example schedule:
- 6:30 AM — activated charcoal 500 mg with 12 oz water
- 8:00 AM — breakfast, morning supplements, prescription medications
- 12:00 PM — lunch
- 3:00 PM — chlorella 2 g (more than 1 hr after lunch, more than 1 hr before any other supplement)
- 6:00 PM — dinner, evening supplements
- 10:00 PM — bentonite or second charcoal dose at bedtime
Cholestyramine and colesevelam have specific pharmacy guidance for medication timing — follow the prescribing information and consult the pharmacist for each medication.
Constipation and Nutrient-Depletion Caveats
Two recurring problems with binder use:
- Constipation. Every binder slows gut transit to some extent. Activated charcoal is the worst, bentonite is moderate, chlorella and modified citrus pectin are mild. Inadequate transit means the bound toxins sit in the gut and can re-release. The solution is adequate water intake (at least 16-20 oz per binder dose), magnesium (200-400 mg elemental at bedtime), and adequate fiber (vegetables, ground flax, psyllium husk if needed). If constipation develops, reduce binder dose or frequency until transit normalizes.
- Nutrient depletion. Chronic binder use can deplete fat-soluble vitamins (A, D, E, K), B-vitamins, and minerals. The Shoemaker protocol for CIRS explicitly recommends periodic monitoring of vitamin and mineral status during prolonged cholestyramine therapy. Supplementation should be timed in separate windows from the binder. For long-term binder users, periodic measurement of vitamin D, A, K2, B12, and folate is prudent.
Matching Binder to Toxin (Practical Use Cases)
- Acute oral poisoning — activated charcoal (medical supervision; 25-100 g in water in the ER setting).
- Mold / CIRS / water-damaged building exposure — cholestyramine (Shoemaker protocol); colesevelam as alternative; activated charcoal as adjunct or for milder cases.
- Mercury (chronic), including post-amalgam removal — chlorella plus activated charcoal, alongside sulfur amino acid support (NAC, alpha-lipoic acid) and selenium.
- Aflatoxin exposure (peanut, corn, or grain contamination) — bentonite (NovaSil) is the validated choice.
- Heavy metal mixed exposure — chlorella as primary, with modified citrus pectin and activated charcoal as adjuncts.
- Ciguatera fish poisoning — cholestyramine (validated in PubMed 12132984).
- Endotoxin / SIBO die-off / Lyme herxheimer — activated charcoal at the time of bacterial-die-off symptoms can blunt the inflammatory response.
- BPA / phthalate / industrial chemical exposure — activated charcoal plus sauna for parallel dermal route; supportive Phase 1/Phase 2 nutrition.
- General "background" detoxification — modified citrus pectin and chlorella in lower doses, paired with adequate fiber from whole food sources.
Cautions and Contraindications
- Bowel obstruction or significant constipation — binders can worsen obstruction; do not use during active obstruction.
- Inflammatory bowel disease in flare — binders may irritate inflamed mucosa; use cautiously.
- Multiple prescription medications — coordinate timing carefully; consider whether binder use is appropriate at all during medication titration windows.
- Pregnancy and lactation — activated charcoal is generally considered acceptable for acute use; routine detoxification protocols during pregnancy require careful clinical review.
- Pediatric use — only under medical supervision; dose adjustments required.
- Shellfish allergy — avoid chitosan (derived from shrimp/crab exoskeleton).
- Iodine allergy / thyroid disorders — chlorella from saltwater sources can contain iodine; freshwater chlorella has minimal iodine.
- Aluminum exposure concern — some lower-quality clay sources may contain elevated aluminum; choose tested brands.
Key Research Papers
- American Academy of Clinical Toxicology, Single-dose activated charcoal position statement Search PubMed
- AACT, Multiple-dose activated charcoal position statement Search PubMed
- Uchikawa T et al., Chlorella binding of methylmercury and dioxins Search PubMed
- Pre-Park K et al., Chlorella reduces cadmium absorption in rats Search PubMed
- Phillips TD et al., Calcium montmorillonite clay (NovaSil) animal aflatoxin studies Search PubMed
- Phillips TD et al., Ghana NovaSil human aflatoxin trial Search PubMed
- Shoemaker RC, Cholestyramine for chronic biotoxin illness (CIRS) PubMed: Shoemaker cholestyramine CIRS
- Lehane L & Lewis RJ, Ciguatera fish poisoning and cholestyramine treatment Search PubMed
- Eliaz I, Modified citrus pectin (PectaSol-C) for heavy metal chelation Search PubMed
- Clinoptilolite (zeolite) detoxification review Search PubMed
- Merrill JC et al., Chlorella supplementation and mercury post-amalgam clearance PubMed: Chlorella post-amalgam
- Volkheimer G, Persorption of microparticles and binder mechanism PubMed: Persorption mechanism
Connections
- Detox Protocols Benefits Hub
- Detox Protocols (Main)
- Liver Phase 1 and Phase 2
- Sweating and Sauna Therapy
- Coffee Enemas
- Chlorella
- Spirulina
- Activated Charcoal
- Bentonite Clay
- Mold (Mycotoxins)
- Mercury
- Lead
- Aflatoxin
- Heavy Metals
- CIRS (Chronic Inflammatory Response Syndrome)
- N-Acetyl Cysteine
- Selenium
- Magnesium
- Heavy Metal Testing
- Mycotoxin Testing