Coffee Enemas
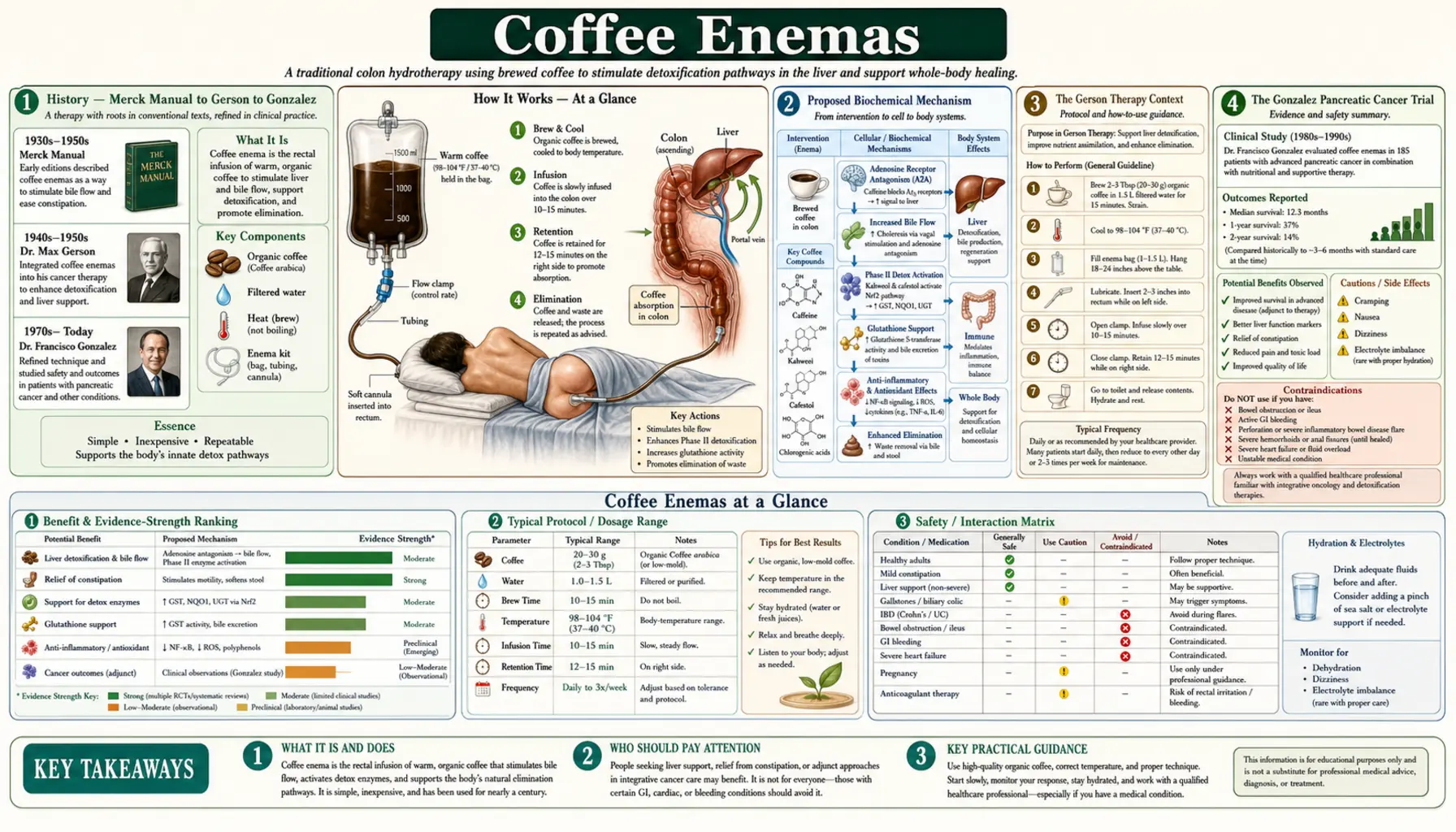
Coffee enemas are the most polarizing intervention in the detoxification toolkit — embraced as a cornerstone of the Gerson protocol since the 1940s, listed in the Merck Manual through the 1972 edition, formally revived by Nicholas Gonzalez at Columbia for pancreatic cancer in the 1990s and 2000s, and dismissed in much of conventional medicine as unsupported folk practice. The proposed biochemical mechanism is real and partially documented: caffeine and palmitic acid esters from coffee, absorbed through the hemorrhoidal veins, travel via the portal circulation to the liver where they upregulate glutathione S-transferase activity and stimulate bile flow. The clinical evidence remains limited; rigorous controlled trials have not been done at the scale that would settle the question definitively. This page covers the history, proposed mechanism, available clinical evidence, safety considerations (electrolyte risk, rare bowel perforation reports), and the standard preparation protocol followed by Gerson and Gonzalez practitioners.
Table of Contents
- History — Merck Manual to Gerson to Gonzalez
- Proposed Biochemical Mechanism
- The Gerson Therapy Context
- The Gonzalez Pancreatic Cancer Trial
- Available Clinical Evidence (and Gaps)
- Preparation Protocol (the Standard Recipe)
- Administration Procedure
- Frequency and Duration
- Cautions, Adverse Events, and Contraindications
- Key Research Papers
- Connections
- Featured Videos
History — Merck Manual to Gerson to Gonzalez
Coffee enemas appear in medical texts going back at least to the late 1800s as a constipation remedy and as a method for sustaining liver function in chemotherapy and post-surgical recovery. The Merck Manual, the standard physician's reference, listed coffee enemas for various indications through the 12th edition (1972), after which they were quietly dropped from subsequent editions as the practice fell out of conventional favor.
Max Gerson, a German-American physician working with cancer patients in the 1940s and 1950s, incorporated coffee enemas as a structural element of his treatment protocol. Gerson's rationale (published in his 1958 book "A Cancer Therapy: Results of Fifty Cases") was that tumor lysis from his hypocaloric, plant-based dietary regimen generated a heavy hepatic toxin load, and that coffee enemas accelerated biliary excretion of those metabolites, preventing the liver from being overwhelmed.
Nicholas Gonzalez, a Cornell-trained internist working in New York, revived and modernized the Gerson protocol in the 1990s for advanced pancreatic cancer. Gonzalez's pilot trial (PubMed 10408866, Pancreas 1999) reported 4 of 11 patients with stage IV inoperable pancreatic adenocarcinoma surviving past 2 years — far exceeding the <5% expected 2-year survival at that time. The follow-up randomized controlled trial comparing the Gonzalez regimen to gemcitabine (Chase study, PubMed 19687229) was published in 2010 and is the source of substantial controversy: results favored gemcitabine, but the study was criticized by Gonzalez and others for protocol compliance issues, patient selection problems, and methodological flaws.
Proposed Biochemical Mechanism
The biochemical rationale offered by Gerson, Gonzalez, and contemporary functional medicine proponents has several documented components:
- Caffeine absorption via the rectal venous plexus. The hemorrhoidal veins drain partially into the portal vein and partially into the systemic circulation. Caffeine absorbed from the rectum can therefore reach the liver directly via portal circulation at higher concentrations than would be achieved by oral coffee. The Teekachunhatean 2013 pharmacokinetic study (PubMed 24279031) confirmed measurable rectal caffeine absorption, with serum levels lower than oral coffee but reaching the liver via portal flow.
- Caffeine and theophylline stimulation of bile flow. Caffeine and the related methylxanthines stimulate gallbladder contraction and bile flow through cholecystokinin-like effects and direct smooth-muscle action.
- Palmitic acid ester (kahweol and cafestol) upregulation of glutathione S-transferase (GST). The diterpenes in coffee oil — kahweol and cafestol, which are concentrated in unfiltered coffee and present at lower levels in filtered coffee — have been shown in animal studies (Lam 1987, PubMed 3470140 and subsequent work) to induce GST and quinone reductase, two important Phase 2 detoxification enzymes.
- Mechanical bile-duct flushing. The Gerson rationale held that retained coffee solution distending the colon stimulates duodenal/biliary contraction reflexively, ejecting bile and any toxins it contains rather than allowing reabsorption in the ileum.
- Glutathione system support. By upregulating GST and stimulating biliary excretion, coffee enemas (per the rationale) accelerate the clearance of glutathione-conjugated metabolites and reduce the cellular oxidative stress that accumulates during heavy detoxification.
Each of these mechanisms has at least some experimental support. What remains unresolved is whether the integrated clinical effect matches what proponents claim, and whether the magnitude of GST induction or bile flow stimulation is large enough to translate into meaningful clinical outcomes.
The Gerson Therapy Context
Coffee enemas in the Gerson protocol are not a stand-alone intervention. The Gerson therapy combines:
- A strict raw-food, low-sodium, high-potassium, plant-based diet with 13 fresh juices per day (carrot, apple, green leafy)
- Multiple coffee enemas per day (originally 5+, modernized programs often 1-4)
- Supplementation with potassium, pancreatic enzymes, niacin, thyroid hormone, and others
- Castor oil treatments
- Restricted total calorie intake
Many of these elements (high vegetable intake, fresh juices, low sodium / high potassium, pancreatic enzyme supplementation) have independent biological rationales. Coffee enemas are one component of a larger system, and the claim that any single Gerson element produces the outcome (without the others) is not well supported.
The Hildenbrand 1995 melanoma analysis reported five-year survival data on Gerson-treated melanoma patients that exceeded historical controls, but the analysis was non-randomized and subject to substantial selection bias.
The Gonzalez Pancreatic Cancer Trial
The Gonzalez regimen for pancreatic cancer added a more detailed enzymatic and nutritional structure to the Gerson framework: large doses of pancreatic enzyme (purportedly to target circulating tumor cells), a customized nutritional protocol per patient, coffee enemas, and supplementation. Gonzalez believed that the enzymatic mechanism was the primary anti-tumor effect and that coffee enemas were necessary to clear the metabolic debris from tumor cell lysis.
The 1999 pilot study (Gonzalez NJ & Isaacs LL, Nutr Cancer 33:117, PubMed 10408866) reported on 11 advanced pancreatic cancer patients: median survival was 17 months and 4 patients survived past 2 years, both far exceeding the <5% expected 2-year survival.
The follow-up NIH-funded randomized controlled trial (Chase JA et al., J Clin Oncol 2010, PubMed 19687229) compared the Gonzalez regimen to gemcitabine chemotherapy. Results showed shorter survival in the Gonzalez arm. Gonzalez published an extensive critique pointing to multiple violations of the original trial design (changes from prospective randomization to patient-choice enrollment, departures from the rigorous nutritional protocol, dropout patterns). The trial remains the largest formal evaluation of any Gerson-style protocol; the interpretation of its results continues to be debated.
Available Clinical Evidence (and Gaps)
The honest summary of the clinical evidence for coffee enemas:
- For cancer treatment as monotherapy: no rigorous evidence. The Chase trial of the Gonzalez regimen is the largest data point and was not supportive when interpreted at face value.
- For symptomatic relief during detoxification (headache, nausea, fatigue from toxin mobilization): abundant clinical anecdote from Gerson and Gonzalez practitioners; no controlled trial data.
- For biochemical effect (GST induction, bile flow): several animal studies (Lam 1987 series) demonstrate the mechanism; limited human pharmacokinetic data confirms caffeine absorption from rectal route.
- For traditional indication of constipation: coffee enemas are effective for stool evacuation; this is uncontroversial but is also true of warm water enemas and other interventions.
- For mold biotoxin / CIRS / chemical sensitivity: anecdotal endorsements from practitioners; no controlled trials specifically of coffee enemas in these settings.
The lack of rigorous controlled trials reflects two realities: coffee enemas have no commercial sponsor capable of funding multi-million-dollar Phase III trials, and the practice falls outside the medical mainstream where institutional research infrastructure is concentrated.
Preparation Protocol (the Standard Recipe)
The Gerson Institute's published recipe is the standard reference:
- Coffee: organic, light to medium roast, ground coffee specifically marketed as enema coffee (such as Gerson-approved, S.A. Wilson's Gold Roast, or Pure Life). Avoid decaffeinated — the caffeine is part of the mechanism.
- Water: filtered or distilled, free of chlorine and fluoride. Tap water can be used in a pinch but is not preferred.
- Ratio: 3 tablespoons (about 15-20 g) ground coffee per 1 quart (~1 liter) of water.
- Brewing: bring water to a boil, add coffee, boil 3 minutes, then reduce to a gentle simmer for 15 minutes. Cool to body temperature (~37°C / 98-100°F) before use.
- Straining: filter through fine mesh or unbleached coffee filter to remove all grounds before introducing to the enema bag.
- Volume: standard is 1 quart (~1 L) total; experienced users may use somewhat less or more.
Storage: brewed coffee can be refrigerated up to 24-48 hours and re-warmed to body temperature; preparation in single-session batches is preferred.
Administration Procedure
- Empty bowel first (regular bowel movement or warm water enema if needed).
- Lubricate the enema tip with coconut oil, food-grade petroleum jelly, or similar.
- Lie on the right side (the position aids transit to the splenic flexure and provides better hepatic exposure via the portal circulation, by Gerson convention) with knees drawn up.
- Insert the tip 2-4 inches and allow the coffee to flow in by gravity from a bag hung 12-24 inches above the body. Slow flow is more comfortable.
- Stop flow if cramping occurs; restart slowly after the cramp passes. Clamping and slow refilling can avoid most discomfort.
- Retain the coffee for 12-15 minutes. Some practitioners shift positions (right side, back, left side, 4 minutes each) during retention to expose more colon to the coffee.
- Evacuate in the toilet. Subsequent bowel movements may continue for 30-60 minutes.
Equipment: a dedicated enema bag (silicone or stainless steel preferred over PVC plastic to minimize phthalate or BPA leaching) with a soft, flexible tip. The bag should be cleaned thoroughly between uses and stored dry.
Frequency and Duration
Recommended frequency varies by source and indication:
- Gerson cancer protocol: 5 per day at the high end; modern modified programs typically 1-3 per day.
- General detoxification or supportive use: 2-3 per week.
- Acute symptom relief (headache, nausea during heavy detox): as needed, often 1 per day during the symptomatic period.
- Maintenance use: 1 per week or fewer.
Anyone using more than 1 per day should be working with a practitioner experienced in the protocol because of the cumulative electrolyte and habituation considerations. Daily long-term use carries the highest risk of electrolyte disturbance and bowel function dependence.
Cautions, Adverse Events, and Contraindications
The safety record of coffee enemas is reasonable but not unblemished. Documented adverse events:
- Electrolyte disturbances — the 1980 Eisele case series (PubMed 7416348) reported hypokalemia, hyponatremia, and dehydration in patients using frequent coffee enemas. Two deaths were reported. Risk is highest in patients on diuretics, with eating disorders, or with cardiac arrhythmia susceptibility. Use of electrolyte supplementation between sessions is prudent for regular users.
- Proctocolitis — the 2009 case report (PubMed 19918168) documented inflammatory proctocolitis attributed to coffee enema use; the mechanism may involve coffee acids or temperature-related mucosal injury. Recovery on cessation.
- Bowel perforation — rare; reported in literature for various enema procedures and not unique to coffee enemas. Risk is highest with rigid or improperly inserted tips, with pre-existing diverticular disease, with inflammatory bowel disease, and with too-vigorous administration.
- Caffeine tachycardia / palpitations — some users absorb enough caffeine to develop tachycardia, anxiety, or insomnia. Reducing volume, frequency, or coffee strength typically resolves.
- Bacterial contamination — coffee solutions left at room temperature can grow bacteria. Always use freshly brewed coffee or properly refrigerated and re-warmed coffee.
- Habituation / dependence on enema-stimulated bowel function — reported in chronic users; reversible on cessation.
Absolute or relative contraindications:
- Active inflammatory bowel disease (Crohn's, ulcerative colitis in flare)
- Severe diverticular disease
- Recent rectal or colon surgery
- Active hemorrhoids (relative; can be uncomfortable)
- Severe cardiovascular disease (caffeine and electrolyte risk)
- Severe kidney disease
- Eating disorders
- Pregnancy
- Active GI bleeding
- Caffeine sensitivity or arrhythmia history
Coffee enemas remain a contested intervention. For anyone considering use, working with a practitioner familiar with the protocol is the safer path, and starting at low frequency (once a week or less) to assess individual tolerance is prudent.
Key Research Papers
- Gonzalez NJ & Isaacs LL, Pancreatic proteolytic enzyme treatment of inoperable pancreatic adenocarcinoma (pilot) — Search PubMed
- Chase JA et al., Pancreatic proteolytic enzyme therapy vs gemcitabine for pancreatic cancer (the formal RCT) — Search PubMed
- Reed A et al., Gerson therapy for cancer (review) — Search PubMed
- Eisele JW & Reay DT, Deaths related to coffee enemas Search PubMed
- Lee CJ et al., Proctocolitis caused by coffee enema (case report) — Search PubMed
- Teekachunhatean S et al., Pharmacokinetics of caffeine by coffee enema vs oral coffee Search PubMed
- Lam LK et al., Isolation and identification of kahweol palmitate and cafestol palmitate as active anti-carcinogens in green coffee beans Search PubMed
- Cassileth BR, The Gonzalez regimen and review PubMed: Cassileth Gonzalez review
- Hildenbrand GL et al., Five-year survival data on Gerson therapy for melanoma PubMed: Hildenbrand Gerson melanoma
- Higdon JV & Frei B, Coffee and health: a review of recent human research (kahweol / cafestol section) — PubMed 16507475: Higdon coffee health review
- Cavin C et al., Cafestol and kahweol, two coffee specific diterpenes with anticarcinogenic activity — PubMed 12067578: Cavin cafestol kahweol
- Green S, Nicholas Gonzalez treatment for cancer (skeptical review) PubMed: Skeptical Gonzalez review
Connections
- Detox Protocols Benefits Hub
- Detox Protocols (Main)
- Liver Phase 1 and Phase 2
- Sweating and Sauna Therapy
- Binders: Charcoal & Chlorella
- Gerson Therapy
- Coffee
- Glutathione
- N-Acetyl Cysteine
- Pancreatic Cancer
- Oncology
- Gastroenterology
- Hepatology
- Mold (Mycotoxins)
- Heavy Metals
- Potassium
- Magnesium
- Sodium
- Coffee Enemas: Gerson Therapy Tradition — the Gerson-therapy account of the same practice set against the mainstream oncology consensus and the documented harms.
- Gerson Therapy — Coffee Enema Component — the Kellogg-era origins, the Wattenberg Phase II argument, and the published harms case in detail.