Glutathione (GSH — The Master Antioxidant)
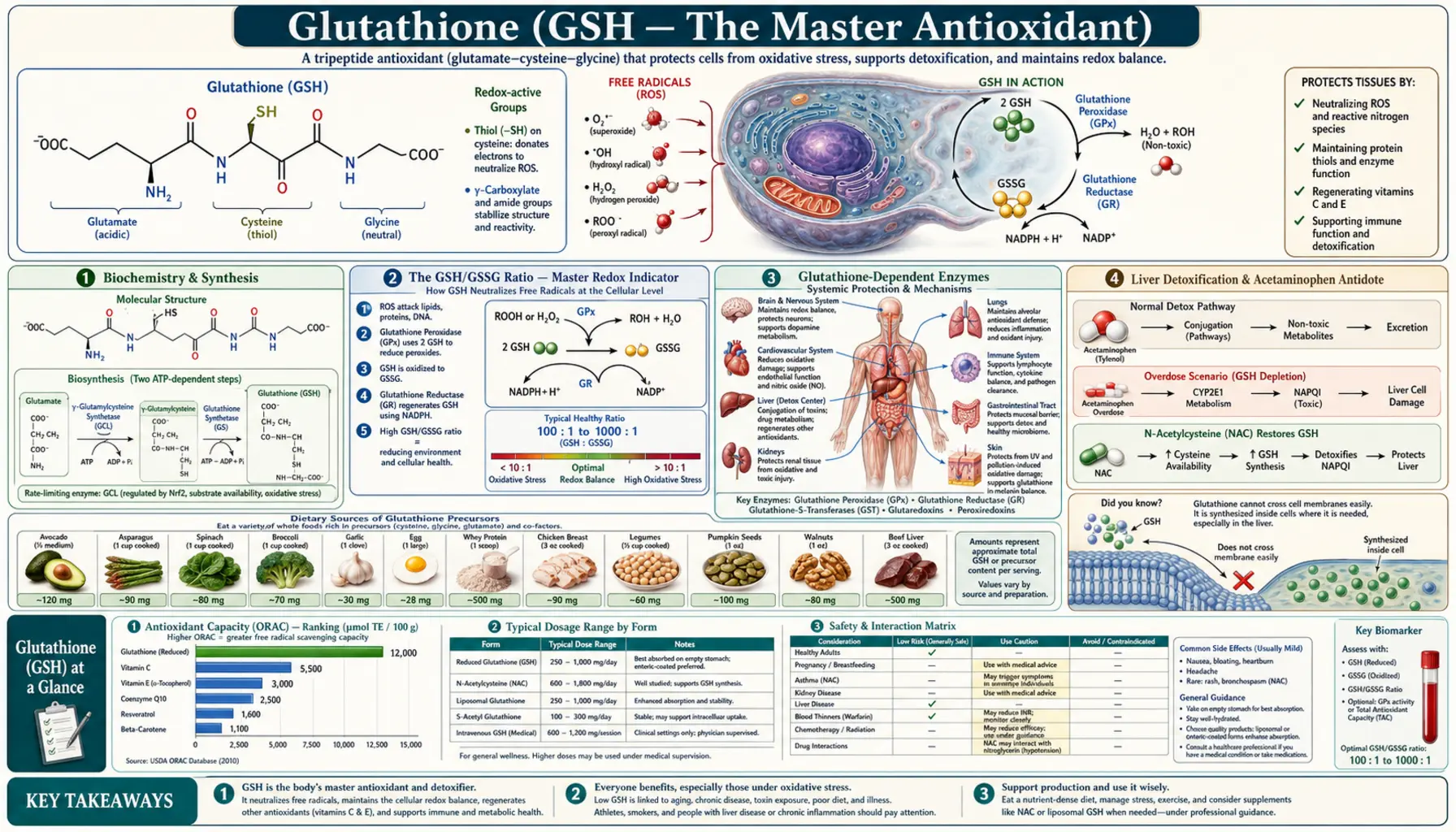
Glutathione (GSH) is a tripeptide of glutamate, cysteine, and glycine and the most abundant intracellular antioxidant in the human body, present at millimolar concentrations in every cell. It detoxifies hydrogen peroxide and lipid peroxides via the glutathione peroxidase / selenium system, conjugates drugs and environmental toxins for excretion through the glutathione-S-transferases, regenerates oxidized vitamin C and vitamin E, and serves as the principal thiol buffer that maintains cellular protein structure. Glutathione is the foundation of the body's antioxidant defense — when it falls, every other system fails.
Interactive Visualization The Methylation Cycle — hand off a methyl group Watch folate and B12 recycle homocysteine into methionine — then knock out B12 and see the folate trap slam shut. Launch → Interactive Visualization How Your Liver Actually Detoxifies Watch Phase I make a toxin *more* reactive and Phase II neutralise it — and see exactly why a juice cleanse changes nothing. Launch → Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Biochemistry & Synthesis
- The GSH/GSSG Ratio — Master Redox Indicator
- Glutathione-Dependent Enzymes
- Liver Detoxification & Acetaminophen Antidote
- Age-Related Decline & the GlyNAC Trial
- Parkinson's Disease & Neurodegeneration
- Lung Disease (Cystic Fibrosis, COPD, ARDS)
- Cardiovascular & Endothelial Function
- Immune Function & T-Cell Regulation
- Autism Spectrum & Oxidative Subtypes
- Insulin Sensitivity & Diabetes
- Skin Lightening & the FDA Warning on IV Cosmetic Use
- Forms: Oral, S-Acetyl, Liposomal, Sublingual, IV, Nebulized
- Precursor Strategies (NAC, Glycine, Whey, SAMe)
- Recommended Dosage
- Cautions and Contraindications
- Research Papers and References
- Connections
- Featured Videos
Biochemistry & Synthesis
Glutathione is a tripeptide composed of three amino acids: glutamate, cysteine, and glycine. What makes it unusual is its bond chemistry — the glutamate is attached to cysteine through its γ-carboxyl group rather than the typical α-carboxyl. This γ-glutamyl peptide bond is resistant to most peptidases, allowing intact glutathione to accumulate intracellularly at millimolar concentrations (typically 1-10 mM) without being degraded by ordinary proteolysis.
The redox-active center is the thiol group (−SH) of the cysteine residue. Two reduced glutathione molecules can donate one electron each, becoming linked through a disulfide bond to form oxidized glutathione disulfide (GSSG). The thiol is what neutralizes peroxides, conjugates with electrophilic toxins, and shuttles reducing equivalents through every compartment of the cell.
Synthesis — two ATP-dependent steps
Glutathione is synthesized de novo in the cytosol of every cell through a two-enzyme pathway:
- Glutamate-cysteine ligase (GCL, also called γ-glutamylcysteine synthetase) — joins glutamate and cysteine through the γ-bond, producing γ-glutamylcysteine. This is the rate-limiting step, and its substrate cysteine is almost always the limiting reactant in cells. GCL is feedback-inhibited by glutathione, so synthesis automatically downregulates when intracellular GSH is high.
- Glutathione synthetase (GS) — adds the glycine residue to form the complete tripeptide. Genetic deficiencies of this enzyme cause severe glutathione deficiency syndromes presenting in infancy with hemolytic anemia and neurological deterioration.
Both steps consume ATP. The cysteine availability bottleneck is why N-Acetylcysteine (NAC) is such an effective glutathione-raising strategy — NAC bypasses the gut's preferential degradation of free cysteine and delivers it intact to hepatocytes, where it is rapidly incorporated into new glutathione synthesis.
The cysteine that feeds glutathione synthesis comes from three sources: dietary sulfur amino acids (cysteine and methionine via the transsulfuration pathway), endogenous turnover of body proteins, and recycled glutathione itself (broken down for amino acid reuse). The methylation cycle — SAMe, homocysteine, B12, B6, folate, and choline — feeds into transsulfuration, which is why B-vitamin deficiencies and elevated homocysteine often parallel low glutathione status.
The GSH/GSSG Ratio — Master Redox Indicator
Intracellular glutathione exists in two pools: reduced glutathione (GSH) and oxidized glutathione disulfide (GSSG). In healthy cells the ratio is approximately 100:1 in favor of GSH — an extraordinarily reducing environment compared to the relatively oxidized extracellular space. This ratio is the single most reliable biochemical indicator of cellular redox status.
When ROS production exceeds antioxidant capacity, GSH is consumed to neutralize the radicals, forming GSSG. The cell must then either regenerate GSSG back to GSH (via the NADPH-dependent enzyme glutathione reductase) or actively export GSSG to maintain the favorable ratio. Both responses cost energy and reducing equivalents.
A falling GSH/GSSG ratio signals oxidative stress before tissue damage is clinically detectable. Functional medicine practitioners measure intracellular GSH and the GSH/GSSG ratio (typically via specialty labs like Genova or Doctor's Data) as part of comprehensive oxidative-stress panels. A reduced ratio is documented in essentially every chronic disease — cardiovascular disease, type 2 diabetes, neurodegeneration, cancer, autoimmune disease, infections, and aging itself.
The total glutathione pool also matters: a cell with severely depleted total glutathione (say, after acetaminophen overdose) is in metabolic crisis even if the small amount remaining is fully reduced. Both quantity (total GSH) and quality (GSH/GSSG ratio) are clinically relevant.
Glutathione-Dependent Enzymes
Glutathione works through four major enzyme families, each catalyzing a different reaction:
- Glutathione peroxidases (GPx) — selenium-dependent — use GSH as the electron donor to reduce hydrogen peroxide (H&sub2;O&sub2;) to water and to reduce lipid peroxides (LOOH) to their corresponding alcohols (LOH). This is how the body neutralizes the peroxides generated as a byproduct of mitochondrial respiration and immune cell respiratory burst. There are eight GPx isoforms; all but GPx4 use the selenocysteine residue at their active site, which is why selenium deficiency rapidly impairs glutathione's antioxidant function even when GSH levels are adequate.
- Glutathione reductase (GR) — the regenerator — converts GSSG back to two molecules of GSH, using NADPH as the electron source. NADPH is supplied primarily by the pentose phosphate pathway. Vitamin B2 (riboflavin) is required as the FAD cofactor for GR; severe riboflavin deficiency therefore mimics glutathione deficiency.
- Glutathione-S-transferases (GST) — Phase II detoxification — conjugate GSH onto electrophilic drugs, carcinogens, and environmental toxins, increasing their water solubility for biliary or urinary excretion. The GST family handles the bulk of toxin clearance for compounds like acetaminophen metabolites, polycyclic aromatic hydrocarbons (cigarette smoke), heterocyclic amines (charred meat), and many chemotherapy drugs. Genetic GST polymorphisms (GSTM1, GSTT1 null genotypes) affect individual detoxification capacity and partly explain variable susceptibility to chemical exposures.
- γ-Glutamyltransferase (GGT) — the recycler — cleaves the γ-glutamyl bond of extracellular glutathione, allowing constituent amino acids to be transported into cells and reused for synthesis. Elevated serum GGT is a sensitive marker of oxidative stress and the cellular response to glutathione depletion — the body upregulates GGT to scavenge every available cysteine when intracellular glutathione is low.
Beyond the enzymatic pathways, reduced glutathione directly regenerates oxidized vitamin C (dehydroascorbate) back to active ascorbate, which in turn regenerates oxidized vitamin E in membranes. Glutathione also recycles oxidized lipoic acid and oxidized CoQ10. It sits at the center of the network that alpha lipoic acid uniquely participates in.
Liver Detoxification & Acetaminophen Antidote
The liver contains the highest concentration of glutathione of any organ — roughly 5-10 mM in hepatocytes, compared to 1-2 mM in most other tissues. This reflects the liver's role as the body's primary detoxification organ, where ingested drugs and environmental toxins are biotransformed through the two-phase hepatic metabolism system:
- Phase I (cytochrome P450 enzymes) — oxidize, reduce, or hydrolyze lipophilic compounds to add reactive sites. Phase I often produces reactive intermediates that are MORE toxic than the parent compound and must be quickly neutralized.
- Phase II conjugation (including glutathione-S-transferases) — attaches glutathione, glucuronic acid, sulfate, glycine, taurine, or methyl groups to the Phase-I products, rendering them water-soluble and excretable. Glutathione conjugation handles the most chemically aggressive intermediates.
The acetaminophen antidote — NAC as glutathione precursor
Acetaminophen (paracetamol, Tylenol) is the classic example. Therapeutic doses are safely cleared through glucuronidation and sulfation, but a small fraction is oxidized by CYP2E1 to NAPQI (N-acetyl-p-benzoquinone imine), a highly reactive hepatotoxin. At normal doses, hepatic glutathione conjugates NAPQI and excretes it harmlessly. In overdose, the glucuronidation and sulfation pathways saturate, NAPQI production surges, hepatic glutathione is consumed, and the unconjugated NAPQI covalently binds liver proteins, causing centrilobular necrosis and acute liver failure.
N-acetylcysteine (NAC) is the FDA-approved antidote because it replenishes hepatic cysteine, allowing the liver to synthesize new glutathione, which then conjugates accumulated NAPQI. NAC is dosed orally (140 mg/kg loading + 70 mg/kg every 4 hours × 17 doses) or intravenously (300 mg/kg over 21 hours by the Prescott protocol). When given within 8-10 hours of overdose, NAC is nearly 100% effective at preventing hepatotoxicity — one of the most successful antidote stories in clinical toxicology.
The same mechanism explains glutathione's broader role in detoxification: it conjugates and neutralizes the reactive intermediates of mercury, lead, arsenic, cadmium, organophosphate pesticides, mold mycotoxins, and BPA. Functional medicine practitioners often pair glutathione (or its precursor NAC) with structured detox protocols for patients with documented heavy metal or environmental toxin burden.
Age-Related Decline & the GlyNAC Trial
Glutathione levels decline progressively with age. Population studies (Sekhar et al., 2011) show that intracellular GSH in red blood cells falls roughly 50% between ages 30 and 80. Older adults show simultaneously reduced GSH synthesis (lower cysteine and glycine availability), reduced GR activity (less efficient regeneration), and increased GSSG accumulation. The result is markedly compromised antioxidant capacity precisely when oxidative stress and chronic disease are accelerating.
The GlyNAC trials (Sekhar lab, Baylor College of Medicine)
Rajagopal Sekhar and colleagues at Baylor have run a series of trials testing combined glycine + NAC supplementation (a strategy they branded "GlyNAC") in older adults with documented glutathione deficiency. The 2021 trial in Clinical and Translational Medicine randomized older adults (ages 70-80) to 24 weeks of GlyNAC supplementation (glycine 100 mg/kg + NAC 100 mg/kg daily) versus placebo. Results in the GlyNAC group:
- Restoration of red blood cell GSH to youthful levels (~50% increase)
- Significant reductions in oxidative stress markers — isoprostanes, 8-OHdG, malondialdehyde
- Reduced mitochondrial dysfunction on multiple markers
- Reduced inflammation — IL-6, TNFα, hs-CRP
- Reduced insulin resistance — HOMA-IR improved
- Improved physical function — grip strength, gait speed, 6-minute walk distance
- Reduced waist circumference and improved body composition
- Improved cognitive scores on executive-function testing
The GlyNAC framework treats age-related glutathione deficiency as a clinically actionable target rather than an unavoidable consequence of aging. Similar effects have been documented in pediatric and adult HIV (Sekhar 2008), diabetes (Sekhar 2011), and nonalcoholic fatty liver disease.
For most older adults, the practical implementation is NAC 600 mg twice daily + glycine 5-10 g daily, taken with meals, for at least 12 weeks before assessing biomarkers. Targeting precursors (NAC + glycine) is more effective than supplementing glutathione itself orally because of digestive degradation.
Parkinson's Disease & Neurodegeneration
Parkinson's disease involves selective oxidative damage to dopaminergic neurons in the substantia nigra. Glutathione levels in the substantia nigra are reduced by 40-50% in Parkinson's patients at autopsy, and this depletion is detectable even in early-stage disease, suggesting it may be a causal factor rather than merely a consequence.
The pivotal Sechi trial (1996, Progress in Neuropsychopharmacology & Biological Psychiatry) gave IV glutathione 600 mg twice daily for 30 days to 9 untreated Parkinson's patients. Results showed a 42% improvement in motor and cognitive symptoms on the UPDRS, with the benefit persisting for 2-4 months after discontinuation. Despite the small uncontrolled design, this trial launched widespread off-label use of IV glutathione in integrative neurology practices.
Subsequent controlled trials have been less consistent. Hauser et al. (2009) randomized 21 Parkinson's patients to IV glutathione 1400 mg three times weekly versus placebo for 4 weeks. The glutathione group showed trends toward UPDRS improvement that did not reach statistical significance, possibly due to small sample size and short duration. A 2017 trial of intranasal glutathione (Mischley et al., Movement Disorders) showed clear motor improvement at 200 mg/day but no significant benefit over placebo.
The current state of the evidence: intravenous and intranasal glutathione likely help some Parkinson's patients but the effect size is modest, replication is inconsistent, and high-quality randomized data are limited. The biology is compelling enough that the intervention remains common in functional and integrative neurology, particularly in early-stage disease where neuronal rescue may still be possible.
For other neurodegenerative conditions — Alzheimer's, multiple sclerosis, ALS — glutathione depletion is documented but supplementation evidence is weaker. The combined approach of NAC + glycine + alpha lipoic acid + selenium offers broader mitochondrial and antioxidant support than any single intervention.
Lung Disease (Cystic Fibrosis, COPD, ARDS)
The lungs are uniquely exposed to oxidative stress — they are the only organ in continuous contact with 21% atmospheric oxygen, and they receive the entire cardiac output. Glutathione is concentrated in alveolar lining fluid at levels 100-400× higher than plasma, where it neutralizes inhaled oxidants, pollutants, and the ROS generated by alveolar macrophages.
Cystic fibrosis
CF patients have severely reduced glutathione in airway surface fluid (often less than 10% of normal) because mutant CFTR cannot transport GSH into the airway lumen. Inhaled or nebulized glutathione (300-600 mg twice daily) and oral NAC have been studied as antioxidant therapy to reduce neutrophil-mediated airway damage. A 2014 Cochrane review found modest improvements in FEV1 and reduced exacerbations with inhaled glutathione, though heterogeneity across trials limits firm conclusions.
COPD and chronic bronchitis
Oral NAC (600-1200 mg/day) has been studied for decades in chronic bronchitis and COPD as a mucolytic and antioxidant. The 2014 PANTHEON trial (Zheng et al., Lancet Respiratory Medicine) showed that NAC 600 mg twice daily for one year reduced COPD exacerbations by 22% in Chinese patients with moderate-to-severe disease. The mechanism is replenishment of bronchial epithelial glutathione, reduced neutrophil oxidative damage, and disruption of mucus disulfide bonds.
ARDS and ventilator-associated lung injury
Acute respiratory distress syndrome (ARDS) is characterized by alveolar glutathione depletion and oxidative damage to the alveolar-capillary barrier. Small ICU trials have explored IV NAC and IV glutathione as adjunctive therapy, with mixed results. The biological rationale is strong; clinical effect size in critically ill patients is variable.
Cardiovascular & Endothelial Function
Glutathione protects the vascular endothelium from oxidative damage and preserves nitric oxide bioavailability — the master regulator of vascular tone. Endothelial glutathione depletion is documented in cardiovascular disease, hypertension, and metabolic syndrome.
Small trials have shown that IV glutathione improves brachial artery flow-mediated dilation in patients with peripheral vascular disease (Prisco 2002) and reduces oxidative stress markers in stable coronary artery disease. Oral NAC reduces blood pressure modestly in trials of hypertensive patients and improves endothelial function as measured by flow-mediated dilation.
Glutathione also reduces LDL oxidation — the initiating step of atherosclerotic plaque formation. Patients with low intracellular glutathione show accelerated coronary calcification on CT scoring and higher rates of major adverse cardiovascular events on long-term follow-up.
Immune Function & T-Cell Regulation
Glutathione is essential for T-lymphocyte function. The proliferation of T-cells in response to antigen requires intracellular GSH levels above a critical threshold; cells with depleted glutathione show reduced proliferation, impaired cytokine production, and accelerated apoptosis. The Th1/Th2 balance — the switch between cell-mediated and humoral immune responses — is partly determined by intracellular GSH, with higher levels favoring Th1 (cell-mediated) responses against intracellular pathogens.
This explains the historical observation that severely glutathione-depleted patients (HIV, advanced cancer, sepsis) develop opportunistic infections and impaired vaccine responses. Sekhar's HIV trials (2008) showed that GlyNAC supplementation restored CD4 T-cell function and reduced markers of immune exhaustion in HIV patients with documented glutathione deficiency.
For ordinary immune support in healthy adults, intracellular glutathione is one of several factors that determines responsiveness; ensuring adequate cysteine, glycine, and selenium status is the foundation, with explicit glutathione supplementation reserved for documented deficiency or specific clinical indications.
Autism Spectrum & Oxidative Subtypes
A substantial fraction of children diagnosed with autism spectrum disorders show evidence of impaired methylation, low intracellular glutathione, and elevated oxidative stress markers. The Jill James group at the University of Arkansas (James et al., 2004 and subsequent) documented reduced GSH and elevated GSSG in plasma and lymphocytes of autistic children compared to neurotypical controls, with the magnitude of redox imbalance correlating with clinical severity in some subgroups.
Open-label trials of methylation support (methyl-B12 + folinic acid) and direct glutathione precursor supplementation (NAC, sometimes transdermal glutathione) have shown improvements in irritability, social withdrawal, and stereotypy in subgroups of autistic children, though randomized controlled trials are limited and effects are heterogeneous. The work of James W. Adams at Arizona State has produced the most systematic trial data; the 2018 randomized trial of comprehensive nutritional support included glutathione precursors and showed clinically meaningful improvement.
This is an area of legitimate scientific interest but also overpromised by some commercial protocols. The evidence supports a glutathione-focused intervention in autistic children with documented redox imbalance on lab testing, not as a universal intervention for all autism spectrum patients.
Insulin Sensitivity & Diabetes
Oxidative stress in skeletal muscle and adipose tissue contributes to insulin resistance. Intracellular glutathione status is inversely correlated with HOMA-IR in patients with metabolic syndrome and type 2 diabetes, and restoration of glutathione status with NAC or GlyNAC supplementation improves insulin-mediated glucose disposal in clinical trials.
The Sekhar 2011 trial in poorly controlled type 2 diabetics (mean HbA1c 9.8%) showed that 14 days of cysteine + glycine supplementation restored red cell glutathione to healthy-control levels and reduced markers of oxidative damage. Although the short trial duration prevented direct measurement of HbA1c changes, the biochemical improvements suggest a potential adjunctive role for glutathione precursors in long-term diabetes management.
For patients with insulin resistance or early type 2 diabetes, NAC 600-1200 mg/day combined with alpha lipoic acid 300-600 mg/day forms a reasonable nutraceutical addition to metformin, dietary changes, and exercise.
Skin Lightening & the FDA Warning on IV Cosmetic Use
Glutathione has become widely marketed in Asia, the Middle East, and parts of South America for skin lightening — an off-label use based on the observation that it inhibits the enzyme tyrosinase (which converts tyrosine to melanin) and shifts melanocyte production from dark eumelanin toward lighter pheomelanin. Oral, IV, and topical formulations are sold for this purpose, often at high prices.
The clinical evidence for oral glutathione as a skin lightener is modest. Small trials (Arjinpathana 2012; Weschawalit 2017) have shown measurable reductions in skin melanin index after 2-12 weeks of 500-1000 mg/day oral glutathione, with effects most visible on sun-exposed skin.
Intravenous glutathione for cosmetic skin lightening is a different matter and the subject of FDA and Philippines FDA safety warnings. There are no controlled trials supporting cosmetic IV glutathione efficacy, and the practice has been linked to serious adverse events including Stevens-Johnson syndrome, toxic epidermal necrolysis, renal dysfunction, thyroid dysfunction, and at least one reported death. The Philippines FDA, where the practice is most popular, has issued explicit warnings against IV cosmetic glutathione, and the US FDA has not approved any glutathione product for skin lightening indications. Patients should be specifically counseled against this use, which is fundamentally different from the legitimate therapeutic IV glutathione protocols used in Parkinson's disease and other neurological conditions.
Forms: Oral, S-Acetyl, Liposomal, Sublingual, IV, Nebulized
- Reduced glutathione (GSH) oral capsules/powder — the original form. Largely degraded by digestive peptidases and intestinal γ-glutamyltransferase before reaching systemic circulation. Older studies showed minimal increase in plasma glutathione after oral GSH, though more recent work (Richie 2015) found that 1000 mg/day oral GSH for 6 months did modestly raise red cell and lymphocyte glutathione — suggesting some bioavailability over chronic dosing.
- S-Acetyl glutathione — the acetyl group on the cysteine sulfur protects the molecule from digestive degradation, improving oral bioavailability by an estimated 3-5× over reduced GSH. The acetyl group is cleaved enzymatically once inside cells, releasing active glutathione. The most pharmacologically refined oral form; more expensive.
- Liposomal glutathione — phospholipid-encapsulated glutathione that bypasses gut peptidase degradation. Trials (Sinha 2018) show meaningful increases in red cell glutathione, NK cell activity, and reduced oxidative stress markers at 500-1000 mg/day for 4 weeks. Reasonably effective oral option.
- Sublingual glutathione spray/lozenge — absorbed across oral mucosa, bypassing gut degradation. Limited bioavailability data but commonly used in functional medicine practice.
- Intravenous glutathione — 600-2000 mg in saline infused over 15-30 minutes. Produces immediate elevation of plasma glutathione to supraphysiological levels for 1-2 hours. Used clinically for Parkinson's disease, acetaminophen overdose (often as IV NAC instead), and acute glutathione depletion states. Off-label use in IV nutrient therapy clinics for chronic fatigue, fibromyalgia, post-viral syndromes, heavy metal mobilization, and (controversially) cosmetic skin lightening.
- Nebulized glutathione — 100-600 mg dissolved in saline and inhaled via nebulizer. Delivers high concentrations directly to airway and alveolar lining fluid. Used in cystic fibrosis, COPD, chronic sinusitis. Requires reduced (not oxidized) glutathione and a compounding pharmacy.
- Transdermal glutathione — cream or patch applications. Bioavailability is highly variable and depends heavily on the carrier matrix. Used in pediatric autism protocols where oral compliance is difficult.
- Suppository glutathione — rectal absorption bypasses first-pass hepatic metabolism. Niche use in patients with severe gut absorption problems.
Practical guidance: For most clinical purposes, raising intracellular glutathione via precursors (NAC + glycine) is more effective per dollar than supplementing glutathione directly. Reserve direct glutathione (liposomal, S-acetyl, or IV) for documented severe deficiency, acute toxicology, neurological disease, or specific protocols where rapid plasma elevation is needed.
Precursor Strategies (NAC, Glycine, Whey, SAMe)
Because direct oral glutathione has variable bioavailability, the dominant clinical strategy is to supply the synthesis precursors and let the body manufacture its own glutathione. The major precursor strategies:
- N-Acetylcysteine (NAC) — the most studied and effective single intervention. The acetyl group protects cysteine from gut breakdown and oxidation; the freed cysteine enters hepatocytes and feeds GCL. Standard dose 600-1800 mg/day. Affordable, well-tolerated, and the foundation of any glutathione-raising protocol.
- Glycine — the second amino acid in the glutathione tripeptide; often deficient in older adults despite adequate protein intake because turnover demand exceeds dietary supply. 5-10 g/day glycine (1-2 teaspoons of pure glycine powder, which has a mildly sweet taste) is the typical GlyNAC dose.
- Cysteine-rich whey protein — undenatured (cold-processed) whey provides cysteine in the form of cystine peptides that resist gut degradation. The Immunocal product is a researched cysteine-delivery whey; generic high-quality whey concentrate (not isolate) provides similar effects. 20-40 g/day.
- SAMe (S-adenosylmethionine) — methylation donor that supports transsulfuration of methionine to cysteine. Most useful in patients with low SAMe (often correlated with low folate, B12, B6) or genetic polymorphisms in MTHFR.
- Sulforaphane (broccoli sprout extract) — Nrf2 activator that upregulates the GCL gene transcription, increasing the enzymatic capacity for glutathione synthesis rather than just providing precursors. 10-30 mg/day or fresh broccoli sprouts.
- Selenium — not a glutathione precursor but essential for glutathione peroxidase function. 100-200 mcg/day from selenomethionine or selenium yeast.
- Vitamin B2 (Riboflavin) — cofactor for glutathione reductase. Most adults get enough from diet but supplementation (100-400 mg/day) is part of mitochondrial protocols.
The integrative medicine "glutathione stack" typically combines NAC + glycine + selenium + sulforaphane — addressing precursor supply, regeneration cofactors, and transcriptional upregulation simultaneously.
Recommended Dosage
- General antioxidant / preventive (precursor strategy) — NAC 600 mg twice daily + glycine 5 g/day with meals; minimum 12 weeks before assessing biomarkers
- S-Acetyl glutathione (oral direct) — 100-300 mg/day with a meal containing some fat
- Liposomal glutathione (oral direct) — 500-1000 mg/day, can be split into two doses
- Reduced glutathione (oral direct) — 250-1000 mg/day; lower bioavailability than other forms
- IV glutathione (functional medicine / Parkinson's protocols) — 600-2000 mg in 100-250 mL saline over 15-30 minutes, 1-3 times per week, typically for 4-12 week courses
- Nebulized glutathione (CF, COPD, chronic sinusitis) — 100-600 mg in saline twice daily via nebulizer; requires compounding pharmacy preparation
- Acetaminophen overdose (NAC antidote) — 140 mg/kg loading oral or 150 mg/kg IV over 1 hour, followed by structured maintenance dosing; emergency-room protocol, not for outpatient use
- GlyNAC for healthy aging — glycine 100 mg/kg + NAC 100 mg/kg daily (typical: 6-8 g glycine + 6-8 g NAC for a 70 kg adult), divided into 2 doses, for 12-24 weeks
- Cosmetic skin lightening (oral) — 250-500 mg/day reduced or S-acetyl glutathione for 12-24 weeks; effects modest. Never recommend IV glutathione for cosmetic use.
Timing. Oral glutathione absorption is improved when taken between meals (gut peptidase activity is lower) but tolerability is better with food. S-acetyl and liposomal forms are less timing-sensitive than reduced glutathione. NAC is taken with or without food — some patients prefer with food to avoid mild stomach upset.
Cautions and Contraindications
Glutathione and its precursors have an excellent overall safety record, but several important considerations exist:
- Asthma — nebulized and oral forms — paradoxical bronchospasm has been reported with both nebulized glutathione and oral NAC in some asthmatic patients, particularly those with sulfite sensitivity. Always perform a supervised first dose in asthmatic patients.
- Pregnancy and breastfeeding — oral NAC has been used safely in pregnancy for acetaminophen overdose (a clear life-threatening indication). Routine supplementation during pregnancy lacks safety data; avoid in the absence of specific clinical indication.
- Cystinuria — the rare genetic disorder causing cystine kidney stones is a relative contraindication for high-dose cysteine or NAC supplementation; cysteine is precursor to cystine.
- IV glutathione safety — therapeutic IV glutathione (for Parkinson's, etc.) administered by trained clinicians in clinical settings has an excellent safety record. IV glutathione for cosmetic skin lightening has been associated with serious adverse events including Stevens-Johnson syndrome, toxic epidermal necrolysis, kidney dysfunction, thyroid disruption, and rare deaths. The Philippines FDA and US FDA have issued specific warnings against this practice.
- Chemotherapy interactions — theoretical concern that supplemental antioxidants might interfere with chemotherapy whose mechanism depends on oxidative damage to tumor cells. Clinical data are reassuring for most agents but the question is unresolved. Coordinate with the oncology team during active treatment.
- Sulfa allergy — glutathione is not a sulfa drug (sulfa drugs contain a sulfonamide group, not the sulfhydryl thiol of glutathione/cysteine), so true sulfa allergy is not a contraindication. Some patients with "sulfa sensitivity" do tolerate glutathione poorly, however.
- Mercury mobilization without excretion capacity — high-dose glutathione can mobilize tissue mercury into the bloodstream faster than the kidneys can excrete it, potentially redistributing mercury to the brain. Heavy metal protocols should always pair glutathione/NAC with adequate hydration, hepatic and renal support, and ideally with skilled clinical supervision.
- Halitosis and sulfur breath — some patients on high-dose NAC or glutathione notice sulfurous breath odor; reduce dose or take with food.
- Mild gastrointestinal upset — nausea, abdominal discomfort, occasional loose stools; usually resolves with divided dosing and food.
Research Papers and References
The following PubMed search links provide curated entry points into the published clinical and mechanistic literature on glutathione.
- GlyNAC for healthy aging (Sekhar Baylor program) — PubMed: GlyNAC glycine NAC glutathione aging
- Glutathione in Parkinson's disease (Sechi IV trial, Hauser, Mischley) — PubMed: glutathione Parkinson disease
- NAC for COPD (PANTHEON, BRONCUS) — PubMed: NAC COPD PANTHEON BRONCUS
- NAC for acetaminophen overdose (Prescott protocol) — PubMed: NAC acetaminophen Prescott
- Inhaled glutathione in cystic fibrosis — PubMed: glutathione inhaled cystic fibrosis
- Glutathione in autism spectrum disorders (James et al.) — PubMed: glutathione autism oxidative
- Glutathione in type 2 diabetes & insulin sensitivity — PubMed: glutathione diabetes insulin sensitivity
- Glutathione age-related decline (Sekhar 2011) — PubMed: glutathione aging decline
- Glutathione and cardiovascular / endothelial function — PubMed: glutathione endothelial cardiovascular
- Glutathione and T-cell / immune function — PubMed: glutathione T-cell immune
- Oral glutathione bioavailability (Richie 2015) — PubMed: oral glutathione bioavailability
- Liposomal glutathione clinical trials (Sinha) — PubMed: liposomal glutathione
- Glutathione skin lightening & IV cosmetic safety concerns — PubMed: glutathione skin lightening safety
- Glutathione peroxidase & selenium dependency — PubMed: glutathione peroxidase selenium
- Glutathione-S-transferases & Phase II detoxification — PubMed: glutathione S-transferase detoxification
External Authoritative Resources
- Linus Pauling Institute — Glutathione (related to Nrf2 and antioxidants)
- NCCIH — Herbs and Supplements at a Glance
- MedlinePlus — Glutathione
- PubMed — All research on glutathione
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- How Your Liver Actually Detoxifies — interactive animation
- The Methylation Cycle & Homocysteine — interactive animation
- All Antioxidants
- NAC (Primary Precursor)
- Alpha Lipoic Acid
- CoQ10
- NAD+ & NMN
- Methylene Blue
- Cysteine
- Glycine
- Glutamic Acid
- Glutamine
- Methionine
- Taurine
- Selenium
- Selenium and Cancer Prevention — selenoprotein biology, the NPC and SELECT trials, evidence across prostate/colorectal/lung cancers, and the U-shaped dose-response curve.
- Sulfur
- Zinc
- Vitamin B2 (Riboflavin)
- Vitamin B6
- Vitamin B9 (Folate)
- Vitamin B12
- Vitamin C
- Vitamin E
- Oxidative Stress
- Liver Cleansing
- Detox Protocols
- Longevity Protocols
- Milk Thistle
- Turmeric (Curcumin)
- Spirulina
- Broccoli (Sulforaphane)
- Parkinson's Disease
- Cystic Fibrosis
- COPD
- Diabetes
- Autism Spectrum
- Mercury
- Lead
- Arsenic
- GGT
- Homocysteine
- Inflammatory Markers