Liver Function Tests
Liver function tests — often just called "LFTs" or a "liver panel" — are a group of blood tests that give a snapshot of your liver's health. They're among the most commonly ordered blood tests, and a mildly "abnormal" result is extremely common and usually not a cause for panic. This guide explains what each marker on the panel actually measures, how doctors read the pattern of results rather than any single number, the most common reasons results come back high, and the genuine warning signs that need prompt attention. Reference ranges below are typical adult values in U.S. conventional units; every lab sets its own ranges, so always compare your result to the range printed on your own report.
Interactive Visualization How Your Liver Actually Detoxifies Watch Phase I make a toxin *more* reactive and Phase II neutralise it — and see exactly why a juice cleanse changes nothing. Launch → Interactive Visualization What Alcohol Actually Does Inside Your Liver Ethanol becomes acetaldehyde becomes acetate — and the NADH that piles up shuts down fat burning, stalls your blood sugar and drives uric acid up. Nothing speeds it up. Launch →
Table of Contents
- Why Liver Function Is Tested
- What the Liver Does
- The Core Tests & What They Mean
- Reading the Pattern (Not Just One Number)
- Common Causes of Abnormal Results
- When to Worry — Red Flags
- Protecting Your Liver
- References
- Connections
- Featured Videos
Why Liver Function Is Tested
Your doctor may order a liver panel for several reasons, and most of them are routine rather than alarming:
- Routine checkups. Liver tests are part of the standard Comprehensive Metabolic Panel (CMP) drawn at many annual physicals, so they're frequently checked even when you feel perfectly well.
- Symptoms that could involve the liver. Persistent fatigue, jaundice (yellowing of the skin or whites of the eyes), pain or fullness in the upper-right abdomen, nausea, dark urine, pale stools, or unexplained itching can prompt liver testing.
- Monitoring medications. Some drugs — including statins, certain antibiotics, anti-seizure medicines, methotrexate, and others — can occasionally affect the liver, so periodic testing is used to keep an eye on it.
- Monitoring alcohol use or known liver conditions. If you drink heavily, or already have a condition like fatty liver or hepatitis, repeat testing tracks whether things are stable, improving, or worsening.
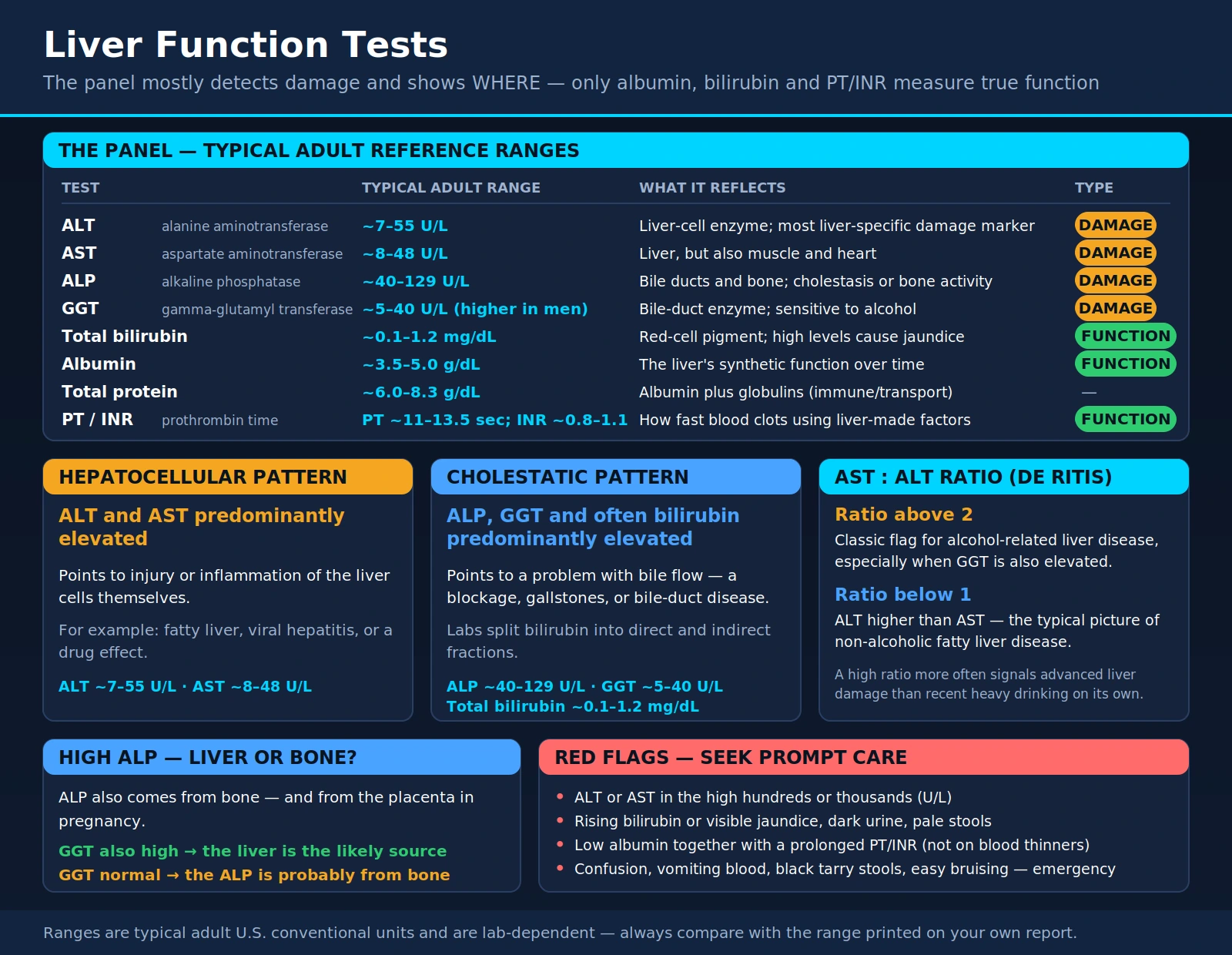
One important point about the name: "liver function tests" is something of a misnomer. Most of the markers on the panel — the enzymes ALT, AST, ALP, and GGT — actually detect liver cell damage or irritation and point to where a problem is, rather than measuring how well the liver is doing its job. Only a few values (albumin, bilirubin, and the clotting time PT/INR) genuinely reflect the liver's working function. Keeping that distinction in mind makes your results much easier to understand.
What the Liver Does
The liver is the body's largest internal organ and one of its busiest chemical factories. A few of its main jobs explain why these blood markers exist in the first place:
- Detoxification. It filters the blood and breaks down drugs, alcohol, and metabolic waste products into forms the body can safely eliminate.
- Protein production. It manufactures most of the proteins in your blood, including albumin, which keeps fluid inside your blood vessels and carries hormones and medicines.
- Bile production. It makes bile, a fluid stored in the gallbladder that helps you digest and absorb fats. Bilirubin — a yellow pigment from worn-out red blood cells — is processed and excreted through bile.
- Metabolism and storage. It helps regulate blood sugar, processes fats and cholesterol, and stores vitamins, iron, and energy as glycogen.
- Clotting factors. It produces most of the proteins your blood needs to clot, which is why a damaged liver can lead to easy bruising or bleeding (and a prolonged PT/INR).
The Core Tests & What They Mean
A standard panel includes the markers below. The ranges shown are typical adult values in U.S. conventional units, but reference ranges differ from lab to lab — and some, like GGT, vary noticeably by sex and method — so the most reliable comparison is always the range printed beside your own result.
| Test | Typical adult reference range | What it reflects |
|---|---|---|
| ALT (alanine aminotransferase) | ~7–55 U/L | An enzyme concentrated in liver cells; the most liver-specific marker of hepatocellular damage. |
| AST (aspartate aminotransferase) | ~8–48 U/L | An enzyme found in the liver but also in muscle and heart; rises with liver-cell injury (and sometimes muscle injury). |
| ALP (alkaline phosphatase) | ~40–129 U/L | An enzyme from the bile ducts and bone; elevation suggests bile-flow blockage (cholestasis) or bone activity. |
| GGT (gamma-glutamyl transferase) | ~5–40 U/L (varies widely; often higher in men) | A bile-duct enzyme; used to confirm that a high ALP is coming from the liver rather than bone, and sensitive to alcohol. |
| Total bilirubin | ~0.1–1.2 mg/dL | Yellow pigment from red-cell breakdown; high levels cause jaundice and point to bile-flow or processing problems. |
| Albumin | ~3.5–5.0 g/dL | The main blood protein the liver makes; a true marker of the liver's synthetic function over time. |
| Total protein | ~6.0–8.3 g/dL | Albumin plus globulins (immune and transport proteins); gives a broad picture of nutrition and liver/immune status. |
| PT / INR (prothrombin time) | PT ~11–13.5 sec; INR ~0.8–1.1 (if not on blood thinners) | How quickly blood clots using liver-made factors; a sensitive measure of synthetic function in serious liver disease. |
ALT and AST (the transaminases) live inside liver cells and leak into the blood when those cells are injured, so they're the headline markers of hepatocellular (liver-cell) damage. ALT is the more liver-specific of the two; AST also comes from muscle and the heart, so a high AST alone isn't always about the liver.
ALP and GGT are associated with the bile ducts. When bile flow is blocked or the ducts are irritated — a cholestatic pattern — these rise. Because ALP also comes from bone (and the placenta in pregnancy), a high ALP is often double-checked with GGT: if GGT is also up, the liver is the likely source; if GGT is normal, the ALP is probably from bone.
Total bilirubin reflects how well the liver processes and excretes the pigment from old red blood cells. When it climbs high enough, the skin and eyes turn yellow (jaundice). Labs often split it into "direct" (conjugated) and "indirect" (unconjugated) fractions to help locate the problem.
Albumin, total protein, and PT/INR are the markers that genuinely measure function. Because the liver continuously manufactures albumin and clotting factors, a low albumin or a prolonged PT/INR (not explained by blood thinners) suggests the liver's manufacturing capacity is impaired — typically in more advanced or longstanding disease rather than a brief upset.
Reading the Pattern (Not Just One Number)
The real skill in interpreting a liver panel is reading the pattern, not fixating on a single high value. Doctors generally sort abnormal results into two broad pictures:
- Hepatocellular pattern — ALT and AST are predominantly elevated. This points to injury or inflammation of the liver cells themselves (for example, fatty liver, viral hepatitis, or a drug effect).
- Cholestatic pattern — ALP, GGT, and often bilirubin are predominantly elevated. This points to a problem with bile flow, such as a blockage, gallstones, or bile-duct disease.
The AST-to-ALT ratio (sometimes called the De Ritis ratio) adds another clue:
- An AST:ALT ratio above 2 is a classic flag for alcohol-related liver disease, especially when GGT is also elevated. (Research notes that a high ratio more often signals advanced liver damage than recent heavy drinking on its own.)
- A ratio below 1 — ALT higher than AST — is the typical picture of non-alcoholic fatty liver disease and many other causes of mild liver-cell irritation.
Finally, a perspective that reassures most people: a mild, isolated elevation is usually not an emergency. Enzyme values that are slightly above the reference range — particularly a modestly raised ALT, AST, or GGT in someone who feels well — are common and frequently temporary. They can follow strenuous exercise, a recent illness, a new medication, a few drinks, or simply natural variation. Standard practice is often to recheck the test after a few weeks before pursuing extensive workups, because many mild abnormalities resolve on their own.
Common Causes of Abnormal Results
When liver numbers are up, the cause is far more often something manageable than something dire. The usual suspects include:
- Non-alcoholic fatty liver disease (NAFLD). This is the most common cause of mildly elevated liver enzymes in many countries. It's linked to excess weight, type 2 diabetes, and metabolic syndrome, and typically shows a mildly raised ALT with an AST:ALT ratio below 1. (It is increasingly called metabolic-associated steatotic liver disease, or MASLD.)
- Alcohol. Regular heavy drinking is a leading cause, classically producing a raised GGT and an AST:ALT ratio above 2.
- Medications and supplements. Many common drugs can nudge liver enzymes up. Acetaminophen (paracetamol/Tylenol) is the most important — safe at recommended doses but a leading cause of serious, dose-related liver injury when too much is taken. Statins commonly cause mild, usually harmless enzyme rises. Certain antibiotics, anti-seizure drugs, and methotrexate are also recognized culprits. Importantly, "natural" supplements and herbal products are not automatically safe — products such as high-dose green tea extract, kava, and some bodybuilding or weight-loss supplements are documented causes of liver injury.
- Viral hepatitis. Hepatitis A, B, and C can raise the transaminases, sometimes substantially. Hepatitis B and C in particular can be chronic and are screened for when liver enzymes stay elevated.
- Non-liver sources. Not every abnormal value comes from the liver. A high AST can come from muscle (after intense exercise, injury, or a muscle disorder) or the heart. A high ALP can come from bone (growing children and teens normally run high; healing fractures and some bone conditions raise it) or from the placenta during normal pregnancy. This is exactly why doctors look at the whole pattern rather than one isolated enzyme.
Less common but important causes — worth knowing exist — include autoimmune hepatitis, hereditary conditions such as hemochromatosis (iron overload) and Wilson's disease (copper overload), thyroid disorders, and celiac disease.
When to Worry — Red Flags
Most abnormal liver tests are mild and manageable, but certain patterns deserve prompt medical attention. Contact your doctor — or seek urgent care — if your results or symptoms include:
- Very high transaminases. ALT or AST in the high hundreds or the thousands (U/L) suggests significant acute liver injury — for example from an acetaminophen overdose, acute viral hepatitis, or a severe drug reaction — and needs prompt evaluation.
- Rising bilirubin or visible jaundice. Yellowing of the skin or eyes, dark "tea-colored" urine, or pale, clay-colored stools point to a meaningful problem with bile flow or liver processing.
- Signs of failing synthetic function. A low albumin together with a prolonged PT/INR (when you're not on blood thinners) suggests the liver's manufacturing capacity is impaired — a more serious sign than enzyme elevations alone.
- Symptoms needing urgent care. Confusion, drowsiness, or difficulty concentrating; vomiting blood or passing black, tarry stools; a swollen, painful abdomen; or easy bruising and bleeding can indicate advanced liver disease or acute liver failure and warrant emergency evaluation.
If you've taken more than the recommended amount of acetaminophen — even spread across several products — don't wait for symptoms; contact a poison control center or seek care immediately, because early treatment is highly effective.
Protecting Your Liver
The good news is that the liver is remarkably resilient and capable of healing, and the most common cause of abnormal tests — fatty liver — often improves substantially with lifestyle changes. Practical, evidence-aligned steps include:
- Manage weight and metabolic health. For fatty liver, gradual weight loss is the single most effective intervention; losing even a modest percentage of body weight can reduce liver fat, and larger losses can reduce inflammation. Keeping blood sugar, blood pressure, and cholesterol in good range also protects the liver.
- Moderate or avoid alcohol. Cutting back — or stopping — gives the liver a chance to recover and is one of the fastest ways to bring an elevated GGT down.
- Be cautious with medications and supplements. Stay within recommended acetaminophen doses (and watch for it hidden in combination cold and pain products), and treat herbal and "detox" supplements with healthy skepticism — tell your doctor about everything you take.
- Eat a Mediterranean-style diet. An eating pattern rich in vegetables, fruit, whole grains, legumes, fish, nuts, and olive oil — and low in sugary drinks, refined carbohydrates, and ultra-processed foods — is the dietary pattern most consistently recommended for fatty liver.
- Exercise regularly. Both aerobic activity and resistance training reduce liver fat, even without dramatic weight loss. General guidance is roughly 150 minutes of moderate activity per week.
- Stay up to date on hepatitis vaccination and screening. Vaccines protect against hepatitis A and B, and screening can detect chronic hepatitis B or C early, when treatment works best.
References
- Kwo PY, Cohen SM, Lim JK. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. American Journal of Gastroenterology. 2017;112(1):18–35. doi:10.1038/ajg.2016.517 (PMID: 27995906).
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797–1835. doi:10.1097/HEP.0000000000000323 (PMID: 36727674).
- Botros M, Sikaris KA. The De Ritis Ratio: The Test of Time. The Clinical Biochemist Reviews. 2013;34(3):117–130. PMID: 24353357.
- Nyblom H, Berggren U, Balldin J, Olsson R. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol and Alcoholism. 2004;39(4):336–339. doi:10.1093/alcalc/agh074 (PMID: 15208167).
- Lala V, Zubair M, Minter DA. Liver Function Tests. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK482489/.
- MedlinePlus (U.S. National Library of Medicine). Liver Function Tests. https://medlineplus.gov/lab-tests/liver-function-tests/.
Connections
- What Alcohol Does Inside Your Liver — interactive animation
- How Your Liver Actually Detoxifies — interactive animation
- Kidney Function
- Comprehensive Metabolic Panel
- GGT
- Non-Alcoholic Fatty Liver Disease
- Mediterranean Diet
- All Lab Tests