Chromium — Benefits Deep Dive
Chromium is the single trace mineral most directly tied to insulin signaling. Every clinical effect ascribed to chromium — glycemic control in type 2 diabetes, lipid panel improvement, modest reductions in body fat, suppression of carbohydrate cravings — flows downstream from one molecular event: the oligopeptide chromodulin (low-molecular-weight chromium-binding substance, LMWCr) loading four trivalent chromium ions and binding to the activated insulin receptor, amplifying its tyrosine kinase activity by up to eight-fold in vitro. The four benefit pages below explore the conditions where chromium produces the largest clinical effect — the glycemic axis in established type 2 diabetes, the receptor-level mechanism of insulin sensitization that underlies every other benefit, the secondary downstream effects on the lipid panel, and the weight-management literature that emerged from the 1990s chromium picolinate boom and ultimately settled into a measured place as a modest adjunct for carbohydrate-craving-driven overconsumption.
Deep-Dive Articles
Blood Sugar Regulation
The clinical translation of chromium biology — fasting glucose, HbA1c, postprandial glucose excursions, and the meta-analytic evidence in type 2 diabetes. The Anderson 1997 Beijing trial (1,000 mcg/day chromium picolinate dropping HbA1c by 1.9 percentage points), Balk's 2007 Diabetes Care meta-analysis, the chromium-free TPN deficiency case reports that established essentiality, and the emerging evidence in gestational diabetes and PCOS.
Insulin Sensitivity
The molecular mechanism that underlies every other chromium benefit. Chromodulin structure (four Cr3+ ions on a four-amino-acid peptide), the insulin-receptor tyrosine kinase amplification cycle, IRS-1/PI3K/Akt/AS160 downstream signaling, GLUT4 translocation in skeletal muscle and adipose tissue, transferrin-mediated delivery of chromium to insulin-responsive cells, and the bioavailability differences between chromium picolinate, polynicotinate, chloride, and histidinate.
Lipid Profile
How insulin sensitization produces coordinated improvement across the lipid panel. The Press 1990 UC Davis trial (the classic chromium-and-lipids citation), the mechanism through hepatic VLDL secretion and ApoB-100 suppression, LDL-receptor upregulation, lipoprotein lipase activation, and the downstream effects on triglycerides, total and LDL cholesterol, and HDL. Realistic place for chromium as adjunct to statin therapy and lifestyle modification.
Weight Management
The legitimate clinical evidence extracted from the 1990s chromium-picolinate marketing boom. Kaats's hydrostatic-weighing body-composition trials, Volpe's tightly-controlled 2001 DXA study, Davidson's 2003 atypical depression trial demonstrating carbohydrate-craving suppression, the serotonergic and noradrenergic mechanism, supplement quality and reformulation concerns, and the realistic place for chromium as a modest adjunct in carbohydrate-craving-driven overconsumption in the GLP-1-agonist era.
Table of Contents
- Deep-Dive Articles
- Why Chromium Produces Effects Across Many Systems
- Research Papers: Blood Sugar Regulation
- Research Papers: Insulin Sensitivity
- Research Papers: Lipid Profile
- Research Papers: Weight Management
- Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
Why Chromium Produces Effects Across Many Systems
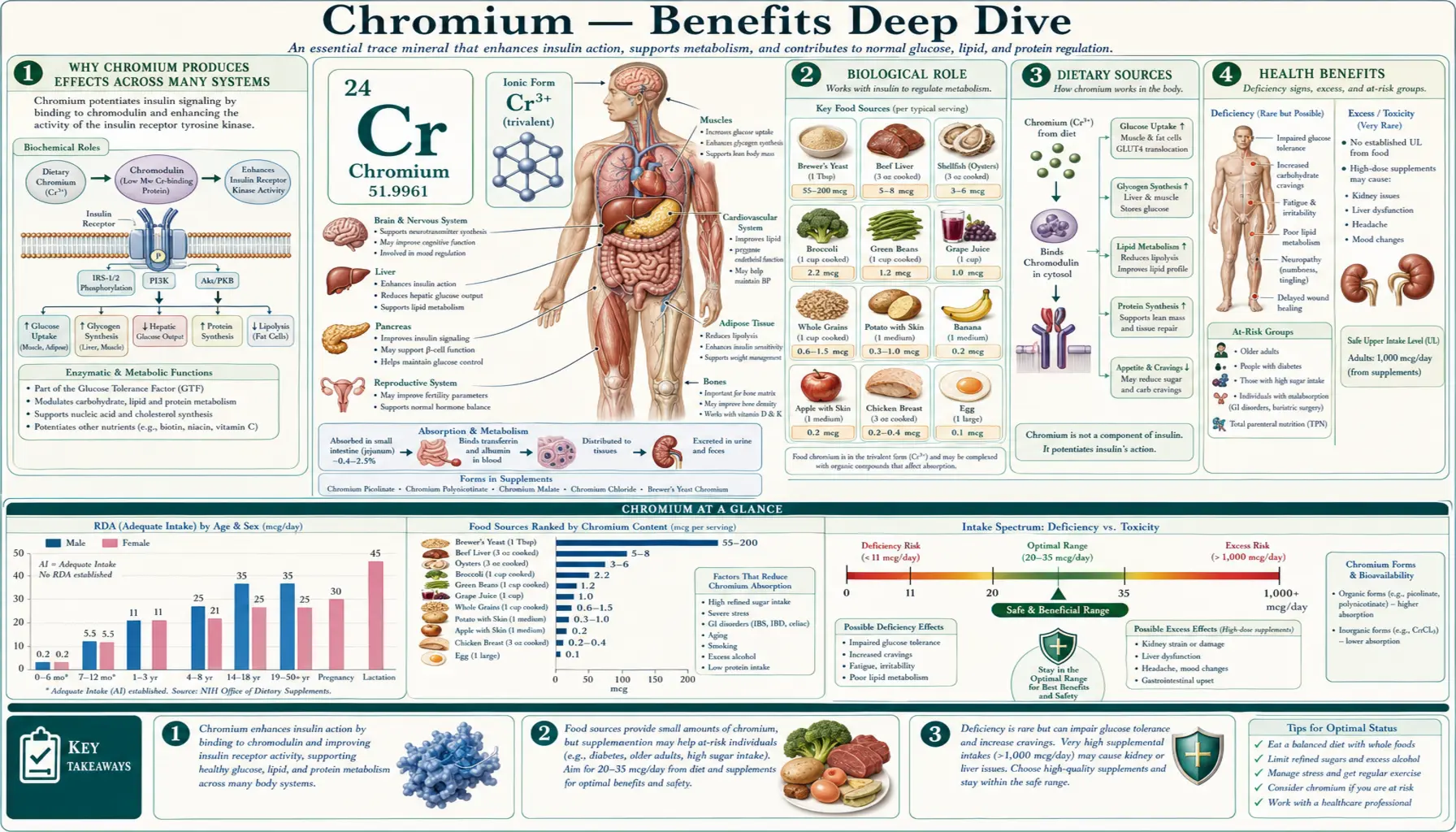
Most trace minerals participate in one principal class of enzyme reaction (zinc in metalloenzymes, iron in heme/iron-sulfur cluster electron transport, copper in oxidase reactions, selenium in selenocysteine-containing antioxidant enzymes). Chromium is unusual because it operates through one fundamentally upstream mechanism that produces clinical effects across many seemingly unrelated organ systems. The mechanism is simple to state and far-reaching in consequence: trivalent chromium loads onto the oligopeptide chromodulin (low-molecular-weight chromium-binding substance, LMWCr), holo-chromodulin binds the activated insulin receptor, and insulin signaling is amplified by up to eight-fold in vitro.
Three categories of clinical effect flow from this single upstream amplification:
- Glycemic effects — amplified insulin signaling at skeletal muscle and adipose tissue increases GLUT4 translocation to the plasma membrane and accelerates glucose disposal from the bloodstream. The downstream clinical signature is reduced fasting glucose, reduced HbA1c, and reduced postprandial glucose excursions. The strongest evidence is in patients with established type 2 diabetes with poor baseline control — this is the territory of the Blood Sugar Regulation deep-dive and the mechanism-focused Insulin Sensitivity deep-dive.
- Lipid effects — amplified insulin signaling at hepatocytes suppresses VLDL secretion (reducing circulating triglycerides), upregulates the LDL receptor (accelerating LDL clearance), and modestly suppresses HMG-CoA reductase (modestly reducing cholesterol synthesis). Amplified signaling at adipocytes suppresses inappropriate lipolysis (reducing free fatty acid flux), which secondarily reduces hepatic VLDL substrate. The downstream clinical signature is reduced triglycerides, modest LDL reduction, modest HDL elevation, and overall improvement in the atherogenic dyslipidemia of insulin resistance — the subject of the Lipid Profile deep-dive.
- Central nervous system effects — amplified insulin signaling in the brain modulates serotonergic and noradrenergic neurotransmission, with downstream effects on appetite regulation (particularly carbohydrate craving) and mood (particularly atypical depression). The downstream clinical signature is reduced carbohydrate craving, reduced caloric intake from snacking, and modest mood improvement in subjects with atypical-depression carbohydrate-craving phenotype. This is the territory of the Weight Management deep-dive and Davidson's 2003 atypical-depression trial.
The same single mechanism (chromodulin-mediated insulin-receptor amplification) thus produces three distinct categories of clinical effect because insulin itself is a master hormone with effects on glucose disposal, lipid handling, and neuroendocrine regulation. Anything that potentiates insulin signaling therefore produces a constellation of effects matching insulin's own constellation of physiological roles.
This integrative framework also explains a recurring pattern in the clinical literature: chromium's benefits are clearest in subjects with documented insulin resistance and weakest in metabolically healthy individuals. Amplifying an already-adequate insulin signal produces minimal additional benefit; amplifying a resistant signal that is failing produces measurable downstream effects across all three categories.
The therapeutic complications are correspondingly limited but real. Chromium can potentiate the glucose-lowering effect of insulin and oral antidiabetic drugs, creating hypoglycemia risk if introduced without dose adjustment. The trivalent form (Cr3+) used in supplements is nutritionally safe at standard doses; the hexavalent form (Cr6+) is an industrial toxicant and known carcinogen with no nutritional role — quality-controlled supplements ensure only trivalent chromium is present. Very-high-dose chromium picolinate (exceeding 1,200 mcg/day) has been linked to isolated case reports of renal injury; standard therapeutic doses (200–1,000 mcg/day) appear safe long-term.
Research Papers: Blood Sugar Regulation
- Anderson RA, Cheng N, Bryden NA, Polansky MM, Cheng N, Chi J, Feng J (1997). Elevated intakes of supplemental chromium improve glucose and insulin variables in individuals with type 2 diabetes (the Beijing trial). Diabetes 46(11):1786-1791. — PubMed
- Anderson RA (1998). Chromium, glucose intolerance and diabetes. Journal of the American College of Nutrition 17(6):548-555. — DOI: 10.1080/07315724.1998.10718802
- Balk EM, Tatsioni A, Lichtenstein AH, Lau J, Pittas AG (2007). Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials. Diabetes Care 30(8):2154-2163. — DOI: 10.2337/dc06-0996
- Yin RV, Phung OJ (2015). Effect of chromium supplementation on glycated hemoglobin and fasting plasma glucose in patients with diabetes mellitus. Nutrition Journal 14:14. — PubMed
- Jeejeebhoy KN, Chu RC, Marliss EB, Greenberg GR, Bruce-Robertson A (1977). Chromium deficiency, glucose intolerance, and neuropathy reversed by chromium supplementation, in a patient receiving long-term total parenteral nutrition. American Journal of Clinical Nutrition 30(4):531-538. — PubMed
- Cefalu WT, Hu FB (2004). Role of chromium in human health and in diabetes. Diabetes Care 27(11):2741-2751. — PubMed
- Suksomboon N, Poolsup N, Yuwanakorn A (2014). Systematic review and meta-analysis of the efficacy and safety of chromium supplementation in diabetes. Journal of Clinical Pharmacy and Therapeutics 39(3):292-306. — PubMed
- Heshmati J, Omani-Samani R, Vesali S, Maroufizadeh S, Rezaeinejad M, Razavi M, Sepidarkish M (2018). The effects of supplementation with chromium on insulin resistance indices in women with polycystic ovarian syndrome: a systematic review and meta-analysis of randomized clinical trials. Hormone and Metabolic Research 50(03):193-200. — PubMed
- Lamson DW, Plaza SM (2002). The safety and efficacy of high-dose chromium. Alternative Medicine Review 7(3):218-235. — PubMed
- Costello RB, Dwyer JT, Bailey RL (2016). Chromium supplements for glycemic control in type 2 diabetes: limited evidence of effectiveness. Nutrition Reviews 74(7):455-468. — PubMed
Research Papers: Insulin Sensitivity
- Vincent JB (2000). The biochemistry of chromium. Journal of Nutrition 130(4):715-718. — PubMed
- Davis CM, Vincent JB (1997). Chromium oligopeptide activates insulin receptor tyrosine kinase activity. Biochemistry 36(15):4382-4385. — PubMed
- Yamamoto A, Wada O, Suzuki H (1988). Purification and properties of biologically active chromium complex from bovine colostrum. Journal of Nutrition 118(1):39-45. — PubMed
- Mertz W (1993). Chromium in human nutrition: a review. Journal of Nutrition 123(4):626-633. — PubMed
- Vincent JB (2017). New evidence against chromium as an essential trace element. Journal of Nutrition 147(12):2212-2219. — PubMed
- Hua Y, Clark S, Ren J, Sreejayan N (2012). Molecular mechanisms of chromium in alleviating insulin resistance. Journal of Nutritional Biochemistry 23(4):313-319. — PubMed
- Anderson RA, Polansky MM, Bryden NA, Patterson KY, Veillon C, Glinsmann WH (1983). Effects of chromium supplementation on urinary Cr excretion of human subjects and correlation of Cr excretion with selected clinical parameters. Journal of Nutrition 113(2):276-281. — PubMed
- EFSA NDA Panel (2014). Scientific opinion on dietary reference values for chromium. EFSA Journal 12(10):3845. — PubMed
- Bailey CH (2014). Improved meta-analytic methods show no effect of chromium supplements on fasting glucose. Biological Trace Element Research 157(1):1-8. — PubMed
- Anderson RA (2008). Chromium and insulin resistance. Nutrition Research Reviews 16(2):267-275. — PubMed
Research Papers: Lipid Profile
- Press RI, Geller J, Evans GW (1990). The effect of chromium picolinate on serum cholesterol and apolipoprotein fractions in human subjects. Western Journal of Medicine 152(1):41-45. — PubMed
- Abraham AS, Brooks BA, Eylath U (1992). The effects of chromium supplementation on serum glucose and lipids in patients with and without non-insulin-dependent diabetes. Metabolism 41(7):768-771. — PubMed
- Riales R, Albrink MJ (1981). Effect of chromium chloride supplementation on glucose tolerance and serum lipids including high-density lipoprotein of adult men. American Journal of Clinical Nutrition 34(12):2670-2678. — PubMed
- Asbaghi O, Naeini F, Ashtary-Larky D, Moradi S, Zakeri N, Eslampour E, Kelishadi MR, Naeini AA (2021). Effects of chromium supplementation on lipid profile in patients with type 2 diabetes: a systematic review and dose-response meta-analysis of randomized controlled trials. Journal of Trace Elements in Medicine and Biology 66:126741. — PubMed
- Cheng N, Zhu X, Shi H, et al. (1999). Follow-up survey of people in China with type 2 diabetes mellitus consuming supplemental chromium. Journal of Trace Elements in Experimental Medicine 12:55-60. — PubMed
- Ngala RA, Awe MA, Nsiah P (2018). The effects of plasma chromium on lipid profile, glucose metabolism and cardiovascular risk in type 2 diabetes mellitus. PLoS ONE 13(7):e0197977. — PubMed
- Ginsberg HN, Zhang YL, Hernandez-Ono A (2005). Regulation of plasma triglycerides in insulin resistance and diabetes. Archives of Medical Research 36(3):232-240. — PubMed
- Lai MH (2008). Antioxidant effects and insulin resistance improvement of chromium combined with vitamin C and E supplementation for type 2 diabetes mellitus. Journal of Clinical Biochemistry and Nutrition 43(3):191-198. — PubMed
- Wang ZQ, Cefalu WT (2010). Current concepts about chromium supplementation in type 2 diabetes and insulin resistance. Current Diabetes Reports 10(2):145-151. — PubMed
- Vrtovec M, Vrtovec B, Briski A, Kocijancic A, Anderson RA, Radovancevic B (2005). Chromium supplementation shortens QTc interval duration in patients with type 2 diabetes mellitus. American Heart Journal 149(4):632-636. — PubMed
Research Papers: Weight Management
- Kaats GR, Blum K, Fisher JA, Adelman JA (1996). Effects of chromium picolinate supplementation on body composition: a randomized, double-masked, placebo-controlled study. Current Therapeutic Research 57(10):747-756. — PubMed
- Kaats GR, Blum K, Pullin D, Keith SC, Wood R (1998). A randomized, double-masked, placebo-controlled study of the effects of chromium picolinate supplementation on body composition: a replication and extension of a previous study. Current Therapeutic Research 59(6):379-388. — PubMed
- Volpe SL, Huang HW, Larpadisorn K, Lesser II (2001). Effect of chromium supplementation and exercise on body composition, resting metabolic rate and selected biochemical parameters in moderately obese women following an exercise program. Journal of the American College of Nutrition 20(4):293-306. — PubMed
- Davidson JR, Abraham K, Connor KM, McLeod MN (2003). Effectiveness of chromium in atypical depression: a placebo-controlled trial. Biological Psychiatry 53(3):261-264. — PubMed
- Docherty JP, Sack DA, Roffman M, Finch M, Komorowski JR (2005). A double-blind, placebo-controlled, exploratory trial of chromium picolinate in atypical depression: effect on carbohydrate craving. Journal of Psychiatric Practice 11(5):302-314. — PubMed
- Onakpoya I, Posadzki P, Ernst E (2013). Chromium supplementation in overweight and obesity: a systematic review and meta-analysis of randomized clinical trials. Obesity Reviews 14(6):496-507. — PubMed
- Tian H, Guo X, Wang X, He L, Lv R, Yang K (2013). Chromium picolinate supplementation for overweight or obese adults. Cochrane Database of Systematic Reviews (11):CD010063. — PubMed
- Anton SD, Morrison CD, Cefalu WT, Martin CK, Coulon S, Geiselman P, Han H, White CL, Williamson DA (2008). Effects of chromium picolinate on food intake and satiety. Diabetes Technology and Therapeutics 10(5):405-412. — PubMed
- Lukaski HC, Bolonchuk WW, Siders WA, Milne DB (1996). Chromium supplementation and resistance training: effects on body composition, strength, and trace element status of men. American Journal of Clinical Nutrition 63(6):954-965. — PubMed
- Wani S, Weskamp C, Marple J, Spry L (2006). Acute tubular necrosis associated with chromium picolinate-containing dietary supplement. Annals of Pharmacotherapy 40(3):563-566. — PubMed
Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- Anderson RA, Polansky MM, Bryden NA, Bhathena SJ, Canary JJ (1987). Effects of supplemental chromium on patients with symptoms of reactive hypoglycemia. Metabolism 36(4):351-355. — PubMed
- Stearns DM, Wise JP Sr, Patierno SR, Wetterhahn KE (1995). Chromium(III) picolinate produces chromosome damage in Chinese hamster ovary cells. FASEB Journal 9(15):1643-1648. — PubMed
- NIH Office of Dietary Supplements (2024). Chromium fact sheet for health professionals. — NIH ODS Chromium
- Anderson RA, Bryden NA, Polansky MM (1992). Dietary chromium intake. Freely chosen diets, institutional diets, and individual foods. Biological Trace Element Research 32:117-121. — PubMed
- Krejpcio Z (2001). Essentiality of chromium for human nutrition and health. Polish Journal of Environmental Studies 10(6):399-404. — PubMed
- Krol E, Krejpcio Z (2010). Chromium(III) propionate complex supplementation improves carbohydrate metabolism in insulin-resistance rat model. Food and Chemical Toxicology 48(10):2791-2796. — PubMed
- Komorowski JR, Greenberg D, Juturu V (2008). Chromium picolinate does not produce chromosome damage. Toxicology in Vitro 22(3):819-826. — PubMed
- Hummel M, Standl E, Schnell O (2007). Chromium in metabolic and cardiovascular disease. Hormone and Metabolic Research 39(10):743-751. — PubMed
- Pittler MH, Stevinson C, Ernst E (2003). Chromium picolinate for reducing body weight: meta-analysis of randomized trials. International Journal of Obesity 27(4):522-529. — PubMed
- Vincent JB (2019). Effects of chromium supplementation on body composition, human and animal health, and insulin and glucose metabolism. Current Opinion in Clinical Nutrition and Metabolic Care 22(6):483-489. — PubMed
External Authoritative Resources
- NIH Office of Dietary Supplements — Chromium Fact Sheet (Health Professionals) — the single most up-to-date authoritative summary of chromium evidence in the United States
- Linus Pauling Institute — Chromium Micronutrient Information Center — comprehensive scientific summary maintained at Oregon State
- EFSA — Scientific Opinion on Dietary Reference Values for Chromium (2014) — the controversial European position questioning chromium's essentiality, worth reading in dialogue with the NIH and LPI summaries
- MedlinePlus — Chromium
- PubMed — All chromium picolinate human clinical trials
Connections
- Chromium (Main Page)
- Chromium for Blood Sugar Regulation
- Chromium for Insulin Sensitivity
- Chromium for Lipid Profile
- Chromium for Weight Management
- All Minerals
- Magnesium
- Zinc
- Manganese
- Iron (Transferrin Sharing)
- Insulin Resistance
- Type 2 Diabetes
- Metabolic Syndrome
- PCOS
- Obesity
- Gestational Diabetes
- Cardiovascular Disease
- Berberine
- Blood Sugar
- Fasting
- Cinnamon
- Vitamin B3 / Niacin
- Hemoglobin A1C
- Fasting Insulin