Chromium Deficiency: What the Evidence Shows
Here is the honest bottom line, stated up front: for ordinary people eating ordinary food, a true chromium deficiency is not a recognized clinical problem. There is no validated blood test for it, no agreed-upon threshold below which you are "deficient," and no defined daily requirement — only a rough estimate of what people typically eat. The idea that low chromium causes everyday tiredness, sugar cravings, or weight gain comes mostly from supplement marketing, not from solid human evidence. The story is genuinely debated by scientists: chromium spent decades being taught as an essential trace element, but careful re-examination of the original studies has led some leading researchers to argue it may not be essential at all, and the European Food Safety Authority has declined to set a requirement. What is well documented is far narrower — a handful of severely ill patients fed entirely through a vein, decades ago, who developed glucose problems that improved when chromium was added back. This page lays out what the evidence actually supports, why a deficiency is so rarely seen in real people, who the genuine edge cases are, and what (if anything) is worth doing — without inventing symptoms that the science does not back up.
Table of Contents
- What the Evidence Actually Says
- Is Chromium Even Essential? The Live Debate
- The Biology: Why Deficiency Is Rarely Seen
- Who, If Anyone, Is Actually at Risk
- Supplements, Blood Sugar, and Weight: What the Trials Show
- What to Do (and Not Do)
- Related Nutrients and Topics
- Key Research Papers
- Connections
- Featured Videos
What the Evidence Actually Says
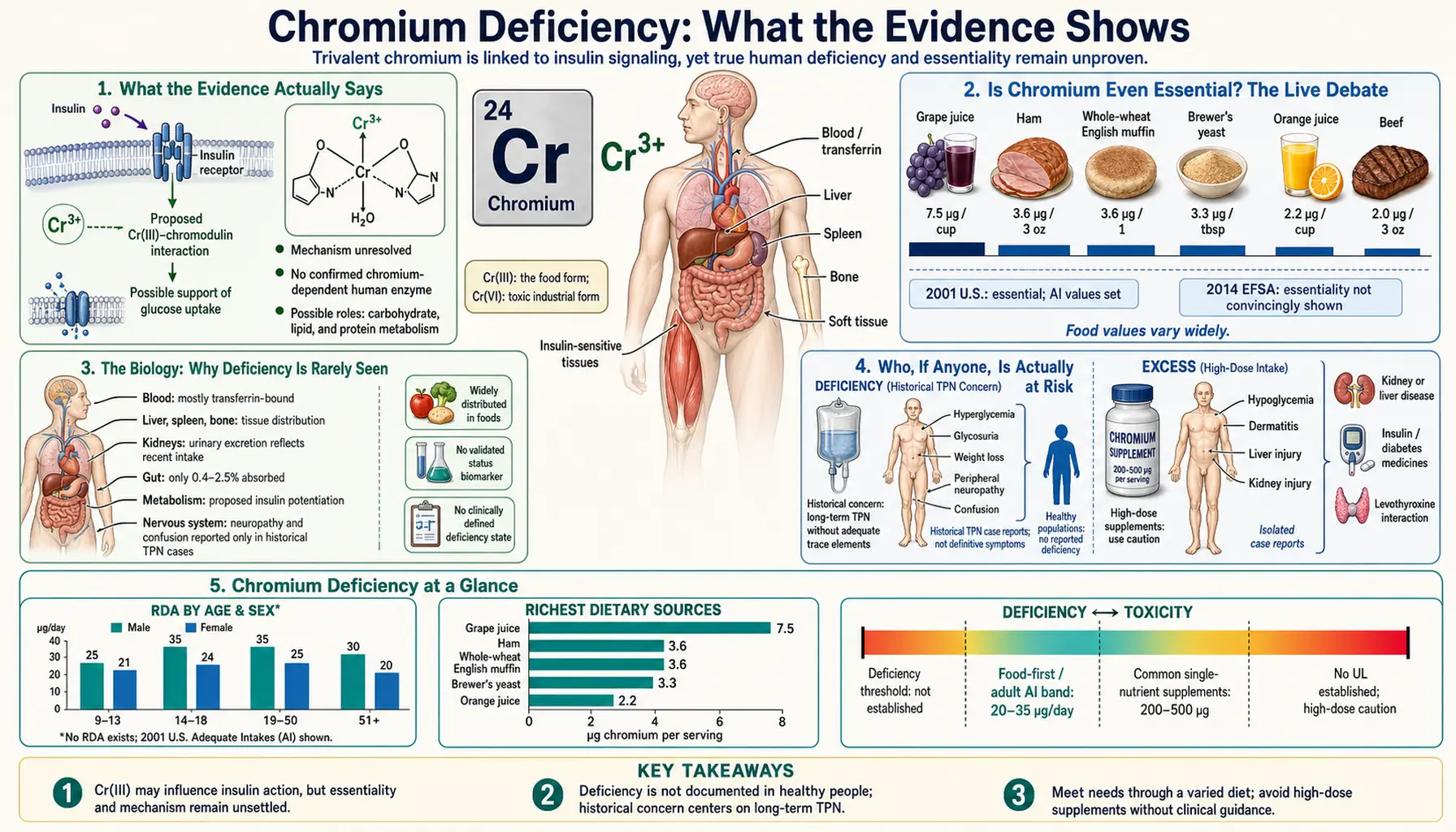
Chromium is a metal that exists in several forms. The kind found in food and supplements is trivalent chromium (chromium-3, written Cr3+ or Cr(III)) — a completely different substance from the toxic hexavalent chromium (chromium-6) used in industry, which is a known carcinogen and is covered on the Chromium Toxicity page. When people talk about dietary "chromium deficiency," they mean a shortage of the harmless food form. So does such a deficiency exist in everyday life? The careful answer is: essentially no.
Several facts make this clear, and it is worth being candid about each one:
- There is no reliable test for chromium status. Blood, serum, and hair chromium measurements are notoriously unreliable, are easily contaminated by the steel needles and equipment used to collect them, and do not correlate with how much chromium is in the body or whether a person is "low." Major reviews state plainly that no biomarker has been validated to diagnose chromium deficiency. If you cannot measure it, you cannot meaningfully diagnose a shortage of it.
- No daily requirement has ever been set. In the United States, the Institute of Medicine did not establish a Recommended Dietary Allowance (RDA) for chromium — the gold standard for a nutrient with a known requirement. Instead it set only an Adequate Intake (AI) of about 25–35 micrograms a day, and that figure was simply an estimate of what healthy people happened to be eating, not a level proven to be needed. An AI is what scientists set when they do not have enough evidence to define a real requirement.
- Europe went further. In 2014 the European Food Safety Authority (EFSA) reviewed the evidence and concluded there was no basis to set any dietary reference value for chromium, because no clear requirement in healthy people could be demonstrated.
- No naturally occurring deficiency syndrome has been described. Unlike iron, iodine, or zinc — each of which causes a well-defined illness when truly lacking — there is no recognized disease that results from eating a normal diet low in chromium. The few human cases ever reported (discussed below) occurred only under extreme, artificial conditions.
This is an unusual situation for something long called an "essential trace element," and it is exactly why the topic is debated rather than settled. The rest of this page explains how chromium earned its essential reputation, why that reputation is now contested, and what the practical takeaway is for an ordinary person.
Is Chromium Even Essential? The Live Debate
For most of the late twentieth century, textbooks listed chromium as an essential trace mineral. That belief rested on two pillars: animal experiments from the 1950s suggesting a "glucose tolerance factor" containing chromium, and a small number of human case reports. The most influential human case, published by Jeejeebhoy and colleagues in 1977, described a woman kept alive for years entirely on intravenous nutrition (total parenteral nutrition, or TPN) that contained almost no chromium. She developed glucose intolerance, weight loss, and nerve symptoms that reversed when chromium was added to her feed. Cases like this were taken as proof that humans need chromium.
Here is where honesty matters. Over the following decades, the foundation began to crack:
- The famous "glucose tolerance factor" was never isolated as a real molecule. Despite decades of searching, no defined chromium-containing compound matching the original description was ever purified and confirmed. The biologically active substance once proposed has largely failed to hold up.
- The TPN cases are hard to interpret. Critically ill patients on long-term intravenous feeding are missing or imbalanced in many nutrients at once and are profoundly abnormal metabolically. Attributing their glucose problems specifically to chromium — rather than to their underlying illness or to other deficiencies — is far from certain. Modern intravenous nutrition solutions also contain trace chromium as a contaminant regardless, so true depletion is unusual.
- No animal can be made deficient with diet alone. A defining test of essentiality is whether removing a nutrient from the diet produces a reproducible deficiency disease. Researchers have struggled to create a clear chromium-deficiency state in animals using diet, which is a serious problem for the "essential" label.
By 2010, the chemist John Vincent — one of the leading researchers on chromium biochemistry — was openly asking, in a paper titled "Chromium: celebrating 50 years as an essential element?", whether the designation was justified. In 2017 he went further, publishing "New Evidence against Chromium as an Essential Trace Element," arguing that chromium should be reclassified as a pharmacologically active substance (one that can have effects at high doses, like a drug) rather than a nutrient the body genuinely requires. This is not a fringe view; it reflects a real shift in the scientific literature.
The fairest summary today is this: chromium may have a minor biological role, but the evidence that humans require it from the diet — and that a dietary shortage causes disease — is weak and disputed. A page that told you "chromium deficiency is a common cause of fatigue and cravings" would be misrepresenting the science. The truth is more modest and more interesting.
The Biology: Why Deficiency Is Rarely Seen
If chromium does anything useful in the body, the leading idea involves a small molecule once nicknamed chromodulin (more cautiously called the low-molecular-weight chromium-binding substance, or LMWCr). The proposed picture is that chromium binds to this molecule, which may then help fine-tune the insulin signal — the hormonal message that tells cells to take sugar out of the blood. Think of insulin as someone pressing an elevator button, and chromium as a small tweak that might make the button slightly more responsive. Even researchers who study this molecule, however, describe its role as modest and still incompletely understood; recent work continues to debate exactly what it binds and does.
Now consider why an ordinary person almost never runs short, even if this molecule matters:
- The amounts involved are tiny. The estimated adequate intake is measured in micrograms — millionths of a gram. A whole day's worth would be invisible on a spoon. The body needs (at most) only a trace.
- Chromium is widespread in ordinary food. It turns up in small amounts across a normal diet — whole grains, broccoli and other vegetables, beans, nuts, some fruits, meat, and even the chromium that leaches from stainless-steel cookware. Because it is scattered so widely, eating varied, real food supplies the trace amounts in play without any effort.
- The body adapts to low intakes. When intake drops, the body absorbs a larger fraction of what is eaten and excretes less — the same conservation trick the body uses for other trace elements. This buffering makes a genuine shortage very hard to reach through diet.
Put these together and you can see why a deficiency disease essentially does not appear in free-living people: the requirement is minuscule (if it exists at all), the supply is everywhere, and the body holds on to it when intake falls. It takes truly artificial circumstances — covered next — to deplete someone.
Who, If Anyone, Is Actually at Risk
Being candid does not mean pretending the topic is irrelevant to everyone. There is a short list of genuine edge cases — but notice that none of them describes a typical person eating typical food, and all of them are managed by clinicians, not by buying a supplement off a shelf.
- Long-term total parenteral nutrition (TPN). The clearest historical cases occurred in people fed entirely and indefinitely through a vein, bypassing the digestive tract, with intravenous solutions that lacked added chromium. This is the population the original deficiency reports came from. Because of those reports, modern TPN formulas typically include trace chromium (or contain enough as a contaminant), so even this scenario is now largely a managed, monitored situation rather than a spontaneous illness.
- Severe, prolonged malnutrition or starvation. In states of extreme undernutrition, total-body trace minerals can fall along with everything else. Even here, chromium is not singled out as the driver of symptoms — it is one small item amid a much larger nutritional collapse that is treated as a whole.
- Theoretical metabolic stress states. Older literature speculated that severe physical stress, major trauma, or poorly controlled diabetes might increase chromium losses in urine. This remains speculative and has not translated into a recognized deficiency disease or a treatment that helps.
Crucially, there is no credible evidence that healthy adults, older people, vegetarians, athletes, or people who feel tired and crave sugar are "chromium deficient." Those everyday symptoms have far more common and far better-established explanations — among them poor sleep, stress, low iron (see Iron), thyroid problems, blood-sugar swings from diet, and ordinary insulin resistance — none of which are fixed by chromium.
Supplements, Blood Sugar, and Weight: What the Trials Show
Because chromium is marketed heavily for blood sugar, weight loss, and "sugar cravings," it is worth addressing those claims directly — especially since they are often dressed up as "correcting a deficiency." They are not. They are claims that extra chromium acts like a mild drug, and they have been tested.
Type 2 diabetes and blood sugar. Chromium supplements (commonly chromium picolinate) have been studied repeatedly in people with and without diabetes. The most rigorous summary is a 2007 systematic review and meta-analysis by Balk and colleagues in Diabetes Care, which pooled dozens of randomized trials. Its conclusion was sobering: chromium showed no significant effect on glucose or insulin in people without diabetes, and only inconsistent, generally small effects in people with diabetes — with the few positive signals coming largely from lower-quality studies, some conducted in populations whose diets may have differed. An earlier review by Cefalu and Hu reached a similarly cautious verdict: the data did not support routine chromium supplementation for blood-sugar control. Professional diabetes guidelines do not recommend chromium for managing diabetes.
Weight loss and "sugar cravings." The popular belief that chromium melts fat or curbs cravings is not supported. Randomized trials, including work published in Diabetes Care on chromium picolinate, have found minimal or no meaningful effect on body weight or body composition. Any benefit seen has been too small to matter in real life. The "curbs cravings" claim in particular rests on very thin evidence and is largely a marketing message.
So why do supplements still imply a deficiency? Because "you might be low in an essential mineral" is a far easier sell than "this acts like a weak, unproven drug." The honest reading of the trial evidence is that chromium supplements are, at best, marginal and inconsistent — and that taking them does not correct a deficiency, because for almost everyone there is no deficiency to correct.
What to Do (and Not Do)
The practical advice here is refreshingly low-key, precisely because this is not a real clinical problem for most people. There is no test to chase, no number to fix, and no urgency.
- Do eat a varied, whole-food diet. This is the entire strategy, and it is the same advice that supports general health. Whole grains, vegetables (broccoli is often cited), beans and lentils, nuts, and fruit all supply the trace chromium in play — alongside far more important nutrients. You do not need to count chromium or seek out "chromium-rich" foods; eating real food handles it automatically.
- Don't buy chromium supplements to treat fatigue, cravings, or weight. The evidence does not support these uses, and the premise — that you are deficient — is almost certainly false. Save your money.
- Don't chase blood, serum, or hair "chromium level" tests. They are unreliable and uninterpretable for nutritional status, and a result — high or low — will not meaningfully tell you anything actionable.
- Do look elsewhere for real answers if you feel unwell. Persistent fatigue, frequent sugar cravings, unexplained weight change, or thirst deserve a proper evaluation. The far more likely culprits — iron status, thyroid function, sleep, mood, and especially blood-sugar regulation — are testable and treatable. If blood sugar is the concern, see Diabetes, Insulin Resistance, and Metabolic Syndrome; a Comprehensive Metabolic Panel and a glucose or A1c check are the appropriate first steps.
- If you do take a modest chromium dose, it is generally low-risk — but pointless. Ordinary supplemental doses of trivalent chromium have a good safety record (toxicity is essentially an industrial-exposure problem; see Chromium Toxicity). The issue is not danger; it is that you are unlikely to be getting anything for your money.
This is one of those cases where the most accurate health advice is also the simplest: eat well, and spend your attention on the things that are actually proven to matter.
Related Nutrients and Topics
It helps to place chromium next to its neighbors, both to understand the debate and to see where your attention is better spent.
- The chromium overview — for the proposed benefits, supplement forms, and the broader case that is sometimes made for chromium, see the main Chromium page. This deficiency page is the candid counterweight: it explains why a shortage is rarely a real concern.
- Chromium toxicity — the genuinely important chromium health issue is not too little but the wrong form: industrial hexavalent chromium (chromium-6) is toxic and carcinogenic. See Chromium Toxicity.
- Trace minerals with real requirements — for contrast, Iron and Zinc are trace elements where deficiency is well defined, testable, and clinically important — the opposite of chromium's situation.
- Industrial and environmental metals — for how toxic metal forms are handled on the site, see Toxic Minerals and Heavy Metals.
- Blood-sugar topics — because most chromium claims orbit blood sugar, the better-evidenced places to focus are Insulin Resistance, Diabetes, and Metabolic Syndrome.
Key Research Papers
- Jeejeebhoy KN, Chu RC, Marliss EB, Greenberg GR, Bruce-Robertson A (1977). Chromium deficiency, glucose intolerance, and neuropathy reversed by chromium supplementation, in a patient receiving long-term total parenteral nutrition. The American Journal of Clinical Nutrition;30(4):531-538. — DOI: 10.1093/ajcn/30.4.531
- Mertz W (1988). Is Chromium Essential for Humans? Nutrition Reviews;46(1):17-20. — DOI: 10.1111/j.1753-4887.1988.tb05348.x
- Cefalu WT, Hu FB (2004). Role of Chromium in Human Health and in Diabetes. Diabetes Care;27(11):2741-2751. — DOI: 10.2337/diacare.27.11.2741
- Balk EM, Tatsioni A, Lichtenstein AH, Lau J, Pittas AG (2007). Effect of Chromium Supplementation on Glucose Metabolism and Lipids: A Systematic Review of Randomized Controlled Trials. Diabetes Care;30(8):2154-2163. — DOI: 10.2337/dc06-0996
- Vincent JB (2010). Chromium: celebrating 50 years as an essential element? Dalton Transactions;39(16):3787-3794. — DOI: 10.1039/b920480f
- Vincent JB (2017). New Evidence against Chromium as an Essential Trace Element. The Journal of Nutrition;147(12):2212-2219. — DOI: 10.3945/jn.117.255901
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA) (2014). Scientific Opinion on Dietary Reference Values for chromium. EFSA Journal;12(10):3845. — DOI: 10.2903/j.efsa.2014.3845
- Institute of Medicine (2001). Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academies Press, Washington, DC. — DOI: 10.17226/10026
- Edwards KC, Gannon MW, Frantom PA, Vincent JB (2021). Low-molecular-weight chromium-binding substance (LMWCr) may bind and carry Cr(III) from the endosome. Journal of Inorganic Biochemistry;223:111555. — DOI: 10.1016/j.jinorgbio.2021.111555
- Martin J, Wang ZQ, Zhang XH, Wachtel D, Volaufova J, Matthews DE, Cefalu WT (2006). Chromium Picolinate Supplementation Attenuates Body Weight Gain and Increases Insulin Sensitivity in Subjects With Type 2 Diabetes. Diabetes Care;29(8):1826-1832. — DOI: 10.2337/dc06-0254
PubMed Topic Searches
- PubMed — Is chromium an essential trace element?
- PubMed — Chromium deficiency and parenteral nutrition
- PubMed — Chromium supplementation, glucose, and diabetes (meta-analyses)
- PubMed — Chromium picolinate and weight loss (randomized trials)
- PubMed — Chromodulin / low-molecular-weight chromium-binding substance
Connections
- Chromium Overview
- Chromium Toxicity
- Chromium Benefits Hub
- Chromium and Blood Sugar
- Chromium and Insulin Sensitivity
- Chromium and Weight Management
- Iron
- Zinc
- Toxic Minerals
- Heavy Metals
- Diabetes
- Insulin Resistance
- Metabolic Syndrome
- Comprehensive Metabolic Panel
- Lentils