Chromium for Weight Management
Chromium picolinate was one of the most heavily marketed weight-loss supplements of the 1990s and early 2000s, generating hundreds of millions of dollars in annual U.S. sales on the back of claims that ranged from defensible to outright fraudulent. The peer-reviewed clinical evidence, when extracted from the marketing noise, tells a more measured story: chromium picolinate produces modest, statistically significant fat-mass reductions in some but not all trials, with the largest and most reproducible effect being suppression of carbohydrate cravings rather than direct fat oxidation. Kaats's two well-conducted trials in the late 1990s, Volpe's tightly controlled 2001 RCT, and Davidson's pivotal 2003 atypical depression trial together form the legitimate evidence base. This deep-dive separates that signal from the marketing noise, examines the carbohydrate-craving mechanism (serotonergic and noradrenergic effects downstream of improved insulin signaling in the brain), discusses supplement quality and reformulation issues, and provides realistic expectations for patients considering chromium as part of a weight-management strategy.
Table of Contents
- Marketing Claims vs Clinical Evidence
- The Kaats Body Composition Trials
- The Volpe 2001 Controlled Trial
- Carbohydrate Cravings and Appetite Regulation
- The Davidson Atypical Depression Trial
- Serotonergic and Noradrenergic Mechanism
- Fat Mass vs Lean Mass Composition
- Exercise Synergy and Resistance Training
- Supplement Quality and Reformulation Cautions
- Realistic Expectations and Clinical Place
- Key Research Papers
- Connections
- Featured Videos
Marketing Claims vs Clinical Evidence
Chromium picolinate emerged as a mass-market weight-loss supplement in the 1990s following the USDA Beltsville Anderson studies on chromium and insulin sensitization. The connection from "improves insulin signaling" to "burns fat" was made aggressively by supplement manufacturers, often beyond what the clinical evidence supported. The Federal Trade Commission filed multiple consent orders against major chromium picolinate marketers in 1996 and 1997, requiring them to retract claims about fat loss, muscle gain, and reduction of cardiovascular risk that the FTC deemed unsupported.
The 1997 FTC consent order against AMBI Inc. (then the largest chromium picolinate marketer) is instructive. AMBI had claimed in widely-distributed advertising that chromium picolinate "burns body fat," "increases lean muscle mass," "lowers cholesterol," and "reduces sugar cravings." The FTC ruled that the first three claims required additional substantiation beyond the published evidence; only the last (sugar craving reduction) was supported by published clinical work to the satisfaction of the FTC reviewers. AMBI was required to disclose this in subsequent advertising.
This regulatory history is worth knowing because it illustrates an important asymmetry: the public perception of chromium picolinate as a "fat burner" is partly an artifact of pre-2000 marketing rather than a fair summary of the clinical literature. A measured reading of the evidence shows that chromium picolinate's strongest reproducible effect on body composition is mediated through reduced caloric intake (specifically, reduced carbohydrate craving), not through direct enhancement of fat oxidation or metabolic rate. The downstream weight loss is therefore a secondary consequence of behavioral intake reduction rather than a direct pharmacological effect on adipose tissue.
That said, the body of clinical evidence does include several well-conducted trials showing modest but statistically significant fat-mass reduction, lean-mass increase, or both. The effect sizes are smaller than the marketing implied but larger than zero. The most fair characterization is: chromium picolinate is a modestly useful adjunct in patients whose weight gain is partly driven by carbohydrate over-consumption, especially in the setting of insulin resistance, with realistic expected effect on the order of 1–3 kg over 8–24 weeks. It is not a substitute for caloric restriction, dietary quality improvement, or physical activity.
The Kaats Body Composition Trials
Gilbert R. Kaats, working at Health and Medical Research Foundation in San Antonio, conducted the two most carefully measured chromium-and-body-composition trials of the 1990s. Both used hydrostatic weighing (the gold-standard body-composition method at the time, since superseded by DXA) to quantify lean and fat mass separately, rather than relying on bathroom-scale weight change.
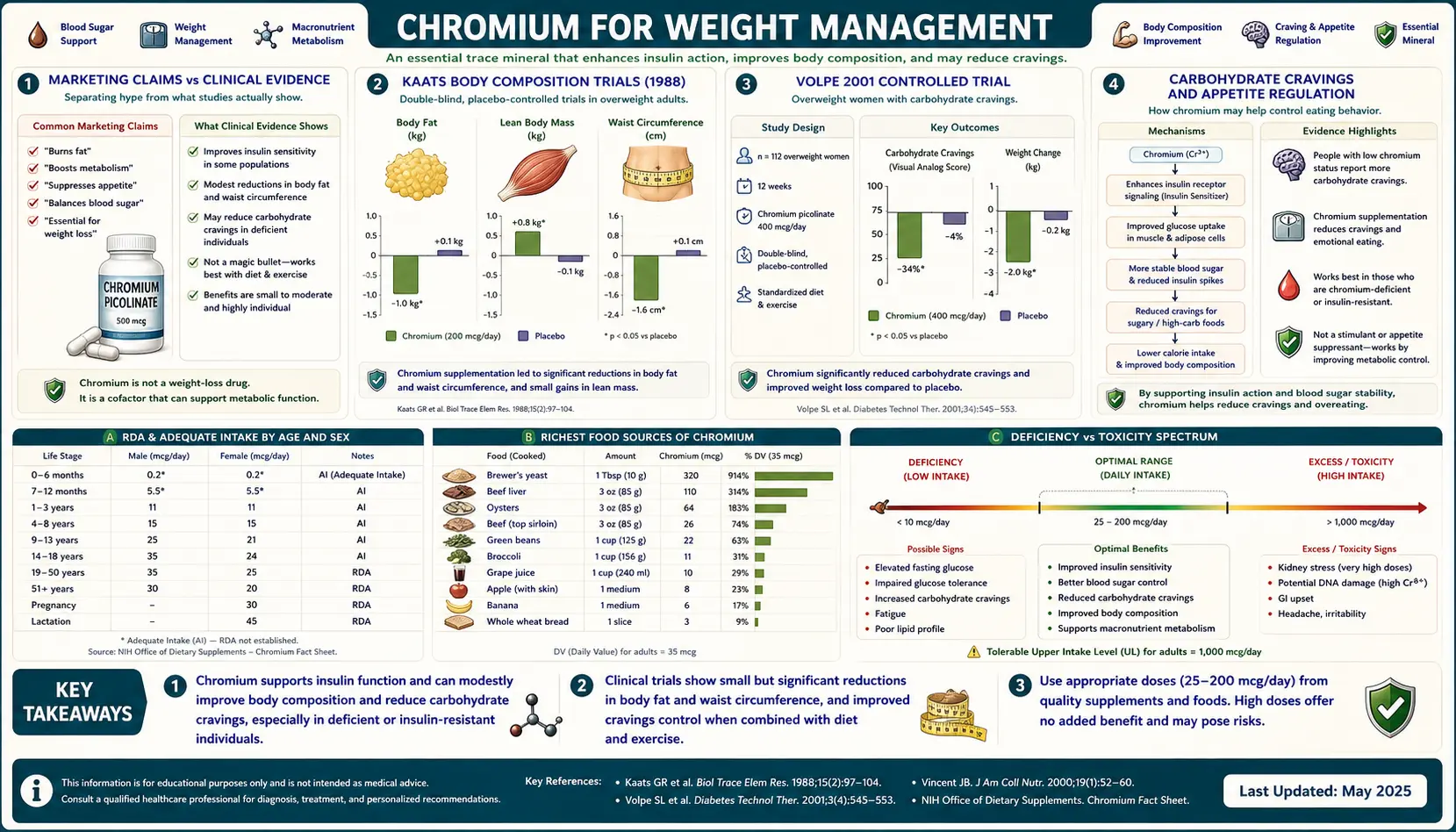
- Kaats 1996 — randomized, double-blind, placebo-controlled trial of 200 mcg/day or 400 mcg/day chromium picolinate vs placebo in 154 free-living adults for 72 days. The 400 mcg/day group lost approximately 4.6 kg of fat mass while gaining 1.4 kg of lean mass (net body weight change was modest because of the offsetting lean gain). The 200 mcg/day group showed intermediate changes. The placebo group showed minimal change. The body-composition specificity was important: it ruled out the alternative explanation that any chromium-attributable weight loss was simply water loss or muscle loss.
- Kaats 1998 — larger replication trial (n=122 with full follow-up), 90 days, 400 mcg/day chromium picolinate or placebo. Confirmed the directional finding of fat mass reduction with chromium relative to placebo, though effect magnitude was smaller than in the 1996 trial. Both arms received instruction in caloric restriction and exercise, so the absolute weight changes reflected the combined intervention with chromium contributing as an adjunct.
The Kaats trials were criticized after publication on several methodological grounds: subject self-selection through advertising, modest follow-up duration, and the involvement of chromium-industry funding. The hydrostatic-weighing technique was state-of-the-art for the era but is more variable than modern DXA scanning. Critics argued the effect sizes were near the limit of measurement precision.
Subsequent replication has been heterogeneous. Multiple smaller trials in the 1990s and 2000s confirmed directional fat-mass reduction with chromium picolinate; an approximately equal number found no effect. The Onakpoya 2013 meta-analysis pooling 11 trials (n=866) found a statistically significant but modest mean body-weight reduction of -0.50 kg favoring chromium picolinate, with substantial heterogeneity across trials.
The Volpe 2001 Controlled Trial
Stella L. Volpe published a particularly carefully controlled trial in Journal of the American College of Nutrition in 2001, addressing several methodological criticisms of the earlier Kaats work. Forty-four moderately obese women were randomized to 400 mcg/day chromium picolinate or placebo for 12 weeks. All subjects participated in a structured exercise program (aerobic and resistance training) and received standardized dietary counseling. Body composition was measured by DXA.
Results:
- Both groups lost weight (mean approximately 2.5 kg) with no significant between-group difference in absolute weight change
- Chromium group showed greater body-fat percentage reduction
- Chromium group showed slightly greater lean mass preservation
- No significant difference in resting metabolic rate or maximum oxygen uptake
The Volpe interpretation: chromium picolinate produced a modest favorable shift in body composition (greater fat loss, better lean mass preservation) during a structured weight-loss program, without affecting whole-body metabolic rate. The effect was small in absolute terms (a few percentage points of body-fat percentage difference) but consistent in direction with the Kaats findings.
The Volpe trial is methodologically the strongest of the chromium-body-composition trials because of the structured exercise and dietary controls, the DXA measurement, and the absence of industry funding. Its modest positive finding probably represents the best available estimate of true effect magnitude in motivated free-living adults engaged in concurrent lifestyle modification.
Trials in non-motivated, non-exercising, non-dieting populations have generally found smaller or null effects. This is consistent with the broader principle that chromium picolinate acts as an adjunct that potentiates the effects of other weight-loss interventions rather than as a stand-alone weight-loss agent.
Carbohydrate Cravings and Appetite Regulation
The most reproducible and clinically meaningful effect of chromium picolinate on body weight appears to be reduction in carbohydrate cravings, with downstream caloric intake reduction. Multiple trials measuring food cravings or appetite as primary or secondary endpoints have found chromium picolinate to reduce craving for sweet and starchy foods specifically.
The mechanism is plausibly tied to improved insulin signaling in the central nervous system. Glucose-sensing neurons in the hypothalamus respond to insulin and to circulating glucose, and they regulate hunger through downstream effects on neuropeptide Y, agouti-related peptide, pro-opiomelanocortin, and other appetite-controlling peptides. When insulin signaling at these neurons is impaired (the central nervous system equivalent of peripheral insulin resistance), appetite regulation is dysregulated — chronic hunger, craving for energy-dense palatable foods, and difficulty achieving satiety. Restored insulin signaling in these neurons normalizes appetite regulation.
The carbohydrate-specific nature of the craving reduction is consistent with this mechanism. Carbohydrate-rich foods drive larger insulin surges than fat- or protein-rich foods, and the brain's homeostatic response to chronic carbohydrate over-consumption produces craving signals to maintain the elevated intake. Breaking this cycle through pharmacological insulin sensitization (or in the chromium case, modest nutritional insulin sensitization) reduces the craving signal.
The clinical translation: chromium picolinate may be particularly useful for patients whose weight challenges are driven by chronic carbohydrate over-consumption and snacking, especially evening snacking on sweets and processed carbohydrates. It is less likely to be useful for patients whose overconsumption is more uniformly distributed across macronutrients or whose weight is driven by reduced physical activity rather than excess intake.
The Davidson Atypical Depression Trial
The strongest mechanistic evidence for chromium's effect on carbohydrate craving comes from Jonathan R. T. Davidson's 2003 trial of chromium picolinate in atypical depression. Atypical depression is a subtype characterized by mood reactivity, leaden paralysis, hypersomnia, and (most relevant here) increased appetite with carbohydrate craving. Standard antidepressants treat atypical depression less well than monoamine oxidase inhibitors, and the carbohydrate-craving component contributes to weight gain that further worsens mood.
Davidson's design: 15 adults meeting DSM-IV criteria for atypical depression, randomized 2:1 to 600 mcg/day chromium picolinate or placebo for 8 weeks. Primary outcome was the Hamilton Depression Rating Scale; secondary outcomes included specific atypical depression symptoms and a measure of carbohydrate craving.
Results:
- Hamilton Depression Rating Scale: significant improvement in chromium group vs placebo
- Carbohydrate craving: significantly reduced in chromium group
- Increased appetite: significantly reduced in chromium group
- Leaden paralysis: improved in chromium group
- Modest weight reduction in chromium group (secondary to reduced caloric intake from craving suppression)
The Davidson 2003 trial was small but significant for two reasons. First, it provided the cleanest demonstration that chromium picolinate's effect on carbohydrate craving was a clinical effect rather than a measurement artifact — the carbohydrate-craving questionnaire showed a clear chromium-vs-placebo signal in a population specifically selected for this symptom. Second, it suggested a broader role for chromium in the neuropsychiatric setting where insulin sensitization in the brain may have antidepressant effects.
A larger replication trial (Docherty 2005, n=113 atypical depression) confirmed the carbohydrate-craving and appetite-suppressing effects of chromium picolinate, with somewhat less impressive effects on overall depression scores. The collective evidence supports chromium picolinate as a reasonable adjunct in atypical depression with carbohydrate-craving features, particularly when standard antidepressants have been inadequate or poorly tolerated.
Serotonergic and Noradrenergic Mechanism
The proposed mechanism for chromium's effects on appetite and mood involves the serotonergic and noradrenergic neurotransmitter systems. Both serotonin and norepinephrine are appetite-regulating neurotransmitters, and both are functionally affected by insulin signaling in the brain.
- Serotonergic effects — serotonin is a major satiety neurotransmitter, and serotonergic dysfunction is associated with carbohydrate craving (the so-called "carbohydrate-craving serotonin hypothesis" originally proposed by Wurtman and Wurtman in the 1970s). Insulin signaling in the brain enhances tryptophan uptake into serotonergic neurons (insulin promotes amino acid uptake into other tissues, which competitively reduces large neutral amino acids in plasma except for tryptophan, which has its own transport mechanism — the net effect is increased tryptophan availability for serotonin synthesis). Restored insulin signaling from chromium supplementation should therefore enhance brain serotonin synthesis and serotonergic tone.
- Noradrenergic effects — norepinephrine in the hypothalamic paraventricular nucleus is appetite-suppressing (this is the mechanism of older anorectic drugs like phentermine, which is a norepinephrine-releasing agent). Chromium has been shown in animal studies to affect noradrenergic neurotransmission in the hypothalamus, though the mechanism is less well-characterized than the serotonergic mechanism.
- Dopaminergic effects — the rewarding aspect of palatable food consumption is mediated through mesolimbic dopaminergic signaling. There is preliminary evidence that chromium may modestly modulate dopaminergic function, potentially reducing food reward salience, though this is more speculative.
The integrated mechanistic picture: chromium picolinate, by improving insulin signaling in the central nervous system, modulates multiple appetite-regulating neurotransmitter systems in directions that favor satiety and reduce specifically carbohydrate craving. This is mechanistically distinct from the appetite suppressant drugs (phentermine, lorcaserin, GLP-1 agonists) but operationally similar in producing reduced caloric intake.
The GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) have substantially transformed the obesity pharmacology landscape since 2020 and produce far larger weight loss than chromium picolinate. Chromium's clinical place is now narrower than it was before the GLP-1 era: as a low-cost adjunct for patients with mild-moderate weight challenges and carbohydrate craving who do not warrant pharmacological GLP-1 therapy, or as a complementary intervention for patients already on GLP-1 agonists.
Fat Mass vs Lean Mass Composition
An important sub-question for any weight-loss intervention is whether the weight lost is primarily fat or primarily lean tissue. Lean tissue loss is metabolically and functionally undesirable — it reduces resting metabolic rate, predisposes to weight regain, and (in older adults) accelerates sarcopenia.
The body-composition trials of chromium picolinate (Kaats, Volpe, and several smaller studies) consistently show preferential fat-mass loss with lean mass preservation or modest increase. The mechanism is plausibly the insulin sensitization itself: improved insulin signaling enhances amino acid uptake into skeletal muscle (insulin is an anabolic hormone, and muscle protein synthesis is partly insulin-dependent), which preserves muscle during caloric restriction. The same insulin sensitization in adipose tissue restores normal lipolysis suppression in the fed state and may enhance lipolysis in the fasted state.
The net body-composition effect is therefore favorable even when total weight change is modest: chromium-supplemented subjects in weight-loss trials tend to lose proportionally more fat and less muscle than placebo-supplemented subjects. The Volpe 2001 DXA data are the cleanest demonstration of this effect.
This has practical implications for older adults attempting weight loss. Loss of muscle mass during caloric restriction is a major concern in patients over 65, and any intervention that preserves muscle during weight loss is valuable for long-term function. Chromium picolinate is a reasonable adjunct in this context, alongside the more important interventions of adequate protein intake (1.0–1.2 g/kg/day in older adults attempting weight loss) and resistance training.
Exercise Synergy and Resistance Training
Resistance training is the most reliable intervention for preserving and building lean mass, and aerobic training is the most reliable intervention for caloric expenditure and improved insulin sensitivity. Chromium picolinate has been studied as an adjunct to both modalities, with mixed results.
- Resistance training — Lukaski 1996 (covered in detail in the Insulin Sensitivity deep-dive) is the classic citation. Modest favorable effects on body composition were observed in chromium-supplemented resistance trainers compared to placebo. Several subsequent trials have produced mixed results; the overall pattern suggests chromium picolinate may enhance the body-composition benefits of resistance training in untrained or moderately trained individuals but has minimal additional benefit in already highly trained athletes (whose insulin signaling is presumably already well-optimized through training adaptation).
- Aerobic training — the evidence here is sparser. Aerobic training itself improves insulin sensitivity substantially, and chromium's additive benefit is small. The Volpe 2001 trial (which included both aerobic and resistance training) is the cleanest evidence; it found favorable body composition changes with chromium during a combined exercise program.
- Athletes and trace element status — intense endurance training increases urinary chromium loss, raising the theoretical possibility that elite endurance athletes might develop chromium-marginal status with associated impaired glucose handling during prolonged exercise. The practical impact appears modest in well-nourished athletes. Routine chromium supplementation in athletes is not generally recommended in the absence of documented deficiency.
The clinical recommendation: chromium picolinate is reasonable as a small adjunct to a structured exercise and diet program for weight management. Patients should not expect chromium to substitute for exercise; the exercise effect is several-fold larger.
Supplement Quality and Reformulation Cautions
Chromium picolinate is sold in the United States as a dietary supplement under DSHEA (the Dietary Supplement Health and Education Act of 1994), which means it is not subject to the same pre-market regulatory review as prescription pharmaceuticals. Product quality and label accuracy vary considerably across manufacturers.
- Form authentication — products labeled "chromium picolinate" should contain authentic chromium picolinate, which is a specific 1:3 chromium-to-picolinate stoichiometry. Cheap or counterfeit products may contain chromium chloride or other inexpensive chromium forms with picolinate added separately, providing different bioavailability than legitimate chromium picolinate. Third-party tested brands (USP Verified, NSF Certified, ConsumerLab.com tested) provide some assurance of label accuracy.
- Dose accuracy — products are sometimes overdosed or underdosed relative to label claims. Reputable brands with third-party verification minimize this risk.
- Excipients and binders — chromium picolinate tablets often include binders, fillers, and disintegrants that vary in quality. Patients with sensitivities should choose minimally formulated products.
- Hexavalent chromium contamination — trivalent chromium (Cr3+) is the supplement form and is nutritionally safe. Hexavalent chromium (Cr6+) is an industrial toxicant and known carcinogen. Reputable supplement manufacturers ensure their chromium ingredient is pure trivalent; contamination with hexavalent chromium is a theoretical risk in unscrupulously sourced products and is one reason to choose third-party-verified brands.
- Storage — chromium picolinate is stable at room temperature in a sealed container. Heat and humidity accelerate degradation. Refrigeration is unnecessary.
- Combination products — many weight-loss supplements combine chromium picolinate with stimulants (caffeine, synephrine), thyroid extracts, or other actives. These combinations multiply both potential benefits and potential adverse effects. Patients considering combination products should review each component independently.
The 2003 case of acute renal failure attributed to chromium picolinate (reported by Wani and colleagues in Annals of Pharmacotherapy) involved a young woman taking 1,200–2,400 mcg/day of chromium picolinate from a poorly-characterized product. The case prompted some regulatory attention but did not result in any restriction on chromium picolinate sales in the U.S. Standard therapeutic doses (200–1,000 mcg/day from quality-controlled products) appear safe long-term in monitored populations.
Realistic Expectations and Clinical Place
Realistic expectations for chromium picolinate as part of a weight-management strategy:
- Magnitude of weight loss — modest. The Onakpoya 2013 meta-analysis pooled effect was approximately 0.5 kg over 8–24 weeks. Individual responders may see 2–5 kg of fat loss; non-responders may see no change. This is substantially smaller than effects achievable with GLP-1 agonists (10–15% of body weight), bariatric surgery (25–35% of body weight), or sustained caloric restriction with exercise (5–10% of body weight).
- Time course — effects develop slowly over 8–24 weeks of consistent supplementation. Patients expecting acute weight loss within days or weeks will be disappointed. A 12-week trial is a reasonable evaluation period.
- Best-responder phenotype — insulin-resistant adults with carbohydrate craving and snacking patterns. Patients with metabolic syndrome, PCOS, or established type 2 diabetes are more likely to respond than otherwise-healthy adults seeking cosmetic weight loss.
- Combination with other interventions — chromium picolinate is best deployed as an adjunct to a structured diet and exercise program, not as a substitute for them. The Volpe 2001 trial design (combined diet + exercise + chromium) reflects the clinical reality.
- Dose — 200–400 mcg/day chromium picolinate is the dose range supported by most weight-management trials. Going higher (up to 1,000 mcg/day, the dose used in the Anderson Beijing diabetes trial) may produce slightly larger effects but with diminishing returns and small theoretical safety concerns at the upper end.
- Cost — chromium picolinate is among the cheapest weight-management supplements, typically $5–15 per month for a quality-verified product. The cost-benefit calculation is favorable even for modest expected effect.
- Stopping criteria — if no measurable benefit (weight change, body composition change, reduced carbohydrate craving) is observed after 12–16 weeks of consistent dosing in the context of an adequate weight-management program, chromium picolinate is unlikely to be helpful for that individual and can reasonably be discontinued.
For patients with severe obesity (BMI > 35) or weight-related medical complications, chromium picolinate should not delay initiation of evidence-based interventions including supervised lifestyle programs, GLP-1 agonists, or referral for bariatric surgery evaluation. For patients with mild-moderate weight challenges in the context of insulin resistance and carbohydrate cravings, chromium picolinate is a low-cost, low-risk adjunct with modest expected benefit.
This content is provided for informational purposes only and does not constitute medical advice. Patients with diabetes, kidney disease, or who are pregnant or breastfeeding should consult their physician before starting chromium picolinate supplementation. Chromium may potentiate the effect of insulin and oral antidiabetic drugs.
Key Research Papers
- Kaats GR, Blum K, Fisher JA, Adelman JA (1996). Effects of chromium picolinate supplementation on body composition: a randomized, double-masked, placebo-controlled study. Current Therapeutic Research 57(10):747-756. — PubMed
- Kaats GR, Blum K, Pullin D, Keith SC, Wood R (1998). A randomized, double-masked, placebo-controlled study of the effects of chromium picolinate supplementation on body composition: a replication and extension of a previous study. Current Therapeutic Research 59(6):379-388. — PubMed
- Volpe SL, Huang HW, Larpadisorn K, Lesser II (2001). Effect of chromium supplementation and exercise on body composition, resting metabolic rate and selected biochemical parameters in moderately obese women following an exercise program. Journal of the American College of Nutrition 20(4):293-306. — PubMed
- Davidson JR, Abraham K, Connor KM, McLeod MN (2003). Effectiveness of chromium in atypical depression: a placebo-controlled trial. Biological Psychiatry 53(3):261-264. — PubMed
- Docherty JP, Sack DA, Roffman M, Finch M, Komorowski JR (2005). A double-blind, placebo-controlled, exploratory trial of chromium picolinate in atypical depression: effect on carbohydrate craving. Journal of Psychiatric Practice 11(5):302-314. — PubMed
- Onakpoya I, Posadzki P, Ernst E (2013). Chromium supplementation in overweight and obesity: a systematic review and meta-analysis of randomized clinical trials. Obesity Reviews 14(6):496-507. — PubMed
- Tian H, Guo X, Wang X, et al. (2013). Chromium picolinate supplementation for overweight or obese adults. Cochrane Database of Systematic Reviews (11):CD010063. — PubMed
- Anton SD, Morrison CD, Cefalu WT, et al. (2008). Effects of chromium picolinate on food intake and satiety. Diabetes Technology and Therapeutics 10(5):405-412. — PubMed
- Lukaski HC, Bolonchuk WW, Siders WA, Milne DB (1996). Chromium supplementation and resistance training: effects on body composition, strength, and trace element status of men. American Journal of Clinical Nutrition 63(6):954-965. — PubMed
- Wani S, Weskamp C, Marple J, Spry L (2006). Acute tubular necrosis associated with chromium picolinate-containing dietary supplement. Annals of Pharmacotherapy 40(3):563-566. — PubMed
- Wurtman RJ, Wurtman JJ (1995). Brain serotonin, carbohydrate-craving, obesity and depression. Obesity Research 3(Suppl 4):477S-480S. — PubMed
- Trent LK, Thieding-Cancel D (1995). Effects of chromium picolinate on body composition. Journal of Sports Medicine and Physical Fitness 35(4):273-280. — PubMed
PubMed Topic Searches
- PubMed: Chromium picolinate weight-loss RCTs
- PubMed: Chromium and carbohydrate craving
- PubMed: Chromium for atypical depression
- PubMed: Chromium and body composition (DXA)
- PubMed: Chromium picolinate safety and renal effects
Connections
- Chromium Overview
- Chromium Benefits Hub
- Chromium for Blood Sugar
- Chromium for Insulin Sensitivity
- Chromium for Lipid Profile
- Obesity
- Metabolic Syndrome
- Insulin Resistance
- PCOS
- Depression
- Fasting
- Blood Sugar
- Berberine
- Cinnamon
- Magnesium
- Tryptophan
- Fasting Insulin
- HbA1c