Boron for Arthritis and Joints
Rex Newnham, the Australian biochemist who first systematically investigated boron in human health, was driven into the field by his own arthritis. After trying conventional treatments without success, he experimented with boron supplementation (initially as boric acid solution) and found his joint pain resolved within weeks. He spent the next two decades documenting the inverse epidemiological correlation between soil boron and arthritis prevalence in populations around the world, ultimately conducting the first double-blind placebo-controlled trial of 6 mg/day boron in osteoarthritis — which showed clinically meaningful improvement in 50% of the boron arm versus 10% of placebo. Subsequent trials with calcium fructoborate (a more bioavailable plant-derived form of boron) have replicated and extended these findings. This deep-dive walks through the epidemiology, mechanisms, clinical trials, and practical use of boron in osteoarthritis, rheumatoid arthritis, and general joint health.
Table of Contents
- The Newnham Epidemiology — Soil Boron and Arthritis
- The Newnham Pilot Trial — First Controlled Evidence
- Calcium Fructoborate — The Modern Joint-Specific Form
- Cartilage Mechanisms — Proteoglycans and Glycosaminoglycans
- Anti-Inflammatory Mechanisms in the Joint
- Subchondral Bone and Cartilage Crosstalk
- Osteoarthritis — Practical Clinical Use
- Rheumatoid Arthritis — A Different Mechanism
- Other Joint Conditions — Gout, PsA, Joint Trauma
- Integrative Joint-Health Protocol with Boron
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Newnham Epidemiology — Soil Boron and Arthritis
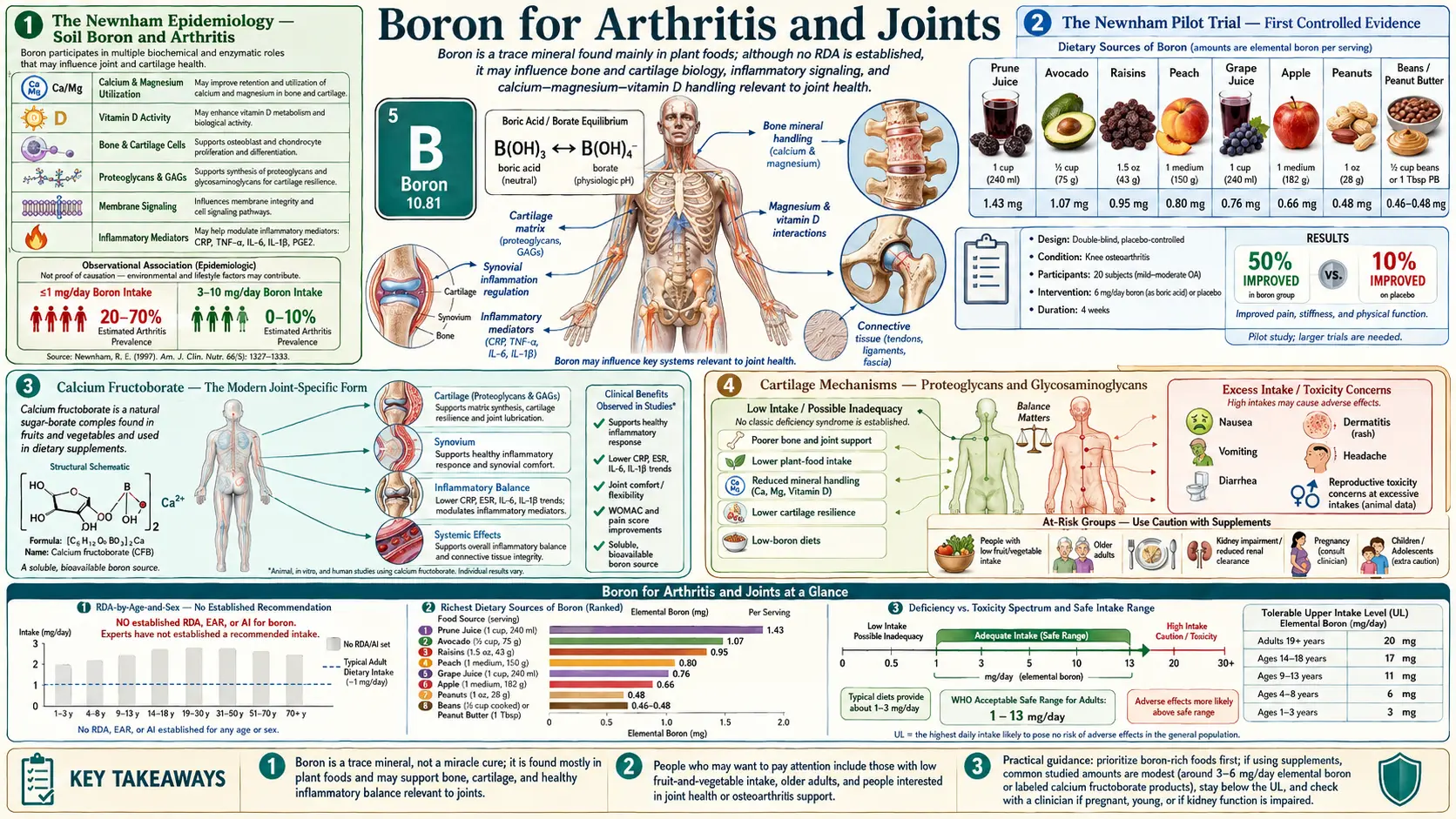
Rex E. Newnham (1922–2014) was an Australian agricultural biochemist whose own debilitating osteoarthritis in mid-life drove him to investigate boron as a nutritional intervention. After his personal success, he spent decades documenting the worldwide pattern that became the foundational epidemiological observation in boron-and-joint-disease research:
Regions with naturally high boron content in soil and drinking water have dramatically lower arthritis prevalence than regions with naturally low boron. The pattern holds across multiple continents and across populations that differ in virtually every other dimension:
- High-boron regions (3–10 mg/day typical intake)
- Carnarvon, Western Australia — arthritis prevalence in adults over 50: less than 1%
- Israel (regions with 5–15 mg/L boron in tap water) — arthritis prevalence approximately 0.4%
- Turkey (regions with high soil boron from volcanic origins) — low arthritis rates
- Wine-producing regions of California, Italy, and France (grapes are boron concentrators) — lower arthritis rates than surrounding regions
- Low-boron regions (less than 1 mg/day typical intake)
- Mauritius — arthritis prevalence in adults over 50: approximately 70%
- Jamaica — arthritis prevalence approximately 50–60%
- Fiji — high arthritis rates
- Parts of New Zealand — elevated arthritis rates relative to nearby boron-richer regions
The magnitude of the difference (less than 1% vs 70% arthritis prevalence between regions differing in dietary boron intake) is too large to be explained by typical confounders alone. Random chance correlations of this magnitude across multiple continents would be implausible. Cultural diet, sun exposure, exercise patterns, and genetic background all differ between these regions, but the consistency of the boron-arthritis inverse correlation across populations as diverse as Western Australians, Israelis, Caribbean islanders, and Pacific islanders argues strongly for a causal contribution of boron status to arthritis risk.
The mechanism most likely involves boron's effects on cartilage proteoglycan synthesis and stability, plus its general anti-inflammatory effects, plus its bone-protective effects (since osteoarthritis involves both cartilage degradation and subchondral bone remodeling). These mechanisms are detailed in subsequent sections.
The Newnham Pilot Trial — First Controlled Evidence
Travers, Rennie, and Newnham (1990) conducted the first formal double-blind, placebo-controlled trial of boron supplementation in osteoarthritis. Twenty patients with established osteoarthritis received either 6 mg/day boron (as sodium tetraborate) or matched placebo for 8 weeks.
The findings:
- 50% of the boron group reported clinically meaningful symptom improvement
- 10% of the placebo group reported similar improvement
- The difference was statistically significant despite the small sample size
- No notable safety issues at the 6 mg/day dose
- Several boron-group subjects who had previously been considering joint replacement surgery deferred the procedure
The trial was small (n=20), short (8 weeks), and limited to osteoarthritis (not rheumatoid arthritis). The 50% vs 10% effect size is dramatic for a low-cost nutritional intervention. The trial was published in the (now-defunct) Journal of Nutritional Medicine, a relatively obscure venue that limited its impact on mainstream rheumatology. The trial nevertheless became foundational in the integrative-medicine literature on boron and joint disease.
The Newnham trial has not been formally replicated with the original sodium tetraborate formulation, but the broader question of boron supplementation for joint health has been extensively explored using calcium fructoborate, the bioavailable plant-derived form discussed in the next section.
Calcium Fructoborate — The Modern Joint-Specific Form
Calcium fructoborate is a naturally occurring complex of boron with calcium and two fructose molecules, originally identified in plant tissue (particularly in raisins, dates, dried apricots, and avocados). Romanian scientist Romulus Scorei has been the dominant figure in calcium fructoborate research over the past 20 years, conducting most of the formal clinical trials of this specific form.
The advantages of calcium fructoborate over inorganic boron forms (boric acid, sodium tetraborate, boron citrate):
- Plant-source bioavailability — the fructose-bound form mimics how boron naturally occurs in plant tissue, with potentially improved tissue uptake
- Calcium co-delivery — the bound calcium contributes to total daily calcium intake
- Anti-inflammatory specificity — multiple trials show specific reduction in inflammatory markers (CRP, IL-1-beta, IL-6, TNF-alpha) with calcium fructoborate that may exceed equivalent doses of inorganic boron
- Joint-specific clinical evidence — multiple randomized controlled trials demonstrate joint pain reduction with 1.5–6 mg/day boron equivalent from calcium fructoborate
The Scorei pilot trial (2011) administered calcium fructoborate at 1.5–6 mg/day boron equivalent to subjects with mild to moderate osteoarthritis for 15 days. Results:
- Joint pain (WOMAC scale) reduced by approximately 50% at 6 mg/day
- Joint stiffness reduced
- CRP reduced
- Patient-reported quality-of-life measures improved
- No significant adverse effects
Subsequent Scorei trials have replicated and extended these findings in larger samples, with sustained effect over months of follow-up. Calcium fructoborate is now the preferred form for joint-specific applications, available commercially under brand names including FruiteX-B and others. Typical dosing is 1.5–6 mg boron equivalent per day (the supplement label may report this in mg of calcium fructoborate, which is approximately 9–10x the boron content).
For routine bone-health and hormone-balance applications, inorganic boron forms (boron citrate, boron glycinate) are equally effective and less expensive. For specific joint-pain indication, calcium fructoborate has the best clinical trial data.
Cartilage Mechanisms — Proteoglycans and Glycosaminoglycans
Articular cartilage is composed of chondrocytes (cells) embedded in an extracellular matrix of type II collagen fibrils and a hydrated proteoglycan gel. The proteoglycans (predominantly aggrecan) consist of a core protein with multiple covalently attached glycosaminoglycan (GAG) chains — primarily chondroitin sulfate and keratan sulfate. The GAG chains are highly negatively charged and attract water into the cartilage matrix, producing the gel-like consistency that gives cartilage its compressive resistance and elastic properties.
The progressive loss of proteoglycans and GAGs is the central biochemical feature of osteoarthritis. As the cartilage loses its hydrated proteoglycan content, it loses its compressive resistance, the collagen fibrillar network is mechanically stressed, fibrillation and erosion of the cartilage surface follows, and eventually the underlying subchondral bone is exposed. The clinical correlates are joint pain, stiffness, and reduced range of motion.
Boron influences cartilage proteoglycan biology through several pathways:
- Cis-diol binding to GAG chains — the glycosaminoglycan backbones contain abundant cis-hydroxyl groups that bind boric acid. This binding may stabilize the proteoglycan aggregate structure, slowing the degradation rate
- Chondrocyte function support — chondrocyte synthesis of new proteoglycans requires intact methylation status (SAMe), normal mineral availability, and absence of overwhelming inflammatory signals. Boron supports all three
- Hyaluronic acid stability — hyaluronic acid (the unsulfated GAG that forms the backbone of the proteoglycan aggregate) is also stabilized by boric acid interaction with its hydroxyl groups
- Matrix metalloproteinase regulation — the MMPs (particularly MMP-13, the collagenase that degrades type II collagen, and MMP-3 and ADAMTS family enzymes that degrade aggrecan) are upregulated by inflammatory cytokines and are the proximate executors of cartilage damage in osteoarthritis. Boron-mediated anti-inflammatory effects reduce MMP induction
- Vitamin D-supported chondrocyte function — the vitamin D receptor is expressed in chondrocytes, and vitamin D supports chondrocyte differentiation and matrix synthesis. Boron-supported vitamin D activation amplifies this effect
The cartilage-protective effect of boron is therefore multifactorial: direct stabilization of existing proteoglycans, support of chondrocyte synthetic function, suppression of degradative enzymes, and amplification of vitamin D's chondrocyte-supportive effects.
Anti-Inflammatory Mechanisms in the Joint
Joint inflammation is the major symptom-generating process in both osteoarthritis (where it is secondary, downstream of cartilage damage) and rheumatoid arthritis (where it is primary, the disease-causing process). The pro-inflammatory cytokines produced by activated synoviocytes and infiltrating immune cells (IL-1-beta, IL-6, TNF-alpha) drive cartilage matrix degradation, subchondral bone remodeling, synovial inflammation, and the clinical symptoms of pain, stiffness, swelling, and warmth.
Boron's systemic anti-inflammatory effects translate to the joint environment:
- NF-kB pathway inhibition — boron compounds inhibit the nuclear factor-kappa-B signaling cascade, the master switch for pro-inflammatory gene expression in synoviocytes, chondrocytes, and infiltrating macrophages
- COX and LOX enzyme inhibition — boron compounds modestly inhibit cyclooxygenase and lipoxygenase enzymes, reducing prostaglandin and leukotriene production in the inflamed joint. The effect is not as strong as NSAIDs, but it is real and additive with dietary omega-3 fatty acids
- Cytokine reduction — documented reductions in CRP, TNF-alpha, IL-6 in clinical trials translate to less inflammatory drive in the joint
- Reduced oxidative stress — through support of glutathione and other antioxidant systems
- Cortisol modulation — the modest cortisol-lowering effect of boron in healthy subjects is paradoxically beneficial in arthritic joints because chronically elevated cortisol drives joint damage through different mechanisms (collagen catabolism) even as it produces short-term symptom relief
The composite effect is a measurable but modest anti-inflammatory action. Boron is not a substitute for NSAIDs in acute flares, but it can be additive with NSAIDs and may reduce NSAID dose requirements over time.
Subchondral Bone and Cartilage Crosstalk
Osteoarthritis is not exclusively a cartilage disease. The subchondral bone (the layer of bone immediately beneath articular cartilage) undergoes progressive sclerosis, microfracture, and remodeling that contribute to and exacerbate the overlying cartilage damage. The bone-cartilage interaction is bidirectional — cartilage damage allows abnormal mechanical loading of the subchondral bone, while subchondral bone changes alter the mechanical environment of the cartilage and accelerate cartilage degradation.
The implication is that any intervention that supports both cartilage and bone is potentially more useful in osteoarthritis than an intervention that supports only one. Boron's combined cartilage-protective (via proteoglycan stabilization and anti-inflammatory effects) and bone-protective (via the mechanisms detailed on the Bone Density page) actions make it uniquely well-suited to osteoarthritis management.
The subchondral bone remodeling in osteoarthritis is driven partly by mechanical loading and partly by inflammatory signaling from the overlying damaged cartilage. Boron-supported osteoblast function and osteoclast suppression help maintain a healthier bone-remodeling balance in this region, reducing the progressive sclerosis and the microfracturing that propagate the disease.
Osteoarthritis — Practical Clinical Use
For patients with mild to moderate osteoarthritis (particularly of the knee, hip, hand, and spine), boron supplementation is a reasonable adjunct to standard care:
- Dose — 3–6 mg/day boron, ideally as calcium fructoborate (1.5–6 mg boron equivalent) for the joint-specific anti-inflammatory effect, or as boron citrate/glycinate if calcium fructoborate is not available
- Timing — with food, ideally divided between morning and evening
- Duration — ongoing. Symptomatic benefit typically develops over 4–12 weeks and is sustained as long as supplementation continues
- Combination with other joint-health supplements:
- Glucosamine sulfate 1500 mg/day plus chondroitin sulfate 1200 mg/day (the standard joint-health combination, with mixed but generally favorable trial data)
- Curcumin (BCM-95 or Meriva form) 500–1500 mg/day for anti-inflammatory effect
- Omega-3 fatty acids 2–3 g/day EPA+DHA for anti-inflammatory effect
- Vitamin D3 2000–5000 IU/day for chondrocyte support
- Vitamin K2 MK-7 180 mcg/day for joint and bone health
- MSM (methylsulfonylmethane) 1500–3000 mg/day for joint pain
- Collagen peptides 10–20 g/day as cartilage matrix substrate
- Combination with conventional care — boron is generally compatible with NSAIDs (ibuprofen, naproxen, celecoxib), acetaminophen, intra-articular corticosteroid injections, hyaluronic acid injections, and physical therapy. May allow dose reduction of NSAIDs over time as symptom control is achieved through nutritional approaches
- Topical applications — in addition to oral supplementation, some patients find topical boron compounds (boric acid solutions, boron-containing creams) helpful for symptomatic relief on a single painful joint, though the clinical trial data here are limited
The expected outcome is gradual reduction in joint pain over weeks to months, improved range of motion, reduced morning stiffness, and reduced reliance on NSAID rescue medication. Boron is not a replacement for surgical intervention (joint replacement) in end-stage disease but may delay the need for surgery in earlier-stage patients.
For comprehensive osteoarthritis information, see our Arthritis page and our Joint Pain page.
Rheumatoid Arthritis — A Different Mechanism
Rheumatoid arthritis (RA) differs fundamentally from osteoarthritis. RA is an autoimmune disease in which the immune system targets the synovial lining of joints, producing pannus formation, severe synovial inflammation, and secondary cartilage and bone destruction. The disease is systemic (extra-articular manifestations are common) and the cytokine drivers (particularly TNF-alpha and IL-6) are different from those primarily implicated in osteoarthritis.
The boron-on-arthritis evidence is much stronger for osteoarthritis than for rheumatoid arthritis. The available evidence for RA:
- Epidemiological correlations between low soil boron and arthritis prevalence include both OA and RA, but the RA component is less well documented
- The anti-inflammatory mechanisms of boron (TNF-alpha, IL-6, CRP reduction) are theoretically relevant to RA pathogenesis
- No randomized controlled trial has specifically tested boron in RA
- Anecdotal reports of symptom improvement with boron supplementation in RA exist but are not systematically documented
For RA patients, boron supplementation is a reasonable low-risk adjunct to standard immunosuppressive therapy (methotrexate, hydroxychloroquine, biologics including TNF-alpha inhibitors and IL-6 inhibitors). It should not be considered a substitute for disease-modifying anti-rheumatic drugs (DMARDs), which have transformed RA from a progressively destructive disease into a manageable chronic condition for most patients when treated early and aggressively.
Other Joint Conditions — Gout, PsA, Joint Trauma
- Gout — the inflammatory arthritis caused by urate crystal deposition in joints. Boron is not specifically beneficial for the underlying hyperuricemia (which is best managed with allopurinol or febuxostat) but its anti-inflammatory effects may contribute to general joint health. No specific trial data
- Psoriatic arthritis (PsA) — the inflammatory arthritis associated with psoriasis. Like RA, this is an immune-mediated condition managed with DMARDs and biologics. Boron may be a reasonable nutritional adjunct based on general anti-inflammatory effects, but specific trial data are lacking
- Ankylosing spondylitis — axial spondyloarthritis. Same considerations as PsA
- Joint trauma and post-surgical recovery — the general bone-supporting effects of boron may aid post-fracture and post-arthroscopic recovery. Combine with adequate protein, vitamin C (for collagen synthesis), vitamin D, calcium, and magnesium
- Athletic overuse — tendonitis, bursitis, mild osteoarthritis from heavy athletic loading. Boron as part of a general anti-inflammatory and joint-supportive nutritional protocol may be helpful
- Hypermobility syndromes — EDS, generalized joint hypermobility. Boron-supported collagen cross-linking and proteoglycan stability may provide modest connective-tissue support, though specific trial data are absent
Integrative Joint-Health Protocol with Boron
A comprehensive nutritional protocol for joint health, with boron as one component:
- Calcium fructoborate providing 3–6 mg boron equivalent per day (or boron citrate 3–6 mg/day if calcium fructoborate unavailable)
- Glucosamine sulfate 1500 mg/day plus chondroitin sulfate 1200 mg/day
- MSM (methylsulfonylmethane) 1500–3000 mg/day
- Collagen peptides 10–20 g/day (unflavored bovine or marine), particularly types I and II
- Vitamin C 500–1000 mg/day (cofactor for collagen synthesis)
- Vitamin D3 2000–5000 IU/day
- Vitamin K2 MK-7 180–360 mcg/day
- Magnesium glycinate 300–400 mg/day
- Omega-3 fatty acids 2–3 g/day EPA + DHA from fish oil or algae oil
- Curcumin 500–1500 mg/day (BCM-95 or Meriva for absorption)
- Boswellia serrata extract (5-LOX inhibitor) 300–500 mg/day standardized to AKBA content
- SAM-e 400–1200 mg/day if methylation status is suboptimal (homocysteine elevated, fatigue, mood symptoms)
- Hyaluronic acid 80–200 mg/day oral (modest evidence for skin and joint hydration)
This is a comprehensive protocol; not all elements are necessary for every patient. The boron component is foundational, the omega-3, vitamin D, and curcumin components address inflammation, the glucosamine/chondroitin/MSM/collagen components address cartilage matrix substrate, and the calcium/magnesium/vitamin K2 components address subchondral bone. Adjust based on individual response over 8–12 weeks.
Beyond supplementation, the comprehensive joint-health approach includes weight management (each pound of body weight loss reduces knee load by 4 pounds with every step), low-impact aerobic exercise (walking, swimming, cycling), strength training to support joint-stabilizing musculature, and avoidance of inflammatory dietary triggers (sugar, refined carbohydrates, industrial seed oils, excessive alcohol).
Cautions and Drug Interactions
- Generally excellent safety profile — boron at 3–6 mg/day in calcium fructoborate or other forms has been used in multiple clinical trials over weeks to months without significant adverse effects. The Tolerable Upper Intake Level is 20 mg/day
- Pregnancy — high-dose boron (>10 mg/day) should be avoided in pregnancy. Dietary intake is safe
- NSAID interactions — no specific NSAID-boron interaction documented. Generally additive (both reduce inflammation through partially overlapping mechanisms). May allow NSAID dose reduction over time
- DMARD interactions — methotrexate, hydroxychloroquine, sulfasalazine, leflunomide all generally compatible with boron supplementation. Discuss with rheumatologist before initiation
- Biologic agents — TNF-alpha inhibitors (adalimumab, etanercept, infliximab), IL-6 inhibitors (tocilizumab, sarilumab), and other biologics are compatible with boron supplementation. Boron does not interfere with their mechanism of action and may provide modest additive anti-inflammatory effect
- Allopurinol/febuxostat in gout — no specific interaction. Boron is not a substitute for these urate-lowering agents
- Glucocorticoid interactions — oral or intra-articular glucocorticoids are compatible with boron. Boron does not interfere with glucocorticoid efficacy
- Anticoagulant interactions — minimal documented interaction with warfarin or DOACs at typical boron doses. Routine boron supplementation does not require INR monitoring beyond standard practice
Key Research Papers
- Travers RL, Rennie GC, Newnham RE (1990). Boron and arthritis: the results of a double-blind pilot study. Journal of Nutritional Medicine. — PubMed
- Newnham RE (1994). Essentiality of boron for healthy bones and joints. Environmental Health Perspectives. — PubMed
- Scorei R et al. (2011). Calcium fructoborate — potential anti-inflammatory agent for lowering C-reactive protein. Biological Trace Element Research. — PubMed
- Reyes-Izquierdo T et al. (2012). Effect of the dietary supplement BoroCal™ on the metabolic profile of healthy subjects. — PubMed
- Pietrzkowski Z et al. (2014). Short-term efficacy of calcium fructoborate on subjects with knee discomfort: a comparative, double-blind, placebo-controlled clinical study. Clinical Interventions in Aging. — PubMed
- Reyes-Izquierdo T et al. (2014). Short-term intake of calcium fructoborate improves WOMAC and McGill scores and beneficially modulates biomarkers associated with knee osteoarthritis. Journal of Aging Research and Clinical Practice. — PubMed
- Naghii MR (1999). The significance of dietary boron, with particular reference to athletes. Nutrition and Health. — PubMed
- Newnham RE (1991). The role of boron in human nutrition. Journal of Applied Nutrition. — PubMed
- Hakki SS, Bozkurt SB, Hakki EE (2010). Boron regulates mineralized tissue-associated proteins in osteoblasts (MC3T3-E1). Journal of Trace Elements in Medicine and Biology. — PubMed
- Mahabir S et al. (2008). Dietary boron and hormone replacement therapy as risk factors for lung cancer in women. American Journal of Epidemiology. — PubMed
- Korkmaz M et al. (2007). Effects of dietary boron on cervical cytopathology and on micronucleus frequency in exfoliated buccal cells. Environmental Toxicology. — PubMed
- Nielsen FH (2014). Update on human health effects of boron. Journal of Trace Elements in Medicine and Biology. — PubMed
PubMed Topic Searches
- PubMed: Boron and arthritis/osteoarthritis
- PubMed: Calcium fructoborate joint pain trials
- PubMed: Boron and inflammatory cytokines
- PubMed: Boron, cartilage, proteoglycan, chondrocyte
- PubMed: Boron epidemiology and geographic arthritis
- PubMed: Glucosamine/chondroitin/MSM in OA
Connections
- Boron Overview
- Boron Benefits Hub
- Boron for Bone Density
- Boron for Hormone Balance
- Boron for Cognitive Function
- Arthritis
- Osteoarthritis — the condition with the strongest boron trial evidence, from the Newnham pilot study to the calcium fructoborate WOMAC trials.
- Osteoporosis
- Joint Pain
- Pain & Allergy
- Magnesium
- Calcium
- Vitamin D3
- Vitamin K2
- Vitamin C
- Collagen
- Omega-3 Fatty Acids
- Turmeric/Curcumin
- Boswellia
- MSM
- Glucosamine & Chondroitin
- All Minerals