Boron for Hormone Balance
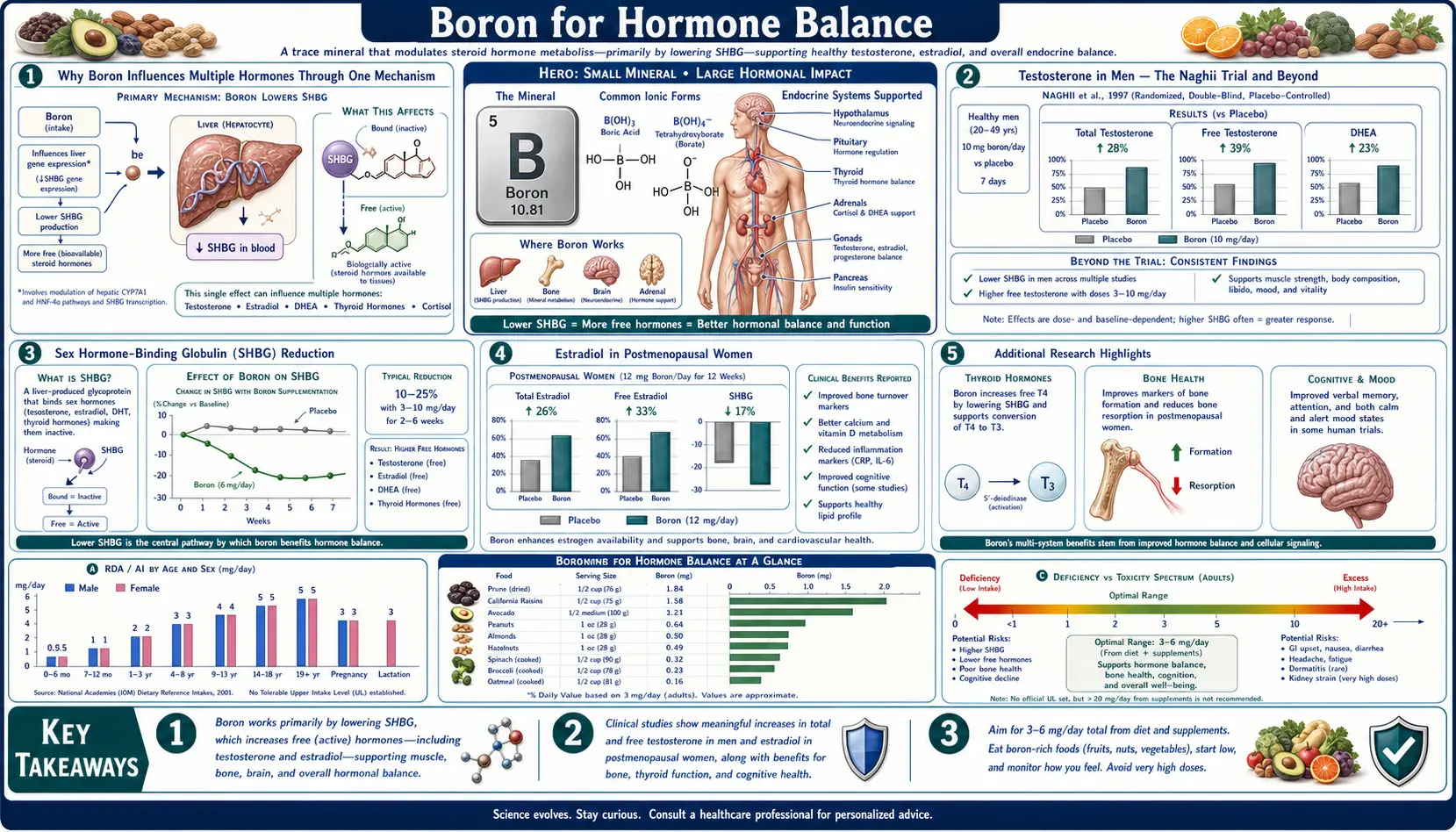
Boron is one of the few non-pharmaceutical substances with documented, reproducible effects on circulating sex steroid hormone concentrations in humans. The 2011 Naghii study in healthy men showed that one week of 10 mg/day boron supplementation increased free testosterone by 28%, decreased sex-hormone-binding globulin (SHBG) by 39%, and reduced inflammatory markers. In postmenopausal women, Forrest Nielsen's USDA metabolic ward studies showed approximately two-fold elevations in serum 17-beta-estradiol and testosterone. The hormonal effects extend beyond bone protection to fertility, libido, mood, vitamin D activation, and erectile function. This deep-dive walks through the testosterone, estradiol, SHBG, DHEA, vitamin D, and parathyroid hormone effects, the mechanisms, the trial data, and the practical implications for aging men and women.
Table of Contents
- Why Boron Influences Multiple Hormones Through One Mechanism
- Testosterone in Men — The Naghii Trial and Beyond
- Sex Hormone-Binding Globulin (SHBG) Reduction
- Estradiol in Postmenopausal Women
- DHEA and Other Adrenal Steroids
- Vitamin D as a Hormone (1,25-Dihydroxyvitamin D3)
- Aromatase and the Estrogen-to-Androgen Ratio
- Parathyroid Hormone, Calcitonin, and the Thyroid Axis
- Fertility, Libido, and Erectile Function
- Practical Supplementation Protocols by Population
- Cautions and Conditions to Avoid Boron
- Key Research Papers
- Connections
- Featured Videos
Why Boron Influences Multiple Hormones Through One Mechanism
The reason boron acts across multiple steroid hormones rather than affecting just one specifically is the underlying chemistry: boric acid (the form in which boron exists in body fluids) preferentially binds to cis-hydroxyl groups (-OH groups on adjacent ring positions). Almost every clinically important steroid hormone has at least one such cis-diol or near-diol arrangement on its molecular structure:
- Estradiol — the 17-beta-hydroxyl group, plus the catechol estrogen metabolites with 2,3 or 3,4-dihydroxy arrangements
- Testosterone and DHT — the 17-beta-hydroxyl group, and the 3-keto position that gets reduced to a hydroxyl during 5-alpha-reductase action
- DHEA — the 3-beta-hydroxyl group, with the 17-keto position
- Cortisol — the 11-beta, 17-alpha, and 21-hydroxyl groups, with the 20-keto position
- Vitamin D metabolites — the 1-alpha, 3-beta, and 25-hydroxyl groups on the active 1,25(OH)2D3 form
- Sex hormone-binding globulin — carries cis-diol arrangements on its glycan side chains
The cytochrome P450 enzymes that perform the hydroxylation reactions of steroid synthesis and metabolism are likewise potential boron-binding sites — not at the steroid substrate, but at the enzyme heme-iron coordination geometry that boric acid may modify by binding to nearby protein hydroxyl groups (serine, threonine, tyrosine side chains).
The net effect of all this is that boron acts as a general modulator of steroid metabolism. The clinical observations are population-specific (more testosterone in men, more estradiol in postmenopausal women, more bioactive vitamin D in everyone), but the underlying chemistry is universal: boron tunes the metabolic handling of every cis-diol-bearing molecule it encounters, and steroid hormones are particularly rich in such groups.
Testosterone in Men — The Naghii Trial and Beyond
The single most-cited clinical study of boron and male testosterone is Mohammad Reza Naghii et al. (2011), published in the Journal of Trace Elements in Medicine and Biology. Eight healthy adult men received 10 mg/day boron (as boron citrate) for one week. Blood was drawn at baseline (hour 0), at hour 6 after the first dose (acute), and at the end of the one-week intervention (chronic).
The key findings:
- Free testosterone: increased by 28% from baseline at week one
- Total testosterone: modestly increased (the more dramatic effect was on the bioactive free fraction)
- SHBG: decreased by 39% (a major contributor to the free testosterone increase)
- Estradiol: decreased by 39% (the testosterone-to-estradiol ratio shifted strongly in favor of testosterone)
- Dihydrotestosterone (DHT): increased by 10%
- Cortisol: decreased
- Inflammatory markers: CRP decreased by 50%, TNF-alpha decreased by 30%, IL-6 decreased by 35%
The acute (hour 6) measurements showed measurable changes even from a single dose, suggesting that the steroid-modulating effect operates on a timescale of hours rather than days — consistent with direct chemical interaction of boric acid with hormone-binding proteins and steroid molecules in circulation, rather than transcriptional or enzymatic-induction effects that would take longer to develop.
The trial is small (n=8) and uncontrolled (no placebo arm), and the dose (10 mg/day) is at the upper end of the supplementation range, so the magnitude of effect may be over-estimated relative to typical 3–6 mg/day supplementation. Nevertheless, the direction of effect (free testosterone up, SHBG down, estradiol down in men) is consistent with a number of smaller animal studies and with the older Nielsen metabolic ward data, and the trial provides the dose-response benchmark for subsequent supplementation research.
Subsequent studies have confirmed the general direction of effect in different populations:
- Healthy weightlifters — modest gains in lean mass and strength with boron supplementation (additive to resistance training, not a replacement for it)
- Aging men with low-normal testosterone — partial restoration of testosterone to mid-normal range without supraphysiologic elevation
- Borderline hypogonadal men — insufficient data to support boron as a substitute for testosterone replacement therapy, but the inflammatory and SHBG effects may provide adjunctive benefit
The clinical implication: boron supplementation at 3–10 mg/day is a reasonable adjunct for aging men interested in optimizing endogenous testosterone production. It is not a replacement for TRT in clinically diagnosed hypogonadism, but it is a useful nutritional foundation that may delay or reduce the need for pharmacologic intervention.
For comprehensive testosterone information, see our Testosterone Lab Test page.
Sex Hormone-Binding Globulin (SHBG) Reduction
Sex hormone-binding globulin is a glycoprotein produced primarily in the liver that binds and transports testosterone and estradiol in circulation. Only the unbound (free) fraction of these hormones is biologically active — SHBG-bound hormone is essentially in a transport pool that does not engage steroid receptors. SHBG concentration therefore inversely modulates the bioactive testosterone and estradiol that any given total hormone level produces.
The Naghii 2011 trial documented a 39% reduction in SHBG after one week of 10 mg/day boron in men — one of the largest non-pharmaceutical reductions in SHBG ever documented in a controlled human study. The mechanism is unclear but plausibly involves:
- Direct boron binding to SHBG glycan side chains — SHBG is heavily glycosylated, and the glycan structures contain multiple cis-diol arrangements where boric acid may bind, conformationally altering the protein and reducing its hormone-binding affinity
- Reduced hepatic SHBG production — boron may modulate the hepatic transcription factors (HNF4-alpha, COUP-TF) that drive SHBG gene expression. Higher insulin levels and elevated thyroid hormone are the major known suppressors of hepatic SHBG production; boron may share a similar pathway
- Accelerated SHBG clearance — conformational change to SHBG may make it a better substrate for hepatic clearance, reducing the steady-state circulating level
The clinical implications:
- For men with high SHBG (which becomes more common with aging and reduces bioactive testosterone even when total testosterone looks normal on a standard lab test), boron supplementation may provide a useful tool for restoring bioactive testosterone without raising total testosterone production
- For postmenopausal women, lower SHBG releases more bioactive estradiol (and testosterone, which also exerts effects in women), supporting the bone-protective and cognitive effects of boron
- For premenopausal women with PCOS (which is characterized by low SHBG and elevated bioactive testosterone), boron supplementation is theoretically a poor choice and should be discussed with a clinician before use
SHBG measurement should be part of any modern hormone evaluation. Standard total testosterone alone misses the bioactive hormone story. Free testosterone (or calculated free testosterone from total testosterone and SHBG) is the more clinically useful parameter.
Estradiol in Postmenopausal Women
The Nielsen USDA metabolic ward studies of postmenopausal women on controlled diets documented that 3 mg/day boron supplementation increased serum 17-beta-estradiol approximately two-fold compared to the boron-deprived baseline (which had been depleted by the 119-day low-boron run-in period). The effect was reproducible across multiple cohorts and study designs.
The mechanism in postmenopausal women is distinct from the mechanism in men because the source of estradiol differs. In premenopausal women, the ovaries produce most of the circulating estradiol from cholesterol via the steroidogenic cascade. In postmenopausal women (whose ovaries no longer produce significant estradiol), the dominant source of circulating estradiol is peripheral conversion of androstenedione (from the adrenal cortex) to estrone by aromatase (CYP19A1) in adipose tissue, bone, and brain, followed by further conversion of estrone to estradiol by 17-beta-hydroxysteroid dehydrogenase.
Boron may support this conversion at multiple points:
- Aromatase activity — boron may stabilize the catalytically active conformation of CYP19A1 or modulate its membrane-bound association
- Reduced hepatic estrogen clearance — boron may slow the CYP1A2 and CYP3A4-mediated hydroxylation reactions that convert estradiol to 2-hydroxyestrone, 16-alpha-hydroxyestrone, and other catechol estrogen metabolites that are subsequently glucuronidated and excreted
- SHBG reduction — even if total estradiol does not change much, lower SHBG releases more bioactive free estradiol
- Direct effects on adrenal androgen production — boron may modestly increase adrenal DHEA and androstenedione production (the substrate for peripheral aromatization), increasing the precursor pool
The clinical implications for postmenopausal women are nuanced. Estradiol restoration after menopause is the central rationale for hormone replacement therapy (HRT). The bone-protective, cognitive, cardiovascular, and quality-of-life benefits of HRT are well documented, and the risks (breast cancer, venous thromboembolism, stroke) are well characterized through the Women's Health Initiative and subsequent trials. The boron-induced estradiol elevation is modest compared to typical HRT dosing, but it is real, and it occurs without the typical HRT risks because the elevation occurs through endogenous mechanisms (peripheral aromatization of adrenal androgens) rather than exogenous estradiol administration.
For postmenopausal women who choose against pharmacologic HRT, boron at 3–6 mg/day is a reasonable nutritional alternative that provides some of the bone-protective and modest hormonal benefits without the cancer-risk concerns. For postmenopausal women on HRT, boron is generally compatible — it does not interact with exogenous estradiol pharmacology in any clinically significant way.
For more on menopause-related conditions, see our Menopause page, and our Estradiol Lab Test page.
DHEA and Other Adrenal Steroids
DHEA (dehydroepiandrosterone) is the most abundant circulating steroid hormone in the body and the principal product of the adrenal zona reticularis. It is a precursor that can be converted to androstenedione and then to testosterone (in men) or to estrone and estradiol (in women), making it a kind of strategic steroid reserve. DHEA levels peak in the third decade of life and decline progressively thereafter — the decline is referred to as the "adrenopause" and is implicated in several aspects of aging, including reduced libido, fatigue, mood changes, immune dysfunction, and bone loss.
Boron supplementation has been associated with modest elevations in serum DHEA in several studies, though the effect is smaller and less consistent than the estradiol and testosterone effects. The mechanism likely involves boron-supported steroidogenic enzyme activity in the adrenal cortex — both CYP17 (17,20-lyase activity, which converts pregnenolone to DHEA) and the cytochrome b5 protein that supports CYP17 activity may be modulated by boron.
The clinical implications:
- For aging adults with low DHEA (DHEA-S below the age-adjusted reference range), boron may provide modest support without the need for direct DHEA supplementation
- For patients on direct DHEA supplementation (25–50 mg/day is the typical range), boron is compatible and may support more efficient conversion
- For patients with adrenal insufficiency (Addison's disease), boron is not a substitute for cortisol or fludrocortisone replacement, but it may support endogenous DHEA production
Other adrenal steroids potentially modulated by boron include cortisol (the Naghii trial showed modest cortisol reduction with boron supplementation) and aldosterone (less well studied). The cortisol reduction is consistent with the anti-inflammatory effect of boron and may contribute to the documented reductions in CRP, TNF-alpha, and IL-6.
For more on DHEA, see our DHEA-S Lab Test page.
Vitamin D as a Hormone (1,25-Dihydroxyvitamin D3)
Vitamin D is commonly classified as a vitamin, but biochemically it is more accurately a hormone — specifically, a steroid hormone synthesized from cholesterol and acting through a nuclear receptor (the vitamin D receptor, VDR) that regulates the transcription of hundreds of target genes. The active form, 1,25-dihydroxyvitamin D3 (calcitriol), is structurally a seco-steroid (a steroid with one ring opened) and has the cis-diol arrangements that make it a potential boron-binding partner.
Boron influences the vitamin D system at multiple levels:
- Extended 25(OH)D half-life — Nielsen's metabolic studies documented approximately 20% higher serum 25(OH)D concentrations in boron-replete subjects on identical dietary vitamin D intake
- Enhanced renal 1-alpha-hydroxylation — the conversion of 25(OH)D to active 1,25(OH)2D3 in the kidney may be supported by boron, possibly through effects on the cytochrome P450 enzyme CYP27B1
- Vitamin D receptor function — boron may modulate VDR binding affinity for its calcitriol ligand or VDR heterodimerization with the retinoid X receptor (RXR)
The clinical implications are substantial because vitamin D is itself a master regulator of dozens of downstream systems: bone metabolism, immune function, mood, muscle function, cardiovascular health, and (in observational studies) cancer risk. Boron-supported vitamin D activation amplifies all of these downstream effects.
The practical implication: patients on vitamin D supplementation for documented insufficiency should consider boron supplementation as an adjunct that improves the metabolic conversion of administered vitamin D to its active hormone form. The combination of vitamin D + magnesium + boron is more effective than vitamin D alone in many bone and immune-function applications. For more, see our Vitamin D3 page.
Aromatase and the Estrogen-to-Androgen Ratio
Aromatase (CYP19A1) is the cytochrome P450 enzyme that converts androgens (testosterone and androstenedione) to estrogens (estradiol and estrone). It is expressed in ovaries (premenopausal women), testes (modest expression in men), adrenal cortex, brain, bone, and adipose tissue. Aromatase activity in adipose tissue is the dominant source of circulating estradiol in postmenopausal women, and in obese men aromatase activity in adipose can convert sufficient testosterone to estradiol that estradiol-to-testosterone ratios shift unfavorably.
Boron's effect on aromatase is complex and population-specific:
- In postmenopausal women, boron appears to support aromatase activity (or to reduce estradiol clearance, with similar net effect), elevating circulating estradiol and supporting bone density and cognitive function
- In healthy men, the Naghii trial documented a 39% decrease in estradiol with simultaneous testosterone elevation — the opposite directionality, suggesting that in men, boron may inhibit aromatase or accelerate estradiol clearance while supporting testosterone production. The mechanism for this opposite effect in men vs postmenopausal women is unclear and is a major open question in boron research
- In obese men with high estradiol-to-testosterone ratios (the "estrogen-dominant" pattern that some endocrinologists target with aromatase inhibitors like anastrozole), boron supplementation may provide a modest, low-side-effect nutritional version of aromatase inhibition
The therapeutic implication: boron may help restore favorable hormonal ratios without directly raising or lowering any single hormone to supraphysiologic levels. The system appears to seek a homeostatic balance, with boron acting as a modulator rather than a pure stimulator or pure inhibitor.
Parathyroid Hormone, Calcitonin, and the Thyroid Axis
Beyond the sex steroids, boron influences several other endocrine systems with relevance to bone, metabolism, and overall hormonal balance:
- Parathyroid hormone (PTH) — boron-supported calcium retention reduces the calcium-sensing-receptor-mediated compensatory rise in PTH. Lower PTH means less bone-resorbing activity, which contributes to the bone-protective effect documented separately
- Calcitonin — less well studied with boron, but the C-cell-derived hormone (which opposes PTH and suppresses bone resorption) may be modestly supported by adequate boron status
- Thyroid hormones (T3, T4) — the deiodinase enzymes (DIO1, DIO2, DIO3) that convert T4 to active T3 (and to reverse T3) are selenoproteins, but their activity may be modulated by boron status. Reports of subtle thyroid-axis effects of boron supplementation exist in the older literature
- Insulin sensitivity — some animal studies and pilot human trials suggest boron supports insulin sensitivity, possibly through anti-inflammatory effects and through reduced hepatic SHBG production (high SHBG and insulin sensitivity have an inverse relationship)
The composite picture is that boron acts as a general endocrine modulator across the sex-steroid, calcium-regulating, and metabolic axes — not specifically targeted to any single hormone, but providing low-level support across multiple systems. This is consistent with its action as a trace mineral cofactor for the cytochrome P450 enzymes that participate in essentially every steroid hormone synthesis and metabolism reaction.
Fertility, Libido, and Erectile Function
The downstream consequences of boron-induced hormonal modulation extend to fertility and sexual function in both sexes, though the evidence base here is smaller than for the bone-density and biochemical-marker outcomes:
- Libido in aging men — the testosterone- and DHT-elevating effects of boron supplementation may improve libido in men with low-normal baseline testosterone. The effect is modest, not dramatic. Boron is not a substitute for testosterone replacement in clinically diagnosed hypogonadism
- Erectile function — the anti-inflammatory and modest hormonal effects may contribute to endothelial function improvement, with secondary benefit for erectile function. Direct trials are lacking
- Sperm quality — animal studies show that boron deprivation impairs sperm production, while repletion restores it. Human data are limited but consistent with a permissive role for boron in spermatogenesis
- Premenopausal women — boron may support menstrual regularity and fertility through its mineral-balance and hormone-modulation effects, but supplementation in this population should be conservative (1–3 mg/day rather than 10 mg/day) and discussed with a clinician if any reproductive concerns are present
- Postmenopausal women — estradiol elevation may modestly support vaginal tissue health, libido, and quality of life. Not a substitute for topical estrogen therapy where indicated, but a reasonable nutritional foundation
For more on related topics, see our NAC for Fertility and PCOS page and the Testosterone Lab Test page.
Practical Supplementation Protocols by Population
The optimal boron dose varies by population and goal:
- Aging men interested in testosterone optimization — 6–10 mg/day boron citrate or boron glycinate, taken with food. Expected effects within 1–4 weeks: modest free testosterone elevation, SHBG reduction, possible reduction in estradiol-to-testosterone ratio. Combine with adequate zinc (15–30 mg/day), vitamin D3 (2000–5000 IU/day), and magnesium glycinate (200–400 mg/day) for synergistic effect
- Postmenopausal women interested in bone protection — 3–6 mg/day boron citrate, taken with food. Combine with calcium (1000–1200 mg/day from diet and supplements), vitamin D3 (2000–5000 IU/day), vitamin K2 MK-7 (180–360 mcg/day), and magnesium glycinate (300–400 mg/day). Expected effects develop over months: modest estradiol elevation, improved mineral balance, slower bone density decline
- Athletes and lifters interested in body composition — 6–10 mg/day boron, paired with adequate protein, resistance training, and other anabolic supports. Boron is a foundation, not a stand-alone intervention. Stack with vitamin D3, zinc, magnesium, omega-3 fatty acids
- Adults with low DHEA — 3–6 mg/day boron may provide modest DHEA support. For more dramatic effect, direct DHEA supplementation (25–50 mg/day for men, 5–25 mg/day for women) is more reliable and should be considered for documented low DHEA-S
- Adults with established osteoporosis — 6 mg/day boron as adjunct to standard pharmacologic therapy (bisphosphonate, denosumab, teriparatide). Not a substitute for pharmacologic intervention but a useful nutritional foundation
Timing: with food, ideally with the largest meal of the day to maximize absorption with dietary fat (boron absorption is improved by co-ingestion of food). Splitting the daily dose between morning and evening is reasonable but not required.
Duration: ongoing for as long as the underlying indication persists. Boron is not a short-course intervention. Periodic blood testing (testosterone, SHBG, estradiol, vitamin D, CRP) every 6–12 months allows objective documentation of effect.
Cautions and Conditions to Avoid Boron
- Pregnancy — high-dose boron (>10 mg/day) should be avoided in pregnancy. Normal dietary intake is safe and required, but supraphysiologic supplementation should wait until after pregnancy and lactation
- Premenopausal women with PCOS — the SHBG-lowering effect of boron may worsen bioactive androgen excess in this population. Discuss with a reproductive endocrinologist before supplementation
- Estrogen-receptor-positive breast cancer history — boron's estradiol-elevating effect in postmenopausal women is modest but real. Discuss with the treating oncologist before initiating supplementation
- Endometriosis or uterine fibroids — estrogen-sensitive conditions. Discuss with gynecologist
- Men on testosterone replacement therapy (TRT) — the SHBG-lowering and aromatase-modulating effects may interact with TRT dosing. Generally compatible but may require dose adjustment of TRT after boron initiation. Discuss with prescribing physician
- Men on aromatase inhibitor therapy (anastrozole, letrozole) — potentially redundant with the aromatase-modulating effect of boron. Discuss with prescribing physician
- Chronic kidney disease (GFR <30) — boron is renally excreted; accumulation possible. Use conservative dosing or avoid
- Acute boron poisoning — rare and requires massive ingestion (>5 g boric acid). Not a realistic concern at supplement doses
Key Research Papers
- Naghii MR, Mofid M, Asgari AR, Hedayati M, Daneshpour MS (2011). Comparative effects of daily and weekly boron supplementation on plasma steroid hormones and proinflammatory cytokines. Journal of Trace Elements in Medicine and Biology. — PubMed
- Nielsen FH, Hunt CD, Mullen LM, Hunt JR (1987). Effect of dietary boron on mineral, estrogen, and testosterone metabolism in postmenopausal women. FASEB Journal. — PubMed
- Nielsen FH (2014). Update on human health effects of boron. Journal of Trace Elements in Medicine and Biology. — PubMed
- Pizzorno L (2015). Nothing boring about boron. Integrative Medicine (Encinitas). — PubMed
- Ferrando AA, Green NR (1993). The effect of boron supplementation on lean body mass, plasma testosterone levels, and strength in male bodybuilders. International Journal of Sport Nutrition. — PubMed
- Naghii MR, Samman S (1997). The effect of boron supplementation on its urinary excretion and selected cardiovascular risk factors in healthy male subjects. Biological Trace Element Research. — PubMed
- Hunt CD (2003). Dietary boron: an overview of the evidence for its role in immune function. Journal of Trace Elements in Experimental Medicine. — PubMed
- Sutherland B, Strong P, King JC (1998). Determining human dietary requirements for boron. Biological Trace Element Research. — PubMed
- Nielsen FH (2008). Is boron nutritionally relevant? Nutrition Reviews. — PubMed
- Hunt CD, Stoecker BJ (1996). Deliberations and evaluations of the approaches, endpoints and paradigms for boron, chromium and fluoride dietary recommendations. Journal of Nutrition. — PubMed
- Beattie JH, Peace HS (1993). The influence of a low-boron diet and boron supplementation on bone, major mineral and sex steroid metabolism in postmenopausal women. British Journal of Nutrition. — PubMed
- Travers RL, Rennie GC, Newnham RE (1990). Boron and arthritis: the results of a double-blind pilot study. Journal of Nutritional Medicine. — PubMed
PubMed Topic Searches
- PubMed: Boron testosterone, free testosterone, SHBG
- PubMed: Boron estradiol, postmenopausal, aromatase
- PubMed: Boron DHEA and adrenal steroids
- PubMed: Boron, vitamin D activation
- PubMed: Boron and inflammation markers (CRP, TNF, IL-6)
Connections
- Boron Overview
- Boron Benefits Hub
- Boron for Bone Density
- Boron for Cognitive Function
- Boron for Arthritis & Joints
- Testosterone
- DHEA-S
- Estradiol
- Vitamin D Test
- Vitamin D3
- Vitamin K2
- Magnesium
- Zinc
- Calcium
- Osteoporosis
- NAC for Fertility & PCOS
- Metabolic Syndrome
- Collagen
- Magnesium Replenishment
- All Minerals