Sulfur for Joint Health
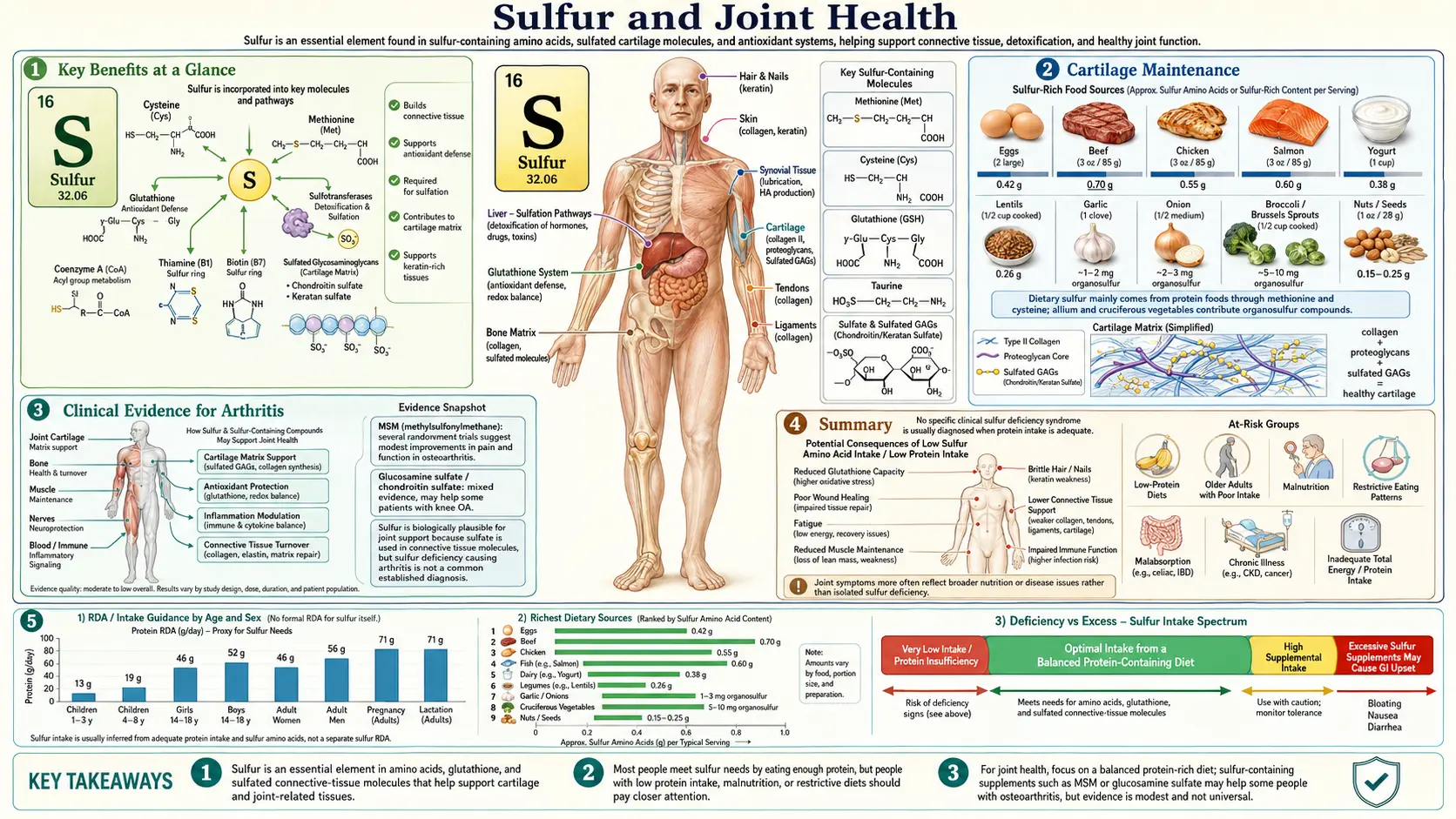
Sulfur is the structural backbone of healthy joints. Cartilage is roughly 75% water by mass, but the molecules that hold that water in place — sulfated glycosaminoglycans like chondroitin sulfate and keratan sulfate — are wholly dependent on sulfur. Three sulfur-derived interventions dominate the evidence base for osteoarthritis management: glucosamine sulfate at 1500 mg/day (the only nutraceutical with three-year structural data showing reduced joint-space narrowing), chondroitin sulfate at 800-1200 mg/day (an injected mimic of cartilage's own load-bearing polysaccharide), and MSM (methylsulfonylmethane) at 1.5-6 g/day (a bioavailable sulfur donor with potent NF-kB and MMP-suppressive activity). Together they address the three layers of joint pathology — substrate depletion, inflammatory degradation, and chondrocyte oxidative stress.
Table of Contents
- Why Sulfur Matters for Cartilage
- MSM (Methylsulfonylmethane)
- Chondroitin Sulfate Structure
- Cartilage Maintenance and Chondrocyte Biology
- Anti-Inflammatory Mechanisms
- Glucosamine Sulfate
- Clinical Evidence for Osteoarthritis
- Collagen Cross-Linking and Tendon/Ligament Strength
- Dosing and Dietary Sources
- Safety and Cautions
- Key Research Papers
- Connections
- Featured Videos
Why Sulfur Matters for Cartilage
Cartilage is a hydrated proteoglycan gel reinforced by a type II collagen fiber mesh. The gel itself is built from aggrecan — a core protein with roughly 100 chondroitin sulfate chains and 30 keratan sulfate chains projecting outward like a bottle brush. Each chondroitin sulfate chain carries about 100 negatively charged sulfate groups along its length. These negative charges repel each other (creating the swelling pressure that resists compression) and attract sodium cations (which in turn attract water by osmotic pressure). The result is the high-pressure water-filled matrix that allows knee cartilage to bear five times body weight without permanent deformation.
Every sulfate group in that matrix had to be installed by a sulfotransferase enzyme using the universal sulfate donor PAPS (3'-phosphoadenosine-5'-phosphosulfate). PAPS itself is synthesized from inorganic sulfate (SO42-) derived ultimately from dietary methionine and cysteine. When sulfur intake is marginal, PAPS pools deplete, sulfation of glycosaminoglycans drops, and the resulting cartilage matrix has reduced charge density, reduced water-binding capacity, and reduced compressive resistance. This is the biochemical substrate underneath the clinical observation that sulfur-replete diets and sulfur-based supplements help osteoarthritic joints — the matrix being rebuilt only works if the sulfur is there.
Compounding the structural requirement, the same chondrocytes responsible for matrix synthesis are also exquisitely sensitive to oxidative stress. The articular cartilage of synovial joints is avascular — nutrients reach chondrocytes only by diffusion through the matrix from the synovial fluid above and the subchondral bone below. Oxygen tension is low, ATP production marginal, and antioxidant reserves limited. Glutathione (itself sulfur-dependent through its cysteine residue) is the primary defense, and adequate sulfur status is therefore doubly important: as substrate for matrix and as cofactor for the antioxidant system that keeps the matrix-producing cells alive.
MSM (Methylsulfonylmethane)
MSM is the oxidized metabolite of dimethyl sulfoxide (DMSO) and the dominant organic sulfur compound circulating in human blood. It occurs naturally in trace amounts in fruits, vegetables, milk, and grains (typical dietary intake is 1-4 mg/day), and is also synthesized endogenously from intestinal bacterial action on dietary sulfur. Supplemental MSM (1.5-6 g/day in clinical trials) provides a roughly 1,000-fold increase over background intake.
- Bioavailable sulfur source — MSM crosses cell membranes freely (no transporter required), distributes broadly including across the blood-brain barrier, and provides sulfur in a form that is readily incorporated into the sulfation pathway via metabolism to inorganic sulfate.
- NF-kB pathway inhibition — MSM blocks the nuclear translocation of NF-kB, reducing transcription of pro-inflammatory cytokines (IL-1beta, IL-6, TNF-alpha) and the inducible enzymes iNOS and COX-2 that drive joint inflammation and chondrocyte apoptosis.
- Matrix metalloproteinase suppression — MSM reduces expression of MMP-1, MMP-3, and MMP-13, the collagenases and aggrecanases that degrade cartilage matrix in osteoarthritis. This is a disease-modifying mechanism, not just symptom suppression.
- Glutathione support — MSM increases intracellular glutathione, enhancing the activity of superoxide dismutase and catalase, protecting chondrocytes and synovial cells from oxidative damage that accelerates cartilage breakdown.
- Clinical pain reduction — multiple RCTs show MSM at 1.5-6 g/day significantly reduces WOMAC pain, stiffness, and physical function scores in knee osteoarthritis, with onset of benefit at 2-4 weeks and maximum effect by 12 weeks. Effect size is moderate but consistent.
- Safety profile — GRAS status from the FDA, very low toxicity, occasional mild GI upset, headache, or insomnia. Doses up to 6 g/day for 12 weeks show no clinically significant adverse events.
Chondroitin Sulfate Structure
Chondroitin sulfate is a long-chain polysaccharide composed of repeating disaccharide units of N-acetylgalactosamine and glucuronic acid, with sulfate groups installed at the 4- or 6-position of the N-acetylgalactosamine residues. In healthy adult cartilage, chondroitin-6-sulfate predominates over chondroitin-4-sulfate. The two isomers have subtly different binding properties and the ratio shifts with age and disease.
Chondroitin sulfate chains are covalently attached to the aggrecan core protein to form proteoglycan aggregates that bind via link protein to hyaluronic acid, creating massive supramolecular complexes that can reach 200 million daltons in molecular weight. The high density of negatively charged sulfate groups attracts cations and water molecules through the Donnan effect, generating osmotic swelling pressures of several atmospheres — constrained only by the type II collagen fiber network that gives the cartilage its tensile strength.
This swelling-pressure-versus-tensile-mesh design is what gives cartilage its remarkable mechanical properties: high compressive stiffness combined with low friction. When joints are loaded, water is squeezed out of the matrix and the swelling pressure rises until it matches the applied load. When loading is removed, water flows back in. The cycle of water flux is what nourishes chondrocytes (since cartilage has no blood supply) and what keeps the articular surface lubricated. Loss of sulfation reduces swelling pressure, increases compressive deformation, and impairs the water-cycling that maintains tissue health.
Sulfation patterns change in osteoarthritic cartilage: the ratio of 4-sulfated to 6-sulfated chondroitin shifts, chain length shortens, and total sulfate content per disaccharide drops. These changes compromise water binding, mechanical resilience, and the chondrocyte microenvironment.
Cartilage Maintenance and Chondrocyte Biology
Cartilage matrix is in a state of continuous turnover. Healthy chondrocytes synthesize aggrecan and type II collagen, secrete them into the extracellular space, and slowly replace older matrix — the half-life of aggrecan in healthy cartilage is approximately 3 years, type II collagen about 100 years. Osteoarthritis represents a derangement of this homeostasis: matrix-degrading enzymes (aggrecanases, MMPs) exceed matrix-synthesizing capacity, and the net result is progressive loss of tissue.
- Anabolic stimulation — glucosamine sulfate and chondroitin sulfate stimulate chondrocyte expression of type II collagen and aggrecan, the two primary structural macromolecules of hyaline cartilage. In vitro and in vivo studies show increased glycosaminoglycan synthesis when chondrocytes are exposed to these compounds at concentrations achievable with oral supplementation.
- Catabolic suppression — sulfur-containing joint supplements inhibit aggrecanases (ADAMTS-4, ADAMTS-5) and matrix metalloproteinases (MMP-1, MMP-3, MMP-13), the enzymes that drive matrix degradation in osteoarthritis.
- Chondrocyte apoptosis prevention — sulfur-derived glutathione protects chondrocytes from oxidative-stress-induced apoptosis, preserving the cellular population responsible for matrix maintenance.
- Autophagy regulation — emerging research suggests sulfur compounds support chondrocyte autophagy, the cellular housekeeping process that removes damaged organelles and maintains cell viability under the mechanical and oxidative stress of joint loading.
- Subchondral bone coupling — cartilage health is mechanically and biochemically coupled to the underlying subchondral bone; sulfur nutrition supports both tissues simultaneously, maintaining the integrity of the osteochondral unit as a whole.
Anti-Inflammatory Mechanisms
The pain and progression of osteoarthritis are driven less by mechanical wear than by the inflammatory milieu within the joint. Synovial fibroblasts, macrophages, and chondrocytes themselves release pro-inflammatory cytokines (IL-1beta, TNF-alpha) that activate destructive enzymes and sensitize peripheral pain nerves. Sulfur-based interventions attack this milieu through multiple convergent pathways.
- NF-kB pathway inhibition — both MSM and chondroitin sulfate independently inhibit the NF-kB inflammatory signaling pathway, reducing the transcription of genes encoding inflammatory cytokines, chemokines, and destructive enzymes in joint tissues.
- Prostaglandin E2 reduction — sulfur compounds decrease the production of PGE2 by suppressing COX-2 expression in synovial fibroblasts and chondrocytes, reducing pain and inflammatory vasodilation in affected joints.
- Nitric oxide suppression — MSM and glucosamine sulfate reduce iNOS expression, lowering nitric oxide production that at excessive levels contributes to chondrocyte apoptosis and cartilage matrix degradation.
- Complement system modulation — chondroitin sulfate has been shown to inhibit components of the complement cascade within joint tissues, reducing complement-mediated inflammation and tissue damage in inflammatory arthropathies.
- Macrophage polarization — sulfur compounds may promote the shift of synovial macrophages from the pro-inflammatory M1 phenotype toward the anti-inflammatory, tissue-reparative M2 phenotype, supporting resolution of joint inflammation rather than chronic perpetuation.
The clinical translation is that sulfur-based supplements reduce pain through an inflammation-modulating rather than purely analgesic mechanism — which is why effects build over weeks rather than appearing within hours like NSAIDs, and why benefits often persist for weeks after discontinuation rather than washing out within a day.
Glucosamine Sulfate
Glucosamine is an amino sugar (2-amino-2-deoxy-D-glucose) and a building block of chondroitin, keratan, and heparan sulfate chains. As a supplement, the sulfate form (typically crystalline glucosamine sulfate stabilized as the potassium chloride double salt) is consistently more effective in clinical trials than the hydrochloride form — suggesting the sulfate moiety itself contributes to therapeutic benefit, not just the glucosamine backbone.
- Substrate provision — glucosamine sulfate provides both the glucosamine backbone for glycosaminoglycan chain elongation and the sulfate group required for sulfation of chondroitin, keratan, and heparan sulfate in cartilage. It is a direct biochemical substrate for matrix synthesis.
- Hexosamine biosynthetic pathway — glucosamine enters the hexosamine pathway, where it is converted to UDP-N-acetylglucosamine, the activated sugar nucleotide used for glycosaminoglycan and glycoprotein synthesis throughout the body.
- PAPS generation — the sulfate component contributes to the pool of 3'-phosphoadenosine-5'-phosphosulfate, the universal sulfate donor for sulfation reactions including glycosaminoglycan sulfation in cartilage.
- Structure-modifying effects — the landmark long-term studies (Reginster et al. 2001, Pavelka et al. 2002) with crystalline glucosamine sulfate at 1500 mg/day for 3 years demonstrated reduced joint-space narrowing on radiographic assessment, indicating a true disease-modifying effect beyond symptomatic relief. This places crystalline glucosamine sulfate in a different therapeutic category from most over-the-counter joint products.
- Crystalline form superiority — the European EMA recognizes prescription crystalline glucosamine sulfate (Rotta Pharm's "Dona" formulation) as a symptomatic slow-acting drug for osteoarthritis (SYSADOA). US over-the-counter products vary widely in bioavailability and clinical evidence.
Clinical Evidence for Osteoarthritis
The evidence base for sulfur-based joint supplements is substantial but not without controversy — results vary by product formulation, study quality, OA severity, and outcome measure. The pattern across well-designed trials is consistent: moderate symptomatic benefit, possible structural benefit with crystalline glucosamine sulfate over 3 years, excellent safety.
- Crystalline glucosamine sulfate (Reginster 2001 Lancet, Pavelka 2002 Arch Intern Med) — two 3-year double-blind RCTs in knee osteoarthritis, total ~400 patients. Both showed significantly reduced joint-space narrowing versus placebo (-0.06 to -0.31 mm difference at 3 years), plus pain and function improvements. This is the strongest structural-modification evidence for any oral OA intervention.
- Chondroitin sulfate (Kahan 2009, Reginster 2017) — the STOPP and CONCEPT trials at 800 mg/day showed symptomatic benefit comparable to celecoxib at 200 mg/day in knee OA, with structural benefit on MRI cartilage volume.
- GAIT trial (Clegg 2006 NEJM) — the largest US trial, 1,583 patients, glucosamine HCl + chondroitin sulfate. Negative overall, but a subgroup with moderate-to-severe baseline pain showed significant benefit from the combination versus placebo. The HCl form may explain weaker overall results compared to European crystalline-sulfate trials.
- MSM (Kim 2006, Debbi 2011, Brien 2011 meta-analysis) — multiple 12-week RCTs at 1.5-6 g/day show significant WOMAC pain and function improvement versus placebo, with additional benefit when combined with glucosamine.
- Combination products — glucosamine + chondroitin + MSM combination products (often plus type II collagen, hyaluronic acid) show additive benefit in some trials, though component-level evidence is the rigorous standard.
- Long-term safety — 3-year safety data from the Reginster and Pavelka trials, plus post-marketing surveillance, confirm safety comparable to placebo with no signal for cardiovascular, renal, hepatic, or hematologic toxicity at recommended doses.
For the broader inflammatory and degenerative context, see our Arthritis page and Joint Pain page.
Collagen Cross-Linking and Tendon/Ligament Strength
Cartilage is the most sulfur-dependent connective tissue, but tendons, ligaments, fascia, skin, and bone all rely on sulfur for structural integrity through a different mechanism: disulfide bonds in collagen-associated proteins and cysteine residues in elastin and fibrillin.
- Disulfide bond formation — sulfur-containing cysteine residues in collagen-associated proteins (such as the C-terminal propeptides of procollagen) form disulfide bonds that stabilize the procollagen triple helix during biosynthesis and contribute to the supramolecular organization of mature collagen fibrils in cartilage, tendons, and ligaments.
- Lysyl oxidase context — while the cross-linking enzyme lysyl oxidase is itself copper-dependent (not sulfur), the overall cross-linking environment depends on adequate sulfur for the synthesis of collagen and elastin substrates that undergo cross-linking. Sulfur and copper work in concert in connective tissue maintenance — see our Copper page.
- Type II collagen integrity — the primary collagen of articular cartilage (type II) requires sulfur-dependent post-translational modifications and interactions with sulfated proteoglycans for proper fibril organization and mechanical function.
- Tendon and ligament tensile strength — sulfur supports the collagen cross-linking density in tendons and ligaments, maintaining their resistance to tensile forces and reducing susceptibility to injury during physical activity. Athletes with marginal protein intake (and therefore marginal sulfur amino acid intake) show measurably higher rates of tendon and ligament injury.
- Age-related cross-linking changes — collagen cross-linking patterns change with aging, with increased non-enzymatic glycation cross-links (which stiffen tissue pathologically) and altered sulfation patterns. Maintaining adequate sulfur intake may help preserve the enzymatic cross-linking balance that supports tissue elasticity and function.
Dosing and Dietary Sources
- Crystalline glucosamine sulfate — 1500 mg/day, taken once daily or split. The single-daily-dose protocol used in Reginster 2001 is the regimen with the structural-modification evidence.
- Chondroitin sulfate — 800-1200 mg/day, often combined with glucosamine. Higher doses do not appear to add benefit.
- MSM — typical therapeutic dose 1.5-3 g twice daily; upper range 6 g/day in clinical trials. Start at 1.5 g/day and titrate to assess tolerance.
- Dietary sulfur amino acids — cysteine and methionine provide most dietary sulfur. Adequate protein intake (0.8-1.2 g/kg/day) typically supplies enough; elderly patients with reduced protein intake may benefit from targeted supplementation.
- Sulfur-rich whole foods — eggs (the richest single source), garlic, onions, leeks, shallots, cruciferous vegetables (broccoli, cabbage, Brussels sprouts, kale, cauliflower, watercress), meat, fish, legumes. For more, see our Eggs page and Broccoli page.
- NAC and methionine adjuncts — for patients with limited dietary protein, N-acetylcysteine (NAC) at 600-1200 mg/day provides additional sulfur and supports glutathione synthesis simultaneously.
- Onset of effect — 4-12 weeks for symptomatic OA benefit; full structural effects of glucosamine sulfate take 2-3 years of consistent daily use.
Safety and Cautions
- MSM — GRAS status; very low toxicity. Occasional mild GI upset, headache, or insomnia; take with food and avoid late-day dosing if sleep is affected.
- Glucosamine shellfish source — most commercial glucosamine is derived from crab and shrimp shells. Patients with severe shellfish allergy should use vegan fermented glucosamine alternatives (derived from Aspergillus niger or corn fermentation). The allergen itself is in shellfish flesh, not shell, so the actual cross-reactivity risk is low — but allergists generally recommend the vegan source for caution.
- Diabetes and insulin resistance — early concerns about glucosamine worsening insulin resistance (raised by an animal study in the 1990s) have not been confirmed in well-designed human trials. Periodic glucose monitoring is reasonable for diabetic patients starting glucosamine, but the supplement is not contraindicated.
- Anticoagulant interaction — chondroitin sulfate is structurally related to heparin. Case reports describe INR elevation in patients taking warfarin who added chondroitin. Monitor INR weekly for the first month when starting chondroitin in any warfarin-treated patient.
- Sulfite sensitivity confusion — some patients with sulfite sensitivity (from wine, dried fruit) worry about sulfur supplements. The two are biochemically unrelated: sulfite-sensitive reactions involve free SO2, not organic sulfur compounds. MSM, glucosamine sulfate, and chondroitin sulfate are safe for sulfite-sensitive patients.
- Chronic high-dose sulfur amino acids — excess methionine intake (from very high-dose protein powders) may raise homocysteine. Balance with adequate folate, B6, and B12 — see our Homocysteine page.
- CBS upregulation and sulfur intolerance — a small subset of patients with cystathionine beta-synthase (CBS) genetic variants report symptoms of "sulfur intolerance" (sulfur smell, brain fog, fatigue) with high-sulfur diets or MSM supplementation. The mechanism is debated; pragmatic management is to reduce dose and titrate slowly.
- Pregnancy — clinical safety data for MSM, glucosamine, and chondroitin in pregnancy are limited; avoid unless the benefit clearly outweighs the unknown risk.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting sulfur-based joint supplements.
Key Research Papers
- Reginster JY, Deroisy R, Rovati LC, et al. (2001). Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. The Lancet. — PubMed
- Pavelka K, Gatterova J, Olejarova M, et al. (2002). Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Archives of Internal Medicine. — PubMed
- Clegg DO, Reda DJ, Harris CL, et al. (2006). Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis (GAIT). NEJM. — PubMed
- Kim LS, Axelrod LJ, Howard P, et al. (2006). Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: a pilot clinical trial. Osteoarthritis and Cartilage. — PubMed
- Debbi EM, Agar G, Fichman G, et al. (2011). Efficacy of methylsulfonylmethane supplementation on osteoarthritis of the knee: a randomized controlled study. BMC Complementary and Alternative Medicine. — PubMed
- Brien S, Prescott P, Lewith G. (2011). Meta-analysis of the related nutritional supplements dimethyl sulfoxide and methylsulfonylmethane in the treatment of osteoarthritis of the knee. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Kahan A, Uebelhart D, De Vathaire F, et al. (2009). Long-term effects of chondroitins 4 and 6 sulfate on knee osteoarthritis: the study on osteoarthritis progression prevention (STOPP). Arthritis & Rheumatism. — PubMed
- Reginster JY, Dudler J, Blicharski T, Pavelka K. (2017). Pharmaceutical-grade Chondroitin sulfate is as effective as celecoxib and superior to placebo in symptomatic knee osteoarthritis (CONCEPT). Annals of the Rheumatic Diseases. — PubMed
- Butawan M, Benjamin RL, Bloomer RJ. (2017). Methylsulfonylmethane: applications and safety of a novel dietary supplement. Nutrients. — PubMed
- Towheed TE, Maxwell L, Anastassiades TP, et al. (2005). Glucosamine therapy for treating osteoarthritis. Cochrane Database of Systematic Reviews. — PubMed
- Singh JA, Noorbaloochi S, MacDonald R, Maxwell LJ. (2015). Chondroitin for osteoarthritis. Cochrane Database of Systematic Reviews. — PubMed
- Henrotin Y, Mathy M, Sanchez C, Lambert C. (2010). Chondroitin sulfate in the treatment of osteoarthritis: from in vitro studies to clinical recommendations. Therapeutic Advances in Musculoskeletal Disease. — PubMed
PubMed Topic Searches
- PubMed: MSM osteoarthritis randomized
- PubMed: Glucosamine sulfate joint-space narrowing
- PubMed: Chondroitin sulfate cartilage aggrecan
- PubMed: PAPS sulfation glycosaminoglycan
- PubMed: MMP osteoarthritis MSM
Connections
- Sulfur (Main Page)
- Sulfur Benefits Hub
- Sulfur for Glutathione & Methylation
- Sulfur for Skin Health
- Sulfur for Detoxification
- Arthritis
- Joint Pain
- Cysteine
- Methionine
- NAC
- Glutathione
- Copper
- Magnesium
- Silicon
- Manganese
- Collagen
- Eggs
- Broccoli
- All Minerals