Magnesium Test: Serum and RBC Magnesium

Magnesium is the fourth most abundant mineral in the human body and a cofactor in over 300 enzymatic reactions, including ATP synthesis, DNA replication, protein synthesis, nerve impulse transmission, and muscle contraction. Despite its central importance, magnesium deficiency is among the most underdiagnosed mineral deficiencies in clinical medicine — largely because the standard serum magnesium test is a poor reflection of total body magnesium stores.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →Table of Contents
- Overview
- When Ordered
- Reference Ranges
- Serum Magnesium
- RBC Magnesium
- Why Serum Magnesium Is Misleading
- Deficiency Symptoms
- Causes of Deficiency
- Food Sources
- Supplementation Forms
- Research Papers and References
- Connections
- Featured Videos
Overview
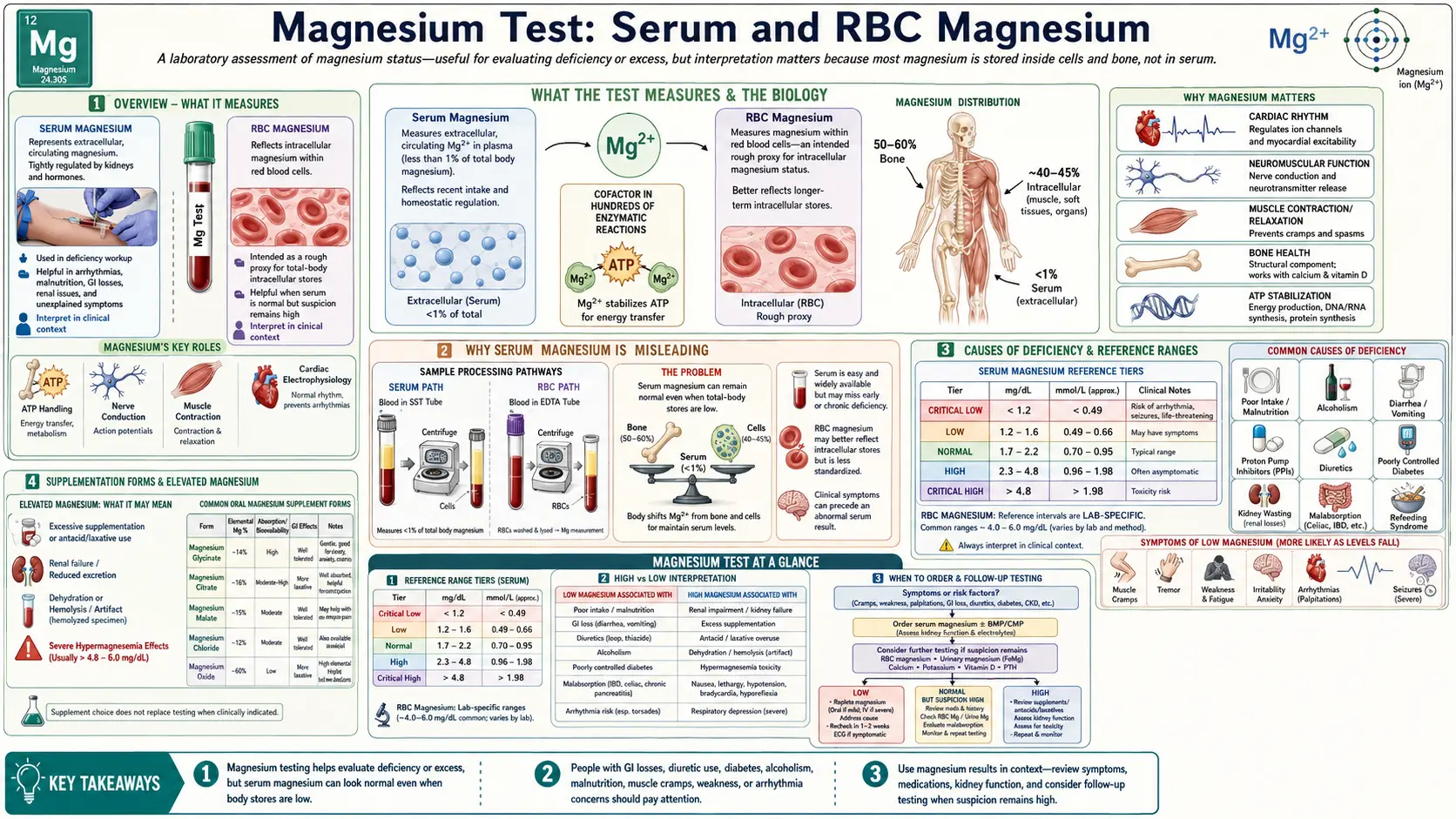
The total body magnesium content in an average adult is approximately 25 grams. This is distributed across three major compartments:
- Bone: ~60% — the largest reservoir, storing magnesium in the hydroxyapatite crystal lattice. Bone magnesium is released slowly and serves as a long-term buffer.
- Intracellular (primarily muscle): ~39% — the metabolically active pool. Intracellular magnesium stabilizes ATP, activates kinases, and is required for all reactions involving ATP hydrolysis.
- Extracellular (serum): ~1% — the fraction measured by standard laboratory tests. Of the serum fraction, approximately 55% is ionized (biologically active), 30% is bound to albumin, and 15% is complexed with phosphate, citrate, and bicarbonate.
The body maintains serum magnesium within a narrow range through renal regulation. When magnesium intake decreases, the kidneys initially conserve magnesium aggressively by reducing urinary excretion. During this conservation phase, serum magnesium remains normal even as intracellular and bone stores are being depleted. By the time serum magnesium falls below the normal range, total body magnesium depletion is already advanced.
Magnesium is essential for:
- All reactions requiring ATP (cellular energy metabolism)
- DNA and RNA synthesis and repair
- Protein synthesis (ribosome function)
- Regulation of calcium channels (antagonizes calcium entry into cells)
- Sodium-potassium ATPase pump function (intracellular potassium maintenance)
- Insulin receptor signaling and glucose transport
- Parathyroid hormone secretion and bone metabolism
- Neuromuscular transmission and cardiac electrical conduction
When Ordered
Magnesium testing is ordered in the following situations:
- Unexplained hypokalemia or hypocalcemia — magnesium deficiency impairs renal potassium conservation and PTH secretion; hypomagnesemia is often the hidden cause of refractory electrolyte abnormalities
- Cardiac arrhythmias — especially torsades de pointes, ventricular tachycardia, or atrial fibrillation unresponsive to standard treatment; magnesium stabilizes cardiac membranes
- Seizures — eclampsia (preeclampsia/eclampsia) is treated with IV magnesium sulfate; magnesium status is also relevant in epilepsy management
- Neuromuscular symptoms — muscle cramps, fasciculations, tetany, tremors, or weakness without clear cause
- Diabetes mellitus — magnesium deficiency is more common in diabetic patients and worsens insulin resistance; monitoring is important in type 2 diabetes
- Alcoholism — alcohol increases urinary magnesium excretion and impairs intestinal absorption
- Malabsorption syndromes — Crohn's disease, celiac disease, short bowel syndrome
- Long-term diuretic use — loop diuretics (furosemide) and thiazides increase urinary magnesium wasting
- PPI use — proton pump inhibitors can cause severe hypomagnesemia via impaired intestinal absorption (FDA warning issued in 2011)
- Critical illness monitoring — ICU patients frequently develop hypomagnesemia from reduced intake, medications, and increased losses
- Migraine evaluation — magnesium deficiency is a recognized trigger and magnesium infusion is used as acute and preventive treatment
- Fatigue, anxiety, or insomnia — functional practitioners often screen for magnesium as part of an integrative workup
Reference Ranges
Serum Magnesium
The standard serum magnesium test measures total magnesium in the extracellular fluid, representing approximately 1% of total body magnesium. It is the most common test ordered for magnesium status and is included in most comprehensive metabolic panels. Despite its widespread use, serum magnesium can be normal even when intracellular depletion is significant.
Serum Magnesium (mg/dL)
Hypomagnesemia (<1.7 mg/dL): Clinically significant symptoms typically appear below 1.2 mg/dL. Levels below 0.8 mg/dL are associated with severe neuromuscular and cardiac manifestations. Hypomagnesemia should prompt evaluation for the underlying cause and simultaneous measurement of serum potassium and calcium (both are frequently co-depleted).
Hypermagnesemia (>2.2 mg/dL): Occurs almost exclusively in patients with renal failure (impaired excretion) or in those receiving excessive magnesium supplementation or IV magnesium therapy. Mild hypermagnesemia is usually asymptomatic. Levels above 4.0 mg/dL cause hypotension, loss of deep tendon reflexes, and respiratory depression. Levels above 6.0 mg/dL can cause cardiac arrest.
RBC Magnesium
The red blood cell (RBC) magnesium test measures the intracellular magnesium concentration within erythrocytes. Because RBCs accumulate magnesium intracellularly over their 120-day lifespan, the RBC magnesium level provides a longer-term, more representative measure of cellular magnesium status than serum levels. It is analogous in concept to hemoglobin A1c as a longer-term marker compared to fasting glucose.
RBC Magnesium (mg/dL)
Clinical notes: RBC magnesium is the preferred test among integrative and functional medicine practitioners because it detects intracellular depletion that serum testing misses. Studies have found that patients with normal serum magnesium but low RBC magnesium have higher rates of hypertension, insulin resistance, cardiovascular disease, and migraine. The test requires a whole blood sample collected in an EDTA tube; the RBCs are separated and lysed before measurement. RBC magnesium is not yet universally available in all clinical laboratories but is offered by major reference laboratories. The level rises gradually with consistent supplementation over 3–4 months, reflecting the 120-day RBC lifespan.
Why Serum Magnesium Is Misleading
The fundamental limitation of serum magnesium as a diagnostic test is a direct consequence of magnesium physiology. Understanding this limitation is essential for clinicians and patients alike.
The 1% Problem
Only approximately 1% of total body magnesium resides in the blood. The remaining 99% is stored in bone (60%) and inside cells, primarily muscle (39%). The serum concentration represents a tightly regulated extracellular pool that is maintained by the kidneys at the expense of intracellular and bone stores. This regulatory system means that serum magnesium is the last compartment to become depleted — not the first.
The Conservation Lag
When dietary magnesium intake falls, the kidneys respond by dramatically increasing tubular magnesium reabsorption, reducing urinary magnesium excretion from a baseline of 100–200 mg/day down to as little as 0.5–1 mg/day. This renal conservation maintains serum magnesium in the normal range for weeks to months while intracellular stores are being progressively depleted. A patient can lose 20–30% of total body magnesium stores before the serum level falls detectably below the normal reference range.
Clinical Implications
Studies using magnesium loading tests (measuring 24-hour urinary retention of a standardized IV magnesium dose) have found that 20–40% of patients with normal serum magnesium have actual total body magnesium deficiency. Because the magnesium loading test is cumbersome and not practical in routine clinical settings, RBC magnesium is the best widely available alternative for assessing functional magnesium status.
The clinical consequence of relying solely on serum magnesium is that symptomatic patients with genuine deficiency are routinely told their magnesium is "normal" and denied treatment — sometimes for years. In conditions such as hypertension, type 2 diabetes, atrial fibrillation, migraine, anxiety, and chronic fatigue, undetected magnesium deficiency may be contributing to disease severity and treatment resistance.
Deficiency Symptoms
Magnesium deficiency produces a broad spectrum of symptoms, reflecting its role as a cofactor in hundreds of enzymatic reactions throughout the body:
Neuromuscular
- Muscle cramps — especially nocturnal leg cramps; magnesium deficiency causes hyperexcitability of the neuromuscular junction
- Muscle weakness and fatigue — impaired ATP production affects all muscle function
- Tremors and fasciculations — fine muscle twitching, most commonly of the eyelids (myokymia)
- Tetany — spontaneous, painful muscle spasms; Chvostek's sign (facial muscle twitch on tapping) and Trousseau's sign (carpal spasm with blood pressure cuff) may be positive
- Numbness and paresthesias — tingling in extremities
Cardiovascular
- Hypertension — magnesium acts as a natural calcium channel blocker; deficiency promotes vasoconstriction
- Cardiac arrhythmias — ventricular premature contractions, torsades de pointes (associated with prolonged QT interval), atrial fibrillation
- Coronary artery spasm — magnesium deficiency increases coronary vasomotor tone
- Increased platelet aggregation — promoting thrombosis risk
Neurological and Psychiatric
- Anxiety and nervousness — magnesium modulates the NMDA glutamate receptor; deficiency increases excitatory neurotransmission
- Insomnia — magnesium promotes GABA activity and melatonin synthesis
- Depression — multiple studies link low magnesium to depressive symptoms
- Migraine headaches — intracellular magnesium depletion triggers cortical spreading depression and neurogenic inflammation
- Cognitive impairment — impaired synaptic plasticity and memory consolidation
Metabolic
- Insulin resistance and type 2 diabetes — magnesium is required for insulin receptor tyrosine kinase activity and glucose transporter (GLUT4) translocation
- Refractory hypokalemia — magnesium is essential for the renal Na-K-ATPase that maintains intracellular potassium; without adequate magnesium, potassium wasting cannot be corrected
- Hypocalcemia — severe magnesium deficiency impairs PTH secretion and end-organ PTH responsiveness, causing secondary hypocalcemia that is refractory to calcium supplementation alone
- Osteoporosis — magnesium is a structural component of bone mineral and regulates osteoblast and osteoclast function
Causes of Deficiency
Inadequate Dietary Intake
The average American diet provides approximately 250 mg of magnesium per day — well below the RDA of 310–420 mg for adults. Surveys consistently show that 45–60% of Americans do not meet the EAR (estimated average requirement) for magnesium. The primary driver is the displacement of magnesium-rich whole foods by refined grains, processed foods, and sugar, which contain little to no magnesium. Refining wheat flour removes approximately 80% of its magnesium content.
Gastrointestinal Losses
- Chronic diarrhea — inflammatory bowel disease, irritable bowel syndrome, infections, laxative overuse
- Malabsorption syndromes — celiac disease, Crohn's disease, short bowel syndrome, tropical sprue
- Vomiting — reduces intake and causes gastric magnesium losses
- Proton pump inhibitors (PPIs) — impair active magnesium transport in the intestine; the FDA issued a safety warning in 2011 regarding PPI-induced hypomagnesemia
Renal Wasting
- Loop diuretics (furosemide, bumetanide, torsemide) — inhibit the NKCC2 transporter in the thick ascending limb, the primary site of renal magnesium reabsorption
- Thiazide diuretics — cause milder but chronic magnesium wasting through distal tubule effects
- Diabetes — osmotic diuresis from hyperglycemia increases urinary magnesium excretion; insulin resistance also impairs intracellular magnesium accumulation
- Alcohol — directly inhibits tubular magnesium reabsorption; alcoholism is the most common cause of symptomatic hypomagnesemia in hospitalized patients
- Medications — aminoglycosides, amphotericin B, cisplatin, cyclosporine, tacrolimus, and certain antivirals (foscarnet) cause renal magnesium wasting
- Genetic tubulopathies — Gitelman syndrome, Bartter syndrome, EAST syndrome
Other Causes
- Type 2 diabetes — reciprocal relationship: low magnesium worsens insulin resistance; hyperglycemia causes magnesium wasting
- Chronic stress — cortisol and catecholamines mobilize intracellular magnesium and increase urinary excretion; stress depletes magnesium, and low magnesium amplifies the stress response
- Excessive sweating — significant magnesium is lost in sweat during intense exercise or heat exposure
- Excessive calcium or vitamin D supplementation — high calcium-to-magnesium ratios can competitively impair magnesium absorption and utilization
- Metabolic alkalosis — reduces tubular magnesium reabsorption
Food Sources
Magnesium is found predominantly in plant foods, particularly those rich in chlorophyll (magnesium is the central atom of the chlorophyll molecule). The best dietary sources include:
- Nuts and seeds: Pumpkin seeds (156 mg/oz), almonds (80 mg/oz), cashews (74 mg/oz), Brazil nuts (64 mg/oz), sunflower seeds (37 mg/oz)
- Legumes: Black beans (60 mg/½ cup), edamame (50 mg/½ cup), kidney beans (35 mg/½ cup), lentils (36 mg/½ cup)
- Whole grains: Quinoa (118 mg/cup cooked), oat bran (96 mg/cup), brown rice (84 mg/cup), whole wheat bread (46 mg/2 slices)
- Leafy greens: Spinach (157 mg/cup cooked), Swiss chard (150 mg/cup), beet greens (98 mg/cup), kale (36 mg/cup)
- Dark chocolate: 70–85% cocoa solids provide 64 mg/oz and are among the richest dietary magnesium sources
- Avocado: 58 mg per medium avocado
- Banana: 32 mg per medium banana
- Fatty fish: Mackerel (82 mg/3 oz), salmon (26 mg/3 oz)
- Hard water: In areas with magnesium-rich groundwater, drinking water can contribute 10–50 mg/day
Notably, the magnesium content of many crops has declined over the past several decades due to depletion of soil magnesium through intensive agriculture and the use of high-phosphate fertilizers that reduce magnesium uptake by plants.
Supplementation Forms
Magnesium supplements differ substantially in their elemental magnesium content, bioavailability, and clinical applications. Choosing the right form depends on the clinical goal and the patient's tolerance:
Well-Absorbed Forms (High Bioavailability)
- Magnesium glycinate (bisglycinate): Chelated with glycine. High bioavailability, excellent gastrointestinal tolerability, minimal laxative effect. Preferred for correcting deficiency, anxiety, sleep, and muscle cramps. Contains approximately 14% elemental magnesium. Considered the gold standard for oral repletion.
- Magnesium malate: Bound to malic acid. Well absorbed, gentle on the GI tract. Malic acid participates in the Krebs cycle, making this form popular for energy and fibromyalgia. Contains approximately 15% elemental magnesium.
- Magnesium taurate: Bound to taurine. Both magnesium and taurine have cardiovascular benefits (antiarrhythmic, vasodilatory). Used specifically for cardiovascular applications.
- Magnesium L-threonate: The only form shown to cross the blood-brain barrier effectively in animal studies. Used specifically for cognitive function and neurological applications. Lower elemental magnesium content per dose.
- Magnesium citrate: Bound to citric acid. Good bioavailability; has mild laxative effect at higher doses (used medically for bowel preparation). Contains approximately 16% elemental magnesium. Widely available and affordable.
Poorly Absorbed or Specialized Forms
- Magnesium oxide: The most commonly sold form (due to low cost and high elemental content at 60%), but poorly absorbed (approximately 4–5% absorption). Primarily used as a laxative rather than for magnesium repletion. Not recommended for treating deficiency.
- Magnesium sulfate (Epsom salt): Used IV in hospitals for eclampsia, severe asthma, and torsades de pointes. Available as a bath additive; transdermal absorption is minimal and not a reliable route of supplementation. Highly osmotic orally — used as a laxative.
- Magnesium chloride: Moderate absorption; available as topical oil/gel (claimed to be transdermally absorbed, though evidence is limited). Oral form well tolerated in small amounts.
- Magnesium hydroxide (milk of magnesia): Poorly absorbed; used primarily as an antacid and laxative.
Dosing Considerations
The tolerable upper intake level (UL) for supplemental magnesium is 350 mg/day for adults (this limit applies to supplements only, not dietary magnesium). The most common side effect of oral magnesium supplementation is diarrhea, which is dose-dependent and most pronounced with poorly-absorbed forms (oxide, sulfate, hydroxide). Divided doses (two or three times daily) improve absorption and reduce GI side effects compared to a single large dose. Patients with renal impairment must use magnesium supplements with caution due to the risk of accumulation and hypermagnesemia.
For RBC magnesium repletion, consistent supplementation with a well-absorbed form for at least 3–4 months is required before re-testing, reflecting the 120-day lifespan of red blood cells.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for magnesium testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Serum magnesium limitations — PubMed literature search
- RBC magnesium clinical utility — PubMed literature search
- Magnesium deficiency prevalence — PubMed literature search
- Magnesium and cardiovascular disease — PubMed literature search
- Magnesium type 2 diabetes — PubMed literature search
- Magnesium and migraine — PubMed literature search
- Magnesium and sleep — PubMed literature search
- PPI magnesium depletion — PubMed literature search
- Magnesium loading test — PubMed literature search
- Ionized magnesium assay — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Magnesium
- Magnesium Glycinate
- Magnesium Replenishment
- Calcium
- Potassium
- Hypertension
- Atrial Fibrillation
- Migraine
- Anxiety
- Depression
- Insomnia
- Fatigue
- Insulin Resistance
- Crohn's Disease
- Celiac Disease
- Sleep Hygiene
- Magnesium and Heart Health
- Magnesium and Sleep