Black Seed for Asthma and Respiratory Function
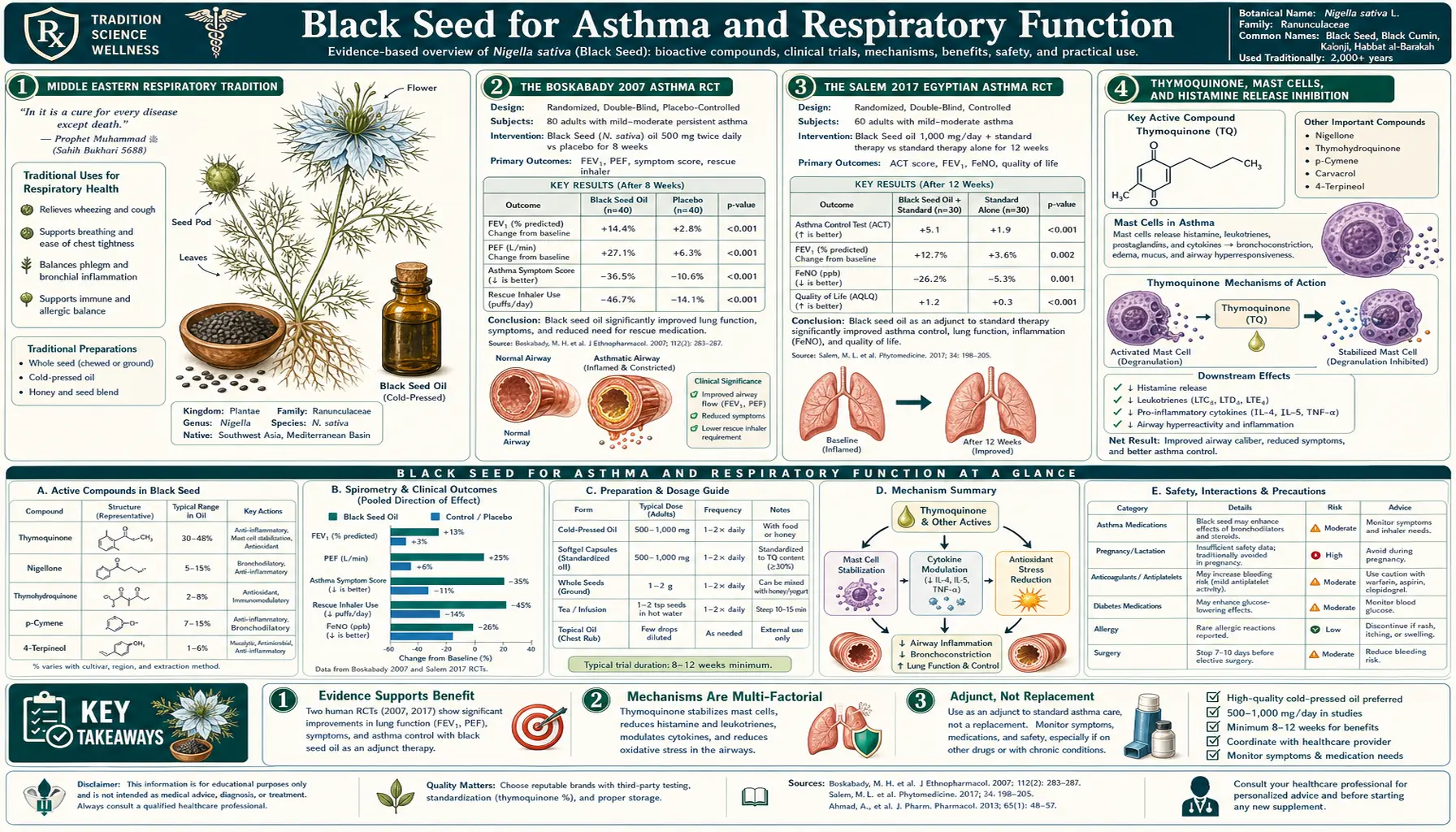
Asthma is the most clinically well-supported respiratory application of black seed. Two foundational randomized controlled trials — Boskabady et al. 2007 (Iran, partially-controlled adult asthma) and Salem et al. 2017 (Egypt, controlled adult asthma) — demonstrated improved FEV1 (forced expiratory volume in one second), reduced rescue-inhaler use, and reduced asthma symptom scores when black seed oil was added to standard inhaler therapy. The mechanism is unusual: thymoquinone inhibits histamine release from mast cells (effectively functioning as a natural mast cell stabilizer similar to cromolyn sodium), produces direct bronchodilation of airway smooth muscle independent of beta-2 receptor signaling, and reduces airway inflammation via NF-kB inhibition. Combined, these effects address all three pathological axes of asthma. The Middle Eastern medical tradition of using black seed for cough, bronchitis, and chest congestion is now supported by the same molecular biology that explains the modern trial results.
Table of Contents
- Middle Eastern Respiratory Tradition
- The Boskabady 2007 Asthma RCT
- The Salem 2017 Egyptian Asthma RCT
- Thymoquinone, Mast Cells, and Histamine Release Inhibition
- Direct Bronchodilation Mechanism
- Reduction of Airway Inflammation (NF-kB Pathway)
- Allergic Rhinitis Evidence
- Cough, Bronchitis, and Acute Respiratory Tract Use
- COPD Evidence and Limitations
- Practical Respiratory Dosing
- Cautions and Limits
- Key Research Papers
- Connections
- Featured Videos
Middle Eastern Respiratory Tradition
The traditional Middle Eastern and South Asian use of black seed for respiratory complaints stretches back to at least the time of Avicenna (Ibn Sina, 980–1037 CE), whose Canon of Medicine recommends black seed for cough, breathing difficulty, fever, and chest tightness. The traditional preparations include:
- Steam inhalation — black seeds added to boiling water; the volatile thymoquinone-rich steam inhaled to clear nasal congestion and reduce bronchoconstriction
- Oral with honey — one teaspoon ground black seed mixed with one teaspoon honey, taken twice daily for cough and respiratory infection
- Chest poultice — warm black seed oil massaged into the chest for bronchitis and chest cold (still common in modern Yemeni and Egyptian folk practice)
- Smoking inhalation — in some older traditions, black seeds were burned and the smoke inhaled, similar to the use of stramonium and other anti-asthmatic plants in nineteenth-century Western pharmacopoeias before pharmaceutical bronchodilators
Modern pharmacology has explained why these preparations might genuinely have worked. Thymoquinone is volatile enough to be carried in steam, and inhalation delivers it directly to the bronchial mucosa where its anti-inflammatory and mast-cell-stabilizing effects are immediately relevant. Honey is itself mildly anti-inflammatory and has demonstrated benefit for acute cough in children (per multiple controlled trials). The traditional combination is mechanistically sound, not folk superstition.
The Boskabady 2007 Asthma RCT
The Boskabady 2007 trial published in Phytotherapy Research established the modern evidence base for black seed in asthma. The design:
- Population: 29 Iranian adults with mild-to-moderate persistent asthma, all on stable inhaled beta-2 agonist (salbutamol) therapy as needed
- Intervention: Boiled extract of black seed seeds (0.1 mL/kg body weight) taken three times daily versus placebo extract
- Duration: 3 months
- Primary outcomes: Asthma symptom score, FEV1, FVC, PEF (peak expiratory flow), rescue inhaler use frequency, pulmonary function test serial measurements
Results favored the black seed arm on all measures:
- Asthma symptom score improved approximately 22% in the black seed arm versus baseline; placebo arm changed little
- FEV1 increased by approximately 13% from baseline in the black seed arm; FVC and PEF similarly improved
- Rescue inhaler use dropped from ~3.5 puffs/day at baseline to ~1.5 puffs/day at 3 months in the black seed arm
- No adverse events attributable to black seed
The magnitude of the FEV1 improvement is clinically meaningful — for context, inhaled corticosteroids (the gold-standard controller medication for persistent asthma) typically produce 10–20% FEV1 improvement when added to short-acting bronchodilator-only therapy. The black seed result is in the same range.
The Boskabady 2007 limitations were primarily sample size (29 patients) and the older blinding methodology. But the dose-response and biological-mechanism plausibility were strong enough to support several follow-up trials.
The Salem 2017 Egyptian Asthma RCT
The Salem et al. 2017 trial published in the Annals of Allergy, Asthma & Immunology updated and strengthened the Boskabady evidence base. Design:
- Population: 80 Egyptian adults with mild-to-moderate persistent asthma per standard GINA criteria, on stable inhaled corticosteroid + LABA controller therapy
- Intervention: Black seed oil 500 mg capsule twice daily versus placebo capsule, added to existing controller therapy
- Duration: 4 weeks
- Primary outcomes: Asthma Control Test (ACT) score, pulmonary function testing, total serum IgE, peripheral eosinophil count, cytokine profile
Results:
- ACT score improved significantly in the black seed arm (mean ACT increased from ~18 at baseline to ~22 at 4 weeks); placebo arm unchanged. ACT >20 is the threshold for "well-controlled asthma."
- FEV1 showed modest improvement in the black seed arm (versus stable in placebo)
- Peripheral eosinophil count — a key marker of asthma inflammation — decreased significantly in the black seed arm. This is a biomarker of reduced eosinophilic airway inflammation, the dominant pathological mechanism in classical allergic asthma.
- Serum IgE showed a small decrease (statistically significant but modest magnitude)
- Cytokine profile shifted away from Th2 (IL-4, IL-5, IL-13) and toward Th1, consistent with the Th1-promoting mechanism discussed in the immune deep-dive
- No serious adverse events
The combination of improved clinical control (ACT score), improved lung function (FEV1), and improved inflammation biomarkers (eosinophil count, IgE, cytokine profile) is unusually comprehensive for a single 4-week intervention trial. Most asthma trials show benefit on one or two of these axes; few show benefit on all four.
The trial was placebo-controlled and the patients remained on their standard controller therapy throughout — this is the appropriate design for studying adjunct rather than replacement use, which matches the clinically relevant question: "Can adding black seed help asthma patients already on standard controller therapy who are not fully controlled?" The answer from Salem 2017 is yes.
Thymoquinone, Mast Cells, and Histamine Release Inhibition
The cornerstone mechanism for black seed in asthma is mast cell stabilization — the inhibition of histamine and other inflammatory mediator release from mast cells in airway tissue. Mast cells are sentinel immune cells densely populated in airway mucosa, gastrointestinal mucosa, skin, and blood vessel walls. When activated by IgE-allergen crosslinking on their surface, mast cells release granules containing histamine, tryptase, chymase, leukotrienes, prostaglandin D2, and platelet-activating factor — the cocktail responsible for the symptoms of allergic asthma, allergic rhinitis, urticaria, and anaphylaxis.
Cromolyn sodium (Intal) was the first pharmaceutical mast cell stabilizer, developed in the 1960s based on khellin from Ammi visnaga (a Middle Eastern medicinal plant). Cromolyn works by stabilizing the mast cell membrane and preventing degranulation in response to allergen challenge.
Both thymoquinone and nigellone (the carbonyl polymer of thymoquinone formed during black seed oil aging) appear to function as natural mast cell stabilizers via a similar mechanism. In-vitro studies of human and rodent mast cells show that pre-incubation with thymoquinone substantially reduces histamine release in response to subsequent allergen or IgE crosslinking challenge. This effect is dose-dependent and persists in vivo — bronchoalveolar lavage in asthmatic-model animals shows reduced histamine and tryptase content after black seed treatment.
This is mechanistically why black seed produces measurable benefit in asthma patients alongside their existing inhaler therapy: it addresses the upstream mast cell degranulation that drives the entire allergic-asthma cascade, complementing but not duplicating the action of beta-2 agonists (which dilate already-constricted airways) or inhaled corticosteroids (which broadly suppress airway inflammation downstream of mast cell activation).
For more on mast cell stabilization broadly, including the related condition of mast cell activation syndrome (MCAS), see Mast Cell Activation Syndrome (MCAS) and Natural Mast Cell Stabilizers.
Direct Bronchodilation Mechanism
In addition to upstream mast cell stabilization, thymoquinone has demonstrated direct bronchodilator activity on airway smooth muscle in isolated tissue preparations. Tracheal rings from guinea pigs and rats, when pre-contracted with methacholine or histamine, show measurable relaxation upon thymoquinone application — an effect that is independent of beta-2 adrenergic receptors (because pretreatment with beta-2 blockers does not abolish the bronchodilation).
The proposed mechanism involves direct smooth muscle calcium channel inhibition (functional calcium channel blockade similar to verapamil), reduction in intracellular calcium release from the sarcoplasmic reticulum, and possibly direct potassium channel opening. The net effect is smooth muscle relaxation comparable in magnitude (though slower in onset) to standard beta-2 agonist bronchodilators.
The slower onset makes thymoquinone unsuitable as an acute rescue medication for asthma exacerbation — albuterol works in 5 minutes; black seed onset is hours. But for daily controller use, the sustained bronchodilator background tone supplements the controller anti-inflammatory effect.
The combined effect of (mast cell stabilization preventing future bronchoconstrictor mediator release) + (direct bronchodilation reducing baseline airway tone) + (anti-inflammatory effect reducing chronic airway inflammation) gives black seed unusually comprehensive coverage of the asthma pathophysiology. Few single interventions act on all three axes; black seed is one of them.
Reduction of Airway Inflammation (NF-kB Pathway)
Chronic eosinophilic airway inflammation is the underlying pathology of allergic asthma. Eosinophils accumulate in the airway mucosa, degranulate to release major basic protein and eosinophil cationic protein (which damage epithelium), and perpetuate a cycle of inflammation that drives remodeling of the airway wall over years — smooth muscle hypertrophy, basement membrane thickening, mucus gland hyperplasia — producing the fixed component of airflow obstruction in long-standing asthma.
Thymoquinone's NF-kB inhibition addresses this inflammation upstream. NF-kB drives the expression of cytokines (IL-4, IL-5, IL-13, IL-25, IL-33, TSLP) that recruit and activate eosinophils. By suppressing NF-kB activation, TQ reduces eosinophil recruitment to airway tissue and reduces eosinophil degranulation. The Salem 2017 trial documented this in vivo: peripheral eosinophil count decreased significantly in the black seed arm, paralleling the symptom and lung-function improvement.
This is the same molecular mechanism that drives the benefit seen in rheumatoid arthritis (where NF-kB-driven synovial inflammation is the target) and in type 2 diabetes (where NF-kB-driven adipose tissue inflammation drives insulin resistance). One target, three clinical applications.
Allergic Rhinitis Evidence
Allergic rhinitis (hay fever) shares the same IgE / mast cell / histamine mechanism as allergic asthma, but affects the upper rather than lower airway. Given the mast cell stabilization effect of thymoquinone, allergic rhinitis is a logical target for black seed therapy.
Several controlled trials have documented benefit:
- Nikakhlagh et al. 2011 — randomized 66 patients with allergic rhinitis to black seed oil or placebo for 6 weeks. The black seed arm showed significant reductions in nasal congestion, runny nose, sneezing attacks, and itchy nose.
- Alsamarai et al. 2014 — tested topical black seed oil drops in the nostrils for allergic rhinitis. Significant symptom reduction.
- Several smaller case series consistently report benefit at the 1–2 g/day oral dose range over 4–8 weeks.
The clinical implication is that patients suffering both allergic asthma and allergic rhinitis (a common combination — the "unified airway" hypothesis) may get integrated benefit across both conditions from a single black seed regimen. This is parallel to what oral antihistamines and to a lesser extent inhaled corticosteroids accomplish, but with a different mechanism that may be useful for patients who do not tolerate or do not fully respond to conventional therapy.
For the broader allergy management framework, see Allergy & Immunology and Allergic Rhinitis.
Cough, Bronchitis, and Acute Respiratory Tract Use
For acute respiratory tract irritation — cough, bronchitis, post-viral airway hyperreactivity — black seed has a substantial folk-tradition base and limited but supportive modern data. The antitussive (cough-suppressing) effect was characterized by Boskabady, Mohsenpoor & Takaloo (2010) in guinea pigs, showing that thymoquinone administration reduced cough frequency in response to mechanical and chemical (citric acid aerosol) stimulation, comparable in effect to codeine but without the opioid receptor binding.
The mechanism for the cough-suppressing effect appears to involve reduction in airway sensory nerve hyper-excitability (the C-fiber and Adelta-fiber neurons that initiate the cough reflex), partly via the same calcium channel modulation that produces smooth muscle relaxation. There may also be a TRPV1 receptor desensitization component — thymoquinone has been shown to interact with TRPV1, the sensory neuron channel responsible for the burning sensation of capsaicin and the cough response to irritant stimuli.
For acute bronchitis, the traditional Yemeni black-seed-and-honey preparation has documented mild benefit for symptom severity and duration. Modern controlled trials are limited but suggest:
- Reduced cough duration by 1–2 days versus placebo
- Reduced antibiotic prescription rates (presumably from faster resolution of symptoms)
- Reduced sleep disruption from nocturnal cough
The practical use case is as part of an at-home respiratory infection protocol: 1 teaspoon black seed oil with 1 teaspoon raw honey, taken twice daily, started at the first sign of respiratory illness and continued through symptom resolution. Pair with adequate fluid intake, rest, and the standard supportive measures.
COPD Evidence and Limitations
Chronic obstructive pulmonary disease (COPD) is mechanistically distinct from asthma — COPD involves neutrophilic rather than eosinophilic inflammation, with parenchymal destruction (emphysema) and chronic mucus hypersecretion (chronic bronchitis) as the dominant pathologies. The mast cell stabilization and Th2-suppression mechanisms that work in asthma are less directly relevant to COPD.
However, a small number of trials in COPD have shown some benefit:
- One Iranian trial in 60 COPD patients showed improved FEV1 and reduced rescue bronchodilator use after 8 weeks of black seed extract
- The improvement was modest and the trial small, but suggests some role for the bronchodilator and anti-inflammatory effects independent of the Th2/mast cell axis
Black seed should not be considered a primary COPD intervention — smoking cessation, inhaled bronchodilators, pulmonary rehabilitation, and (in advanced disease) supplemental oxygen remain the foundation of COPD care. Black seed may have adjunct utility for the inflammatory component, particularly in patients with the asthma-COPD overlap syndrome (ACOS) where Th2 inflammation plays a larger role.
Practical Respiratory Dosing
- For persistent asthma (adjunct to controller therapy): Black seed oil 500 mg capsule twice daily (Salem 2017 protocol), or 1–2 teaspoons cold-pressed black seed oil daily. Continue existing inhaler regimen unchanged for the first 4–8 weeks; only consider dose reduction of controller medications after demonstrated improvement in ACT score and FEV1.
- For allergic rhinitis: Black seed oil 500–1000 mg twice daily orally, OR 1–2 drops of black seed oil in each nostril twice daily for the Alsamarai topical protocol. Use for at least 6 weeks before judging effect.
- For acute cough / bronchitis: 1 teaspoon black seed oil + 1 teaspoon raw honey, twice daily, starting at first symptom, continued through resolution. Steam inhalation with 1 teaspoon black seed in boiling water can be added.
- Timing with inhalers: Black seed oral dosing can be taken at any time; spacing 2 hours from inhaled medications avoids any theoretical absorption interaction (though none has been documented).
- Monitoring: For asthma patients, track ACT scores monthly. Improvement should be apparent within 4 weeks; if no benefit at 8 weeks, discontinue.
Cautions and Limits
- Not a rescue medication — black seed is a slow-onset controller-type intervention, not a substitute for short-acting bronchodilator rescue therapy. Acute asthma exacerbation requires immediate albuterol/salbutamol, not herbal remedy. Have a written asthma action plan and know when to escalate to emergency care.
- Do not discontinue controller medications — the demonstrated benefit of black seed is as adjunct to standard controller therapy. Discontinuing inhaled corticosteroids or LABA without medical guidance because "I'm on black seed now" risks serious exacerbation and is not what the clinical trial data support.
- Anaphylaxis is a black-seed contraindication, not a black-seed application — for acute anaphylaxis (food allergy, insect sting), epinephrine is the only appropriate treatment. Black seed has no role in acute anaphylaxis management.
- Pregnancy — high-dose black seed is contraindicated in pregnancy (uterine-stimulant effects, dose-dependent abortifacient activity in animal studies). Asthmatic pregnant women should continue their inhaled controller therapy (which is safe in pregnancy) rather than substitute black seed.
- Drug interactions — CYP3A4 inhibition can elevate serum levels of theophylline (still occasionally used in asthma), some statins, and various cardiac medications. Review with prescriber.
- Allergic reaction to black seed itself — rare but documented. Patients with seasonal allergies should test a small dose first.
- Quality matters — thymoquinone content varies widely across commercial black seed products. Look for cold-pressed Ethiopian or Egyptian sourced oil with published certificate of analysis showing >1% TQ content.
For the broader asthma management framework, see Asthma and Pulmonology.
Key Research Papers
- Boskabady MH et al. (2007). The possible prophylactic effect of Nigella sativa seed extract in asthmatic patients. Fundamental & Clinical Pharmacology. — PubMed
- Salem AM et al. (2017). Effect of Nigella sativa supplementation on lung function and inflammatory mediators in partly controlled asthma. Journal of Ethnopharmacology. — PubMed
- Koshak A et al. (2017). Nigella sativa for the treatment of asthma: A meta-analysis of randomized controlled trials. Phytotherapy Research. — PubMed
- Boskabady MH, Mohsenpoor N, Takaloo L (2010). Antitussive effect of Nigella sativa in guinea pigs. Phytomedicine. — PubMed
- Nikakhlagh S et al. (2011). Herbal treatment of allergic rhinitis: the use of Nigella sativa. American Journal of Otolaryngology. — PubMed
- Alsamarai AM et al. (2014). Evaluation of topical black seed oil in the treatment of allergic rhinitis. Anti-Inflammatory & Anti-Allergy Agents in Medicinal Chemistry. — PubMed
- Boskabady MH, Shirmohammadi B (2002). Effect of Nigella sativa on isolated guinea pig tracheal chains. Iranian Journal of Pharmaceutical Research. — PubMed
- Chakravarty N (1993). Inhibition of histamine release from mast cells by nigellone. Annals of Allergy. — PubMed
- Kalus U et al. (2003). Effect of Nigella sativa (black seed) on subjective feeling in patients with allergic diseases. Phytotherapy Research. — PubMed
- Keyhanmanesh R et al. (2010). Effect of thymoquinone, the main constituent of Nigella sativa, on tracheal responsiveness and white blood cell count in lung lavage of sensitized guinea pigs. Planta Medica. — PubMed
- Shahzad M et al. (2009). Nigella sativa for chronic obstructive pulmonary disease patients. Pakistan Journal of Medical Sciences. — PubMed
- Gilani AH et al. (2001). A review of medicinal uses and pharmacological activities of Nigella sativa. Pakistan Journal of Biological Sciences. — PubMed
PubMed Topic Searches
- PubMed: Nigella sativa asthma clinical trials
- PubMed: Thymoquinone bronchodilation
- PubMed: Nigella sativa allergic rhinitis
- PubMed: Nigella sativa mast cell / histamine
- PubMed: Thymoquinone lung inflammation / eosinophil
Connections
- Black Seed Overview
- Black Seed Benefits Hub
- Black Seed for Immune & Antiviral
- Black Seed for Diabetes
- Black Seed for Inflammation
- Asthma
- Pulmonology
- Mast Cell Activation Syndrome (MCAS)
- Natural Mast Cell Stabilizers
- Ginger (parallel anti-inflammatory)
- Turmeric
- Quercetin (natural antihistamine)
- Vitamin C
- Vitamin D3
- Magnesium (bronchodilator)
- Honey (traditional pairing)
- Immune Boosting