Black Seed for Diabetes and Metabolic Syndrome
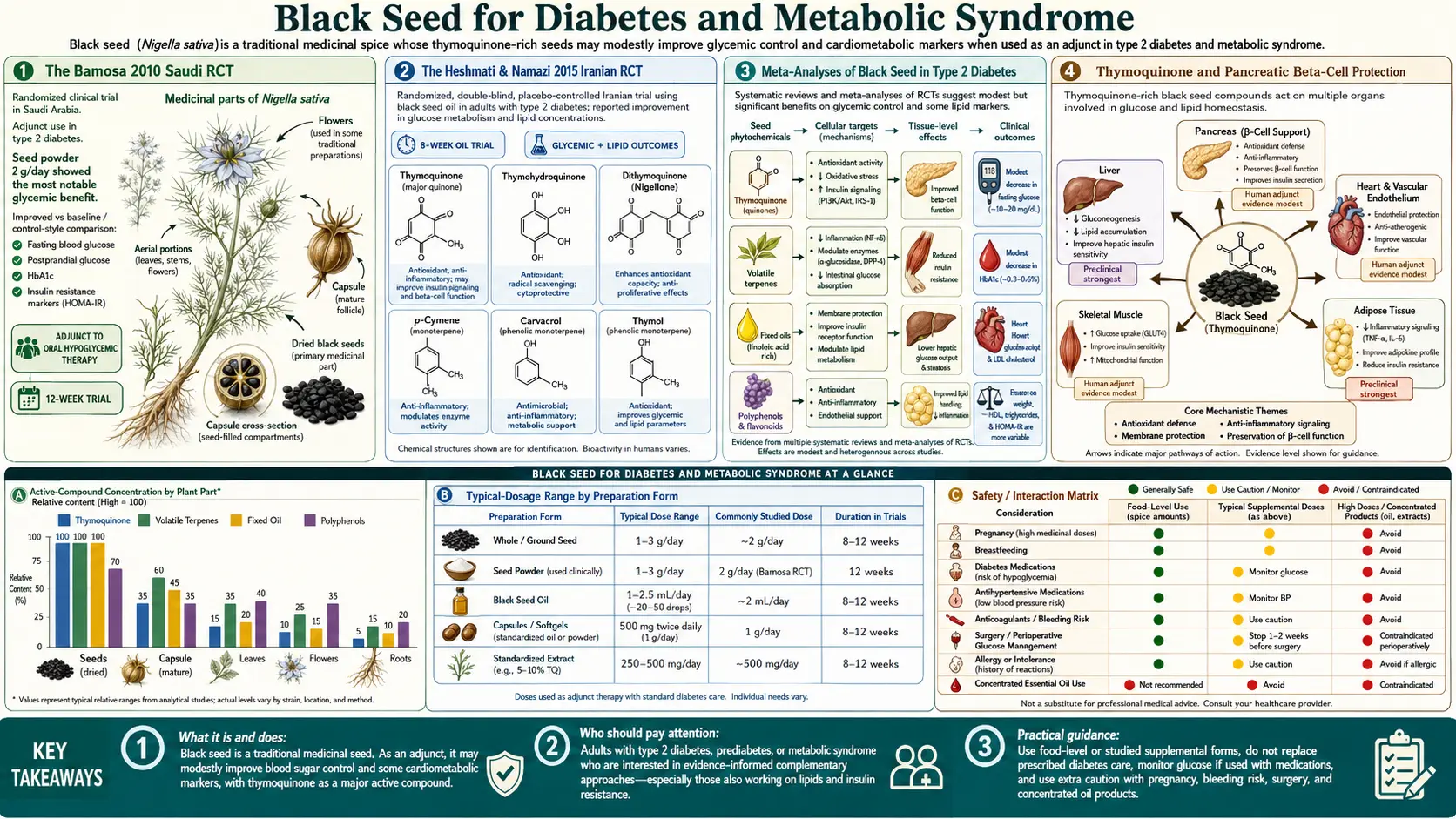
The strongest human evidence for any black seed indication is in type 2 diabetes. Two pivotal randomized controlled trials — Bamosa et al. 2010 (Saudi Arabia, 94 patients) and Heshmati & Namazi 2015 (Iran, 84 patients, expanded design) — demonstrated that 2–3 grams per day of black seed powder over 12 weeks produced HbA1c reductions of approximately 1.0 to 2.0 percentage points, comparable to a moderate dose of metformin (500–1000 mg twice daily). The mechanism combines AMPK activation (mimicking metformin), direct protection of pancreatic beta cells against oxidative damage, improved insulin sensitivity at the muscle and liver, and reductions in total cholesterol, LDL, and triglycerides. This deep-dive walks through both trials in clinical detail, the molecular mechanism, the practical dosing for diabetic and pre-diabetic patients, and the safety considerations when combining black seed with conventional diabetes medication.
Table of Contents
- The Bamosa 2010 Saudi RCT
- The Heshmati & Namazi 2015 Iranian RCT
- Meta-Analyses of Black Seed in Type 2 Diabetes
- Thymoquinone and Pancreatic Beta-Cell Protection
- AMPK Activation — The Metformin-Like Mechanism
- Insulin Sensitivity at Muscle and Liver
- Lipid Improvements: Cholesterol, LDL, Triglycerides
- Metabolic Syndrome and Weight Trial Evidence
- Practical Dosing for Pre-Diabetes and Type 2 Diabetes
- Drug Interactions and Hypoglycemia Risk
- Key Research Papers
- Connections
- Featured Videos
The Bamosa 2010 Saudi RCT
The Bamosa et al. 2010 trial published in the Indian Journal of Physiology and Pharmacology is the foundational human study for black seed in type 2 diabetes. The trial design:
- Population: 94 Saudi Arabian patients with type 2 diabetes, all on stable oral hypoglycemic therapy (sulfonylurea, biguanide, or both)
- Intervention: Three arms — black seed powder 1 g/day, black seed powder 2 g/day, or black seed powder 3 g/day, added to existing diabetes therapy
- Duration: 12 weeks
- Primary outcome: Fasting plasma glucose, HbA1c, and insulin levels
Results were strikingly dose-dependent. The 1 g/day arm showed minimal change. The 2 g/day arm produced a meaningful HbA1c reduction. The 3 g/day arm produced the largest effect:
- HbA1c reduction: approximately 1.5 percentage points (from ~8.2% to ~6.7%) in the 3 g arm
- Fasting glucose reduction: approximately 45 mg/dL in the 3 g arm
- Insulin resistance (HOMA-IR): significant improvement in the 2 g and 3 g arms
- Adverse events: No clinically significant hypoglycemia, no GI intolerance prompting discontinuation, no hepatic or renal abnormalities on lab monitoring
The 1.5 percentage point HbA1c reduction is comparable to what is achieved by adding metformin (500–1000 mg twice daily) to existing diabetes therapy. For context, the regulatory threshold for a new diabetes drug to be approved by the FDA is typically a 0.5 percentage point HbA1c reduction versus placebo. The Bamosa effect size is three times that threshold.
The trial limitations should be noted: single-blind rather than double-blind, single-center, and the patients were on background diabetes medication so the pure black-seed effect cannot be perfectly isolated. But the dose-response relationship and the magnitude of effect make this one of the strongest human studies for any herbal hypoglycemic.
The Heshmati & Namazi 2015 Iranian RCT
The Heshmati & Namazi 2015 trial published in Complementary Therapies in Clinical Practice replicated and extended the Bamosa findings using black seed oil rather than seed powder:
- Population: 70 Iranian patients with type 2 diabetes
- Intervention: Black seed oil 2.5 mL twice daily versus placebo (sunflower oil 2.5 mL twice daily) added to existing diabetes therapy
- Duration: 8 weeks
- Primary outcomes: HbA1c, fasting glucose, lipid profile, blood pressure, body weight
Results:
- HbA1c reduction: approximately 1.0 percentage point versus placebo
- Fasting glucose reduction: approximately 35 mg/dL versus placebo
- Total cholesterol reduction: ~20 mg/dL versus placebo
- LDL reduction: ~17 mg/dL versus placebo
- Triglyceride reduction: ~25 mg/dL versus placebo
- HDL increase: ~4 mg/dL versus placebo
- Systolic blood pressure: small but statistically significant reduction
- Body weight: small reduction (~1.5 kg over 8 weeks) versus stable in placebo
The Heshmati design was stronger than Bamosa in two ways: it was double-blind, and it used a placebo arm rather than only dose comparisons. The replication of the HbA1c effect at roughly the same magnitude using a different form of black seed (oil vs powder), in a different population (Iranian vs Saudi), with a different design (placebo-controlled vs dose-ranging), strengthens the confidence that the effect is real and not a single-center artifact.
The simultaneous improvement in all four metabolic-syndrome lipid markers (cholesterol, LDL, triglycerides, HDL) along with glucose and a small blood pressure reduction is unusual — most single-agent interventions target one pathway. Black seed's multi-target activity at the NF-kB / AMPK / lipid-metabolism node produces a coordinated metabolic-syndrome improvement.
Meta-Analyses of Black Seed in Type 2 Diabetes
Several meta-analyses have pooled the available black seed diabetes trials. The 2017 meta-analysis by Daryabeygi-Khotbehsara et al. in Complementary Therapies in Medicine pooled 15 trials (n = 1,025 patients) and found:
- Mean HbA1c reduction: 0.71 percentage points versus control
- Mean fasting glucose reduction: 17.4 mg/dL versus control
- Mean total cholesterol reduction: 19.0 mg/dL versus control
- Mean triglyceride reduction: 22.0 mg/dL versus control
- Mean LDL reduction: 22.0 mg/dL versus control
The pooled effect is somewhat smaller than the individual Bamosa and Heshmati trials, partly because the meta-analysis includes lower-dose trials and trials with shorter duration. But the consistency of direction across 15 different trials, conducted in different countries and using different black seed preparations, is the meaningful signal — this is not a single-trial finding that fails to replicate.
A subsequent 2019 meta-analysis by Hadi et al. focusing specifically on glycemic control found similar HbA1c benefit and noted that the effect was larger in trials using black seed for longer than 8 weeks, consistent with the gradual onset of effect typical of insulin-sensitizing interventions (similar to how metformin's full glycemic effect takes 4–8 weeks to develop).
Thymoquinone and Pancreatic Beta-Cell Protection
Type 2 diabetes is characterized by both insulin resistance (peripheral tissues do not respond properly to insulin) and progressive pancreatic beta-cell failure (the cells that produce insulin gradually die off, partly from oxidative stress and partly from glucotoxicity). Most diabetes medications address insulin resistance (metformin, thiazolidinediones) or stimulate residual beta-cell function (sulfonylureas, GLP-1 agonists). Few medications meaningfully protect the beta cells from ongoing damage.
Thymoquinone has shown striking beta-cell protective effects in animal models. In the classic streptozotocin (STZ) and alloxan diabetic-rat models — in which a single high dose of STZ or alloxan selectively destroys pancreatic beta cells via oxidative damage and produces diabetes within days — pretreatment with thymoquinone partially blocks beta-cell destruction. Histology of pancreatic islets in TQ-pretreated rats shows preserved islet architecture and substantially higher beta-cell mass compared to untreated diabetic controls.
The mechanism involves several converging effects:
- Direct antioxidant activity — thymoquinone is a quinone with significant free-radical scavenging activity, particularly against the superoxide and hydroxyl radicals generated by STZ/alloxan metabolism in beta cells
- Mitochondrial protection — TQ preserves mitochondrial membrane potential and prevents the mitochondrial permeability transition that triggers beta-cell apoptosis
- Anti-apoptotic signaling — TQ upregulates Bcl-2 and downregulates Bax in beta cells, shifting the apoptosis/survival balance toward survival
- Suppression of NF-kB-driven inflammatory beta-cell damage — chronic low-grade pancreatic inflammation contributes to T2D progression; TQ's NF-kB inhibition addresses this
The human translation is necessarily indirect — we cannot biopsy human pancreatic islets to measure beta-cell mass in living patients — but the C-peptide measurements in the clinical trials (C-peptide is a surrogate for endogenous insulin production, hence for beta-cell function) suggest that black seed users maintain beta-cell function better than placebo controls over the trial periods studied. This is a potentially distinctive benefit of black seed compared to most other diabetes interventions, which tend to either work the beta cells harder (sulfonylureas, accelerating burnout) or merely improve insulin response without addressing beta-cell preservation.
AMPK Activation — The Metformin-Like Mechanism
Metformin, the first-line oral medication for type 2 diabetes worldwide, works primarily by activating AMP-activated protein kinase (AMPK) in the liver. AMPK is the cellular energy sensor — when cellular ATP levels fall (signaling low energy), AMPK activates a cascade of responses that increases ATP-generating processes (fatty acid oxidation, glucose uptake) and suppresses ATP-consuming processes (gluconeogenesis, fatty acid synthesis, cholesterol synthesis).
Thymoquinone activates AMPK through a mechanism distinct from but parallel to metformin. The downstream effects on glucose metabolism are similar:
- Suppressed hepatic gluconeogenesis — the liver makes less glucose, lowering fasting glucose levels (this is the primary action of metformin and of black seed)
- Increased peripheral glucose uptake — skeletal muscle and adipose tissue take up more glucose, lowering postprandial glucose
- Suppressed lipogenesis — the liver makes less fatty acid and triglyceride, contributing to the lipid profile improvements
- Improved insulin sensitivity — AMPK activation reduces hepatic insulin resistance over time
The clinical practical implication is that black seed and metformin appear to have additive rather than redundant glycemic effects in trial settings — patients on metformin who add black seed still see additional HbA1c reduction. The mechanisms overlap but the molecular targets are sufficiently distinct that the effects sum rather than max out. This is consistent with the Bamosa trial, in which patients added black seed on top of their existing metformin-based therapy and still saw a 1.5 percentage point further HbA1c drop.
For patients who cannot tolerate metformin (the GI side effects are dose-limiting for 10–15% of users) or who have advanced renal disease that contraindicates metformin (eGFR < 30), black seed may offer a partial AMPK-targeting alternative — though dose adjustment and close glucose monitoring is essential.
Insulin Sensitivity at Muscle and Liver
Beyond the AMPK pathway, black seed appears to improve insulin signaling in skeletal muscle and liver through additional mechanisms. Animal studies have shown:
- Increased GLUT4 translocation to skeletal muscle cell membrane (the glucose transporter that responds to insulin)
- Increased IRS-1 phosphorylation (a key insulin signaling intermediate)
- Reduced hepatic insulin resistance markers
- Reduced inflammatory cytokines (TNF-alpha, IL-6) that drive insulin resistance
The TNF-alpha and IL-6 connection is particularly interesting because obesity-driven type 2 diabetes is increasingly understood as an inflammatory condition — chronic low-grade inflammation in adipose tissue and liver drives insulin resistance, which drives compensatory hyperinsulinemia, which over years drives beta-cell failure. By reducing the inflammatory signal at the source (NF-kB inhibition), black seed addresses the root inflammatory driver of T2D, not just the downstream glucose elevation.
This is also why black seed's benefit is especially pronounced in patients with the obese, metabolic-syndrome phenotype of T2D rather than in lean autoimmune-like T2D or LADA (latent autoimmune diabetes in adults). For more on metabolic-syndrome-driven T2D, see Insulin Resistance and Diabetes.
Lipid Improvements: Cholesterol, LDL, Triglycerides
The consistent lipid improvement seen across black seed trials is large enough to be clinically relevant in its own right, independent of the glycemic benefit. The Heshmati trial showed:
- Total cholesterol: ~20 mg/dL reduction (equivalent to a low-dose statin)
- LDL: ~17 mg/dL reduction
- Triglycerides: ~25 mg/dL reduction (a strong effect — comparable to a moderate dose of fenofibrate)
- HDL: ~4 mg/dL increase (HDL is notoriously hard to raise; a few mg/dL is meaningful)
The mechanism is multi-faceted:
- Reduced hepatic cholesterol synthesis — thymoquinone modestly inhibits HMG-CoA reductase (the enzyme target of statins) and reduces lipogenic gene expression
- Increased LDL receptor expression — more LDL receptors means more LDL clearance from circulation
- Improved triglyceride clearance — via AMPK-mediated upregulation of fatty acid oxidation and lipoprotein lipase activity
- Improved HDL function and modest HDL elevation
For a patient with combined metabolic syndrome (T2D + dyslipidemia + hypertension), black seed addresses all three components at once. The magnitude of each individual effect is smaller than dedicated single-agent therapy (a full-dose statin reduces LDL by 40–60%, far more than the 20% from black seed), but the convenience of one intervention with multi-system effect and the favorable safety profile make black seed an attractive adjunct or first-line option for patients seeking nonpharmaceutical approaches.
Metabolic Syndrome and Weight Trial Evidence
Beyond strict T2D, black seed has been studied in metabolic syndrome (the cluster of central obesity + dyslipidemia + hypertension + insulin resistance / hyperglycemia that precedes overt T2D). The Mahdavi trial in obese women (n = 84, 8 weeks of black seed oil 3 g/day) showed:
- Weight loss of approximately 4.3 kg versus 1.8 kg in placebo
- Waist circumference reduction
- BMI reduction
- Triglyceride and total cholesterol reduction
- Inflammatory marker (hs-CRP) reduction
The weight loss is modest in absolute terms but meaningful as part of a lifestyle-plus-supplement metabolic syndrome reversal protocol. The combination of weight loss + lipid improvement + reduced inflammation + improved insulin sensitivity makes black seed a credible adjunct for metabolic-syndrome reversal alongside dietary changes (low-carbohydrate or Mediterranean pattern), regular physical activity, and other proven interventions.
For the broader metabolic-syndrome management framework, see Metabolic Syndrome and Blood Sugar Management.
Practical Dosing for Pre-Diabetes and Type 2 Diabetes
Based on the clinical trials, the dosing protocol that has produced measurable benefit is:
- Whole black seed powder: 2–3 grams per day, divided into two doses (morning and evening with meals). 1 g = approximately 1/2 teaspoon ground.
- Black seed oil (cold-pressed): 2.5 mL twice daily (5 mL/day total), taken with food for fat absorption. Refrigerate after opening.
- Standardized capsule: 500–1000 mg standardized black seed extract twice daily, with the extract specifying TQ content (target 2–5%).
- Duration: Expect 4–8 weeks before measurable HbA1c effect, similar to metformin. Continue at least 12 weeks before judging effect.
- Monitoring: Check HbA1c at baseline and at 12 weeks. Check fasting glucose and home glucose self-monitoring during the first 2–4 weeks to catch any unexpected hypoglycemia (especially important if also on insulin or sulfonylureas).
- Combinable with: Metformin, GLP-1 agonists, SGLT2 inhibitors — additive effects with low hypoglycemia risk.
- More caution with: Insulin, sulfonylureas (glipizide, glyburide), meglitinides (repaglinide) — these can produce hypoglycemia when combined with black seed unless dose-adjusted downward.
Drug Interactions and Hypoglycemia Risk
- Insulin and sulfonylureas — the most important interaction. Black seed lowers blood glucose, and adding it to insulin or sulfonylurea therapy can produce hypoglycemia within days. Reduce the insulin or sulfonylurea dose by 10–20% when starting black seed and monitor glucose closely. Adjust further based on observed glucose readings.
- Warfarin and antiplatelet drugs — black seed has mild antiplatelet activity. Combined with warfarin, aspirin, or clopidogrel, it may increase bleeding risk. Monitor INR more frequently when starting black seed in a warfarin patient.
- CYP3A4 substrates — black seed inhibits CYP3A4 (the cytochrome P450 enzyme responsible for metabolizing many drugs). This can elevate serum levels of:
- Statins (simvastatin and lovastatin particularly affected; atorvastatin less so)
- Calcium channel blockers (amlodipine, felodipine)
- Cyclosporine, tacrolimus (organ transplant patients should avoid)
- Some chemotherapy drugs
- Antihypertensive drugs — black seed lowers blood pressure modestly. Combined with ACE inhibitors, ARBs, or other antihypertensives, may produce additive blood pressure reduction. Monitor BP and consider dose adjustment if symptomatic hypotension occurs.
- Pregnancy contraindication — high-dose black seed should not be used in pregnancy (uterine-stimulant effects in animal studies, dose-dependent abortifacient activity).
- Surgery — discontinue at least 2 weeks before planned surgery due to antiplatelet effect.
The good news: in the clinical trials, no serious adverse events have been reported at the doses used. The interactions above are manageable with awareness and appropriate monitoring. Black seed is one of the better-tolerated herbal interventions in diabetes care, with substantially fewer side effects than metformin (no GI intolerance), sulfonylureas (hypoglycemia, weight gain), or thiazolidinediones (fluid retention, fracture risk).
Key Research Papers
- Bamosa AO et al. (2010). Effect of Nigella sativa seeds on the glycemic control of patients with type 2 diabetes mellitus. Indian Journal of Physiology and Pharmacology. — PubMed
- Heshmati J, Namazi N (2015). Effects of black seed (Nigella sativa) oil on glycemic control in patients with type 2 diabetes. Complementary Therapies in Clinical Practice. — PubMed
- Daryabeygi-Khotbehsara R et al. (2017). Nigella sativa improves glucose homeostasis and serum lipids: A systematic review and meta-analysis. Complementary Therapies in Medicine. — PubMed
- Hadi V et al. (2019). The effect of Nigella sativa on glycemic control in patients with type 2 diabetes: A systematic review and meta-analysis. Phytotherapy Research. — PubMed
- Mahdavi R et al. (2015). Effects of Nigella sativa oil with a low-calorie diet on cardiometabolic risk factors in obese women. Food & Function. — PubMed
- Kanter M et al. (2004). Protective effects of Nigella sativa on the histological structure of streptozotocin-induced diabetic rat pancreas. Anatomical Record. — PubMed
- El-Mahmoudy A et al. (2005). Thymoquinone lowers blood glucose and reduces oxidative stress in a rat model of diabetes. Planta Medica. — PubMed
- Najmi A et al. (2008). Effect of Nigella sativa oil on various clinical and biochemical parameters of metabolic syndrome. International Journal of Diabetes in Developing Countries. — PubMed
- Sahebkar A et al. (2016). A systematic review and meta-analysis of randomized controlled trials investigating the effects of supplementation with Nigella sativa on plasma lipid concentrations. Pharmacological Research. — PubMed
- Benhaddou-Andaloussi A et al. (2008). The in vivo antidiabetic activity of Nigella sativa is mediated through activation of the AMPK pathway and increased muscle Glut4 content. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Fararh KM et al. (2002). Nigella sativa oil lowers blood glucose and ameliorates pancreatic islet damage in streptozotocin-diabetic hamsters. Research in Veterinary Science. — PubMed
- Hosseinzadeh H et al. (2017). The application of Nigella sativa and thymoquinone in metabolic syndrome and its components: a systematic review. Iranian Journal of Basic Medical Sciences. — PubMed
PubMed Topic Searches
- PubMed: Nigella sativa type 2 diabetes HbA1c
- PubMed: Thymoquinone pancreatic beta cell
- PubMed: Nigella sativa AMPK / insulin
- PubMed: Nigella sativa lipid meta-analysis
- PubMed: Nigella sativa metabolic syndrome / obesity
Connections
- Black Seed Overview
- Black Seed Benefits Hub
- Black Seed for Immune & Antiviral
- Black Seed for Asthma
- Black Seed for Inflammation
- Type 2 Diabetes
- Insulin Resistance
- Metabolic Syndrome
- Blood Sugar Management
- Fenugreek (parallel blood-sugar herb)
- Cinnamon
- Berberine (parallel AMPK activator)
- Turmeric
- Magnesium (insulin sensitivity)
- Chromium
- HbA1c Lab Test
- Continuous Glucose Monitor
- Metformin — the first-line AMPK-activating diabetes drug black seed is benchmarked against and combined with.