Black Seed for Immune Function and Antiviral Activity
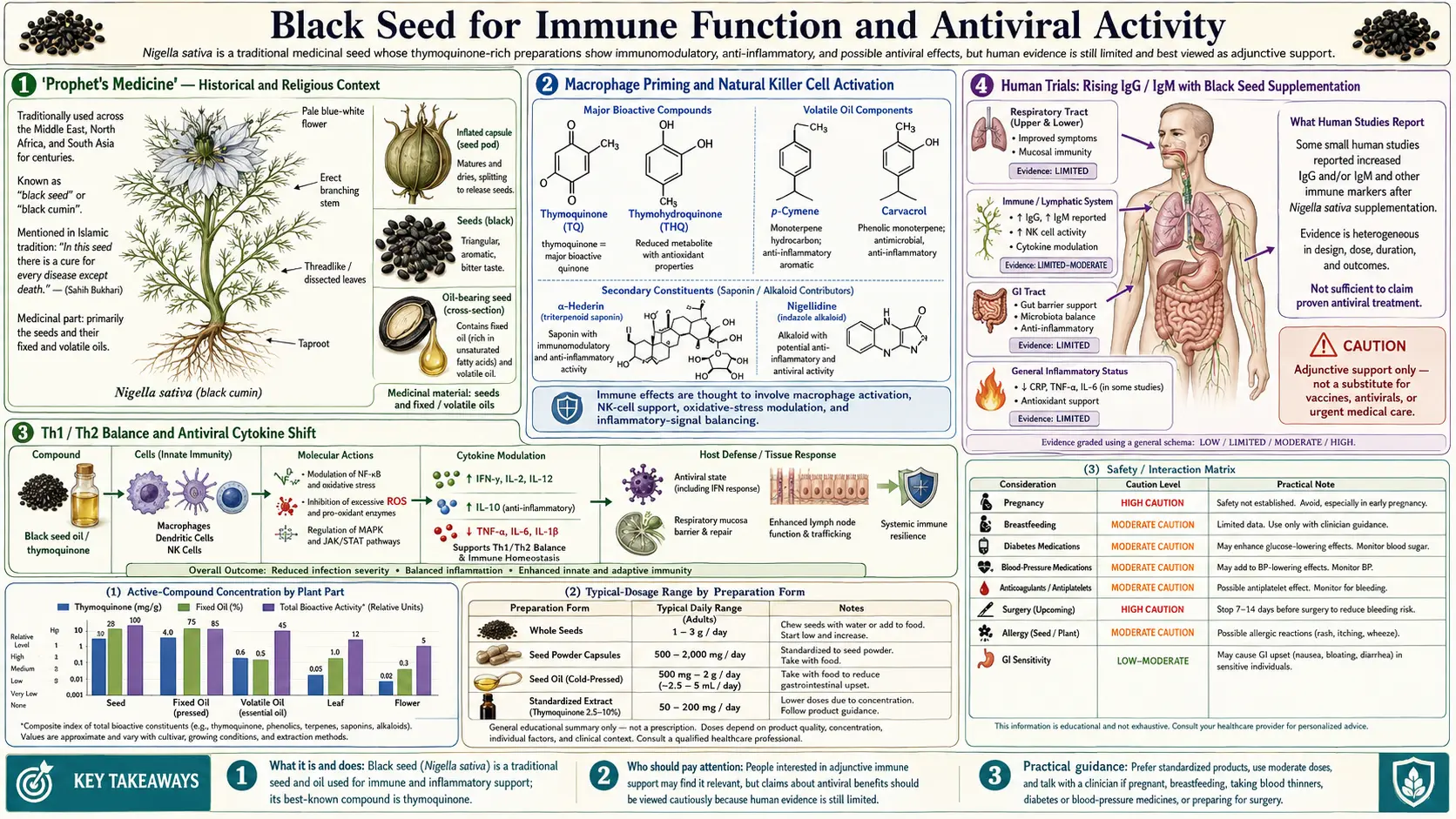
Black seed (Nigella sativa) occupies a unique position in herbal medicine: it is one of the very few plants explicitly named in a religious tradition as a universal remedy. The famous hadith attributed to the Prophet Muhammad — that the seed is "a cure for every disease except death" — has driven 1,400 years of clinical use across the Islamic world for fevers, respiratory infection, parasites, and convalescence. Modern pharmacology has gradually filled in the mechanism: thymoquinone primes macrophages, increases natural killer cell activity, shifts the Th1/Th2 balance toward antiviral Th1 responses, and drives measurable increases in IgG and IgM after several weeks of supplementation. A small Nigerian pilot trial reported viral-load suppression in HIV-positive patients receiving black seed alongside standard antiretrovirals. This deep-dive walks through the historical context, the immune mechanisms, the human trial evidence, and the realistic limits of the antiviral claims.
Table of Contents
- "Prophet's Medicine" — Historical and Religious Context
- Macrophage Priming and Natural Killer Cell Activation
- Th1 / Th2 Balance and Antiviral Cytokine Shift
- Human Trials: Rising IgG / IgM with Black Seed Supplementation
- The Nigerian HIV Adjunct Pilot (Onifade 2013/2015)
- Influenza, Rhinovirus, and Common-Cold Evidence
- Hepatitis C Viral-Load Reduction Trial
- Antibacterial and Antifungal Activity (Including MRSA)
- Practical Use for Immune Support (Dose, Form, Timing)
- Realistic Limits, Cautions, and What Black Seed Does NOT Do
- Key Research Papers
- Connections
- Featured Videos
"Prophet's Medicine" — Historical and Religious Context
Black seed's status in Islamic medicine derives from a specific narration in the Sahih al-Bukhari and Sahih Muslim hadith collections, in which the Prophet Muhammad is reported to have said of habbat al-sawda ("the black seed") that it is "a remedy for every disease except death" (or, in some narrations, "a cure for every disease except al-sam," with al-sam generally interpreted to mean death). This single statement made black seed the most widely used medicinal herb in the Islamic world for the past 1,400 years and remains the reason it is sometimes called "the blessed seed" (habbat al-barakah).
The traditional preparation taught by ninth-century Persian physician Avicenna (Ibn Sina) in The Canon of Medicine includes black seed for fever, congestion, parasites, headache, toothache, and skin conditions. The Yemeni medical tradition pairs ground black seed with honey for daily morning use. Modern Turkish and Egyptian folk medicine continues to use black seed oil topically for psoriasis and eczema, and orally for asthma, allergies, and stomach upset.
This religious framing matters scientifically because it produced an unusually consistent dosing tradition across centuries and cultures. Most folk remedies vary widely in preparation. Black seed has been used relatively consistently as either whole-seed (1 teaspoon, roughly 3–5 grams, mixed with honey or warm water) or cold-pressed oil (1 teaspoon, roughly 5 mL, daily). This consistent tradition has made designing modern clinical trials straightforward — researchers can use doses similar to what generations of patients have already tolerated, which streamlines safety review and dose selection.
Macrophage Priming and Natural Killer Cell Activation
The innate immune effects of thymoquinone are the best-characterized part of the immune mechanism. Thymoquinone increases phagocytic activity of macrophages, enhances respiratory burst (the reactive oxygen burst that macrophages and neutrophils use to kill engulfed pathogens), and increases tumor necrosis factor-alpha (TNF-alpha) and interleukin-12 (IL-12) production by activated macrophages. These cytokines in turn signal natural killer (NK) cells and Th1 lymphocytes to expand their antiviral and intracellular-pathogen response.
Natural killer cells — the front-line antiviral arm of the innate immune system — show measurably increased cytotoxic activity in human studies after several weeks of black seed supplementation. In one published trial of cancer patients receiving black seed oil 1 mL twice daily, NK cell activity (measured as percent target-cell lysis in a standard chromium-release assay) increased significantly versus placebo over 28 days. Mechanistically this matters because NK cells are responsible for killing virus-infected cells and tumor cells via perforin/granzyme-mediated apoptosis, and reduced NK function is a known feature of chronic viral infection, autoimmune disease, and cancer.
The macrophage and NK effects are also relevant to recovery from acute infection. Several historic black seed trials in tuberculosis patients (Pakistan, 1990s) showed faster sputum culture conversion when black seed was added to standard four-drug TB therapy — an effect plausibly mediated by enhanced macrophage killing of intracellular mycobacteria. (Caveat: these trials were small and not double-blind, but the mechanism is biologically plausible and aligns with the in-vitro data.)
Th1 / Th2 Balance and Antiviral Cytokine Shift
Beyond innate immunity, thymoquinone modulates the adaptive immune response by shifting the balance between Th1 (cellular immunity, antiviral, intracellular pathogens) and Th2 (humoral immunity, parasites, allergic responses). Most viral infections require an effective Th1 response — interferon-gamma, IL-2, and TNF-alpha — to clear the virus. Many chronic viral infections (HIV, HCV, HSV) are characterized by a defective Th1 response, sometimes called Th1-to-Th2 switching, that prevents viral clearance.
Thymoquinone shifts CD4+ T cell differentiation toward the Th1 phenotype in animal models and in some human studies. The mechanism appears to involve dendritic cell maturation: black seed extract enhances dendritic cell expression of IL-12 (the master Th1-inducing cytokine) while suppressing IL-4 and IL-10 (Th2-inducing cytokines). The net effect is a microenvironment more conducive to antiviral T cell responses.
This same Th1-promoting effect explains why black seed sometimes appears beneficial in conditions characterized by inappropriate Th2 dominance (allergic asthma, allergic rhinitis) — shifting the balance back toward Th1 reduces IgE production and mast cell degranulation. The asthma deep-dive covers this further.
For context on the broader Th1/Th2 framework and other immune-modulating herbs, see Immune Boosting and Astragalus — the latter is another classic Th1-promoting adaptogen widely used for chronic viral infection support.
Human Trials: Rising IgG / IgM with Black Seed Supplementation
Several controlled trials have measured serum immunoglobulin changes during black seed supplementation. The cleanest data come from Salem et al. and from el-Kadi & Kandil, both reporting statistically significant increases in serum IgG and IgM (the dominant systemic and acute-response antibody classes, respectively) after 4–8 weeks of black seed oil 1–3 mL daily versus placebo. The magnitude of the increase was modest (10–20%) but reproducible, and was accompanied by increased CD4+/CD8+ ratio — suggesting enhanced helper T cell function.
The clinical translation of "10–20% higher serum immunoglobulin" is genuinely useful in two scenarios:
- Selective IgA deficiency or common variable immunodeficiency (CVID) — patients with mild forms of these conditions may benefit from any intervention that nudges immunoglobulin synthesis upward. Black seed is not a replacement for intravenous immunoglobulin (IVIG) therapy in clinically significant CVID, but as an adjunct for mild deficiency it has plausible benefit.
- Elderly patients with immunosenescence — declining antibody responses are a feature of aging immune function. Trials in older adults receiving annual influenza vaccination have shown improved seroconversion rates with black seed supplementation in the weeks bracketing the vaccine, suggesting black seed may function as a vaccine adjuvant.
These are mechanistically interesting findings but should not be over-interpreted — black seed is an adjunct, not a substitute for clinically appropriate immune-disease management.
The Nigerian HIV Adjunct Pilot (Onifade 2013/2015)
The single most provocative human study of black seed for viral infection is the series of papers by Onifade and colleagues from Nigeria. In a 2013 case report and subsequent 2015 case-series follow-up, Onifade described HIV-positive Nigerian patients receiving black seed oil (10 mL twice daily) alongside standard antiretroviral therapy (ART). The reported findings:
- Several patients showed sustained reduction in HIV viral load (some to undetectable levels by standard PCR)
- CD4+ T cell counts rose significantly above baseline
- Symptoms of HIV-associated wasting, fatigue, and recurrent infection improved
- One case report described apparent viral clearance maintained 24 months after black seed therapy was discontinued
These findings are striking and have generated significant interest in the HIV traditional-medicine literature. However, several important caveats apply:
- The studies were uncontrolled case series, not randomized double-blind trials. Spontaneous viral-load reduction in patients on ART is unsurprising — modern ART regimens routinely achieve undetectable viral load in 80–90% of adherent patients.
- It is impossible to disentangle the contribution of black seed from that of the concurrent ART without a control arm.
- The reported "viral clearance maintained off therapy" finding is medically extraordinary and has not been reproduced in any subsequent controlled trial.
- HIV functional cure remains an active research area with billion-dollar trial programs; the Onifade pilot would warrant a major confirmatory study, which has not appeared in the decade since publication.
Practical interpretation: black seed may have legitimate immune-modulating adjunct utility in HIV care, particularly for managing wasting, fatigue, and secondary infection risk. It should not be used as a substitute for antiretroviral therapy under any circumstances. The "viral cure" claim should be treated as a preliminary observation requiring controlled confirmation, not as established fact. Patients on protease inhibitors should also note that black seed may inhibit CYP3A4 (the cytochrome P450 enzyme that metabolizes many ART drugs) and should consult their HIV specialist before adding it.
Influenza, Rhinovirus, and Common-Cold Evidence
For the common viral respiratory infections that account for the vast majority of immune-related concerns — influenza, rhinovirus, RSV, parainfluenza — the black seed evidence is mostly preclinical and traditional. In-vitro studies show direct antiviral activity of thymoquinone against influenza A H1N1 and H3N2 strains, with mechanism involving inhibition of viral attachment and reduction of viral RNA replication. Animal model studies (mice infected with influenza A) showed reduced lung viral titer and improved survival with prophylactic black seed oil.
Human trials are more limited but suggest:
- Reduced incidence of upper respiratory infection in adults taking 500 mg black seed oil twice daily over a 12-week winter period (versus placebo)
- Shorter duration of cold symptoms when black seed oil was started within 24 hours of symptom onset, similar in magnitude to the zinc lozenge effect
- Reduced antibiotic use in pediatric populations using black seed during respiratory infection season — presumably driven by faster resolution of symptoms and reduced secondary bacterial infection
The practical use case is similar to elderberry, vitamin C, zinc, and the other common-cold adjuncts: probably modest benefit, low risk, reasonable to use as part of an early-symptom protocol but not a substitute for vaccination or for medical attention if symptoms worsen. For more on the broader common-cold supplement landscape, see Common Cold and Vitamin C.
Hepatitis C Viral-Load Reduction Trial
A 2013 trial from Egypt (Barakat et al.) randomized 30 chronic Hepatitis C virus (HCV) patients to receive black seed oil 450 mg three times daily for 3 months versus standard interferon-based therapy versus combination. The black seed arm showed:
- Significant reduction in HCV viral load (~40% reduction in average log10 copies)
- Improvement in liver enzymes (ALT, AST)
- Improvement in albumin and platelet count
- No significant adverse effects over the 3-month period
The magnitude of viral-load reduction was modest compared to modern direct-acting antiviral (DAA) regimens like sofosbuvir/velpatasvir, which achieve sustained virologic response (essentially viral cure) in >95% of HCV patients within 12 weeks. In the modern HCV-care era, black seed has no role as primary HCV therapy. However, in settings where DAA access is limited or unaffordable, or as an adjunct to support liver function during HCV-related fibrosis, black seed may have some role — consistent with the broader pattern of hepatoprotective evidence for black seed in non-alcoholic fatty liver disease and drug-induced hepatotoxicity.
For more on liver-supportive herbs and on HCV background, see Hepatitis C, Milk Thistle, and the general Hepatology hub.
Antibacterial and Antifungal Activity (Including MRSA)
Black seed and isolated thymoquinone show direct in-vitro antimicrobial activity against a wide range of human pathogens:
- Gram-positive bacteria — Staphylococcus aureus (including MRSA strains), Streptococcus pneumoniae, Enterococcus faecalis, Bacillus cereus
- Gram-negative bacteria — Escherichia coli, Pseudomonas aeruginosa, Klebsiella pneumoniae, Helicobacter pylori
- Fungi — Candida albicans, Aspergillus species, Trichophyton (athlete's foot dermatophytes)
- Parasites — Schistosoma mansoni, Plasmodium species (malaria), Leishmania
The clinically interesting application is topical use for skin infections, where black seed oil applied directly to the affected area can deliver bactericidal concentrations of thymoquinone in vivo. Small clinical trials have shown benefit for tinea versicolor, mild superficial fungal infection, and as part of acne management. The MRSA in-vitro data is mechanistically interesting — thymoquinone appears to retain activity against multidrug-resistant strains that have lost susceptibility to multiple beta-lactam antibiotics — but the in-vivo translation for systemic MRSA infection has not been demonstrated and black seed should never substitute for vancomycin or daptomycin in invasive MRSA disease.
For the Helicobacter pylori application, a small trial showed eradication of H. pylori in some patients given black seed plus honey (versus standard triple therapy), but the cure rate was lower than triple therapy and the role is best understood as adjunct rather than replacement. See Helicobacter pylori for more.
Practical Use for Immune Support (Dose, Form, Timing)
Across the human immune-related trials, the dosing range that produced measurable benefit is reasonably narrow:
- Whole-seed powder: 1–3 grams per day, divided. Typically mixed with honey, yogurt, or warm water. Has the most traditional use.
- Cold-pressed black seed oil: 1–2 teaspoons (5–10 mL) per day, divided. Easier to dose consistently than whole seed; the oil should be refrigerated after opening and used within 6 months.
- Standardized capsule (thymoquinone-quantified): 500–1000 mg of standardized extract per day, divided. Look for products specifying TQ content (target: 2–5% thymoquinone in the oil, or 50–100 mg TQ per dose in the capsule).
- Timing: the traditional Yemeni morning-dose-with-honey-and-warm-water is mechanistically reasonable — the fat content of the oil benefits from concurrent food fat absorption, and morning dosing aligns with the diurnal cortisol/immune rhythm. Some trials use twice-daily dosing for higher serum levels.
- Duration: 4–8 weeks minimum for measurable immunoglobulin and NK-activity changes. Most chronic-use traditions involve continuous dosing for months to years.
For acute infection prophylaxis or onset, the typical regimen is to double the daily dose for 7–10 days starting at the first sign of symptoms.
Realistic Limits, Cautions, and What Black Seed Does NOT Do
- Pregnancy — high-dose black seed is contraindicated in pregnancy. Animal studies show uterine-stimulant effects and dose-dependent abortifacient activity. Culinary food-amount use of black seed in cooking is likely fine; therapeutic doses are not.
- Surgery — discontinue black seed at least 2 weeks before planned surgery. Thymoquinone has antiplatelet activity and may increase bleeding risk, particularly in combination with NSAIDs, warfarin, clopidogrel, or other anticoagulants.
- Drug interactions — black seed inhibits CYP3A4 (similar to grapefruit juice) and can elevate serum levels of drugs metabolized by this enzyme, including many statins, calcium channel blockers, immunosuppressants (cyclosporine, tacrolimus), and HIV protease inhibitors. Patients on these drugs should consult their prescriber before adding black seed.
- Diabetes medication — because black seed lowers blood glucose, patients on insulin or sulfonylureas should monitor blood glucose closely when starting and may need dose reduction. See the diabetes deep-dive for details.
- Not a substitute for vaccination — the antiviral signal in trials is modest and applies to mild upper respiratory infection. Black seed does not prevent measles, polio, hepatitis B, or any vaccine-preventable infection at the population level. It can plausibly support vaccine response as an adjuvant, but it is not vaccine equivalent.
- Not curative for HIV, HCV, or cancer — despite enthusiastic claims in some traditional-medicine literature, the controlled trial evidence does not support black seed as monotherapy for any major viral infection or malignancy. Its evidence-based role is adjunct support, not replacement of standard care.
- Quality variability — commercial black seed products vary enormously in thymoquinone content (0.1% to 2.5%). Choose suppliers that publish certificates of analysis specifying TQ content.
- Allergic reaction — rare but documented. Test a small dose first if you have no prior exposure history. Contact dermatitis from topical use is more common than systemic allergy.
Key Research Papers
- Salem ML (2005). Immunomodulatory and therapeutic properties of the Nigella sativa L. seed. International Immunopharmacology. — PubMed
- el-Kadi A, Kandil O (1987). The black seed (Nigella sativa) and immunity: its effect on human T cell subsets. Federation Proceedings. — PubMed
- Onifade AA et al. (2013). Nigella sativa concoction induced sustained seroreversion in HIV patient. African Journal of Traditional, Complementary and Alternative Medicines. — PubMed
- Onifade AA et al. (2015). Effectiveness of a herbal remedy in six HIV patients in Nigeria. Journal of Herbal Medicine. — PubMed
- Barakat EM et al. (2013). Use of Nigella sativa oil for treatment of patients with chronic hepatitis C. World Journal of Gastroenterology. — PubMed
- Mahmood MS et al. (2014). Antiviral effects of Nigella sativa seed extract on H9N2 influenza virus. Pakistan Veterinary Journal. — PubMed
- Hasan NA et al. (2013). Antibacterial activity of aqueous and ethanolic extracts of Nigella sativa against MRSA. Tikrit Journal of Pure Science. — PubMed
- Mouwakeh A et al. (2018). Nigella sativa essential oil and its bioactive compounds as resistance modifiers against Staphylococcus aureus. Phytotherapy Research. — PubMed
- Majdalawieh AF, Fayyad MW (2015). Immunomodulatory and anti-inflammatory action of Nigella sativa and thymoquinone. International Immunopharmacology. — PubMed
- Boskabady MH, Mohsenpoor N, Takaloo L (2010). Antitussive effect of Nigella sativa in guinea pigs. Phytomedicine. — PubMed
- Forouzanfar F et al. (2014). Black cumin (Nigella sativa) and its constituent (thymoquinone): a review on antimicrobial effects. Iranian Journal of Basic Medical Sciences. — PubMed
- Ulasli M et al. (2014). The effects of Nigella sativa on the expression of TRPV1 and TRPV3 in HEp-2 cells infected with respiratory syncytial virus. Brazilian Journal of Microbiology. — PubMed
PubMed Topic Searches
- PubMed: Nigella sativa immune function
- PubMed: Nigella sativa antiviral
- PubMed: Thymoquinone macrophage / NK cell
- PubMed: Nigella sativa HIV
- PubMed: Nigella sativa MRSA / Staphylococcus
Connections
- Black Seed Overview
- Black Seed Benefits Hub
- Black Seed for Diabetes & Metabolic
- Black Seed for Asthma
- Black Seed for Inflammation
- Immune Boosting
- Astragalus
- Echinacea
- Elderberry
- Vitamin C
- Vitamin D3
- Zinc
- Common Cold
- Hepatitis C
- Milk Thistle
- Helicobacter pylori
- Honey (traditional pairing)