Natural Mast Cell Stabilizers for MCAS
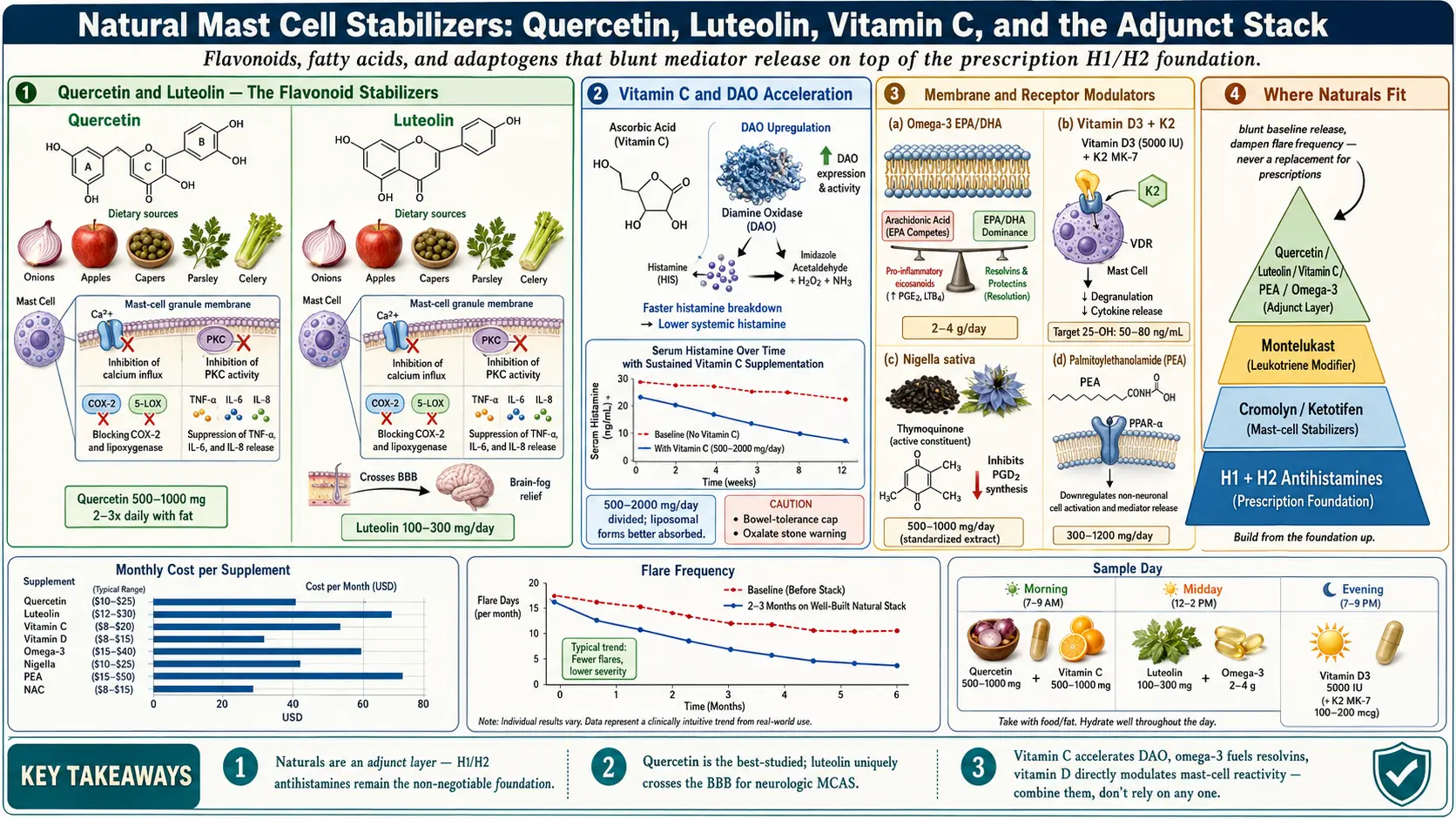
Table of Contents
- Where Natural Stabilizers Fit in MCAS Treatment
- Quercetin — The Best-Studied Natural Stabilizer
- Luteolin — Quercetin’s Slightly-More-Potent Cousin
- Vitamin C — Histamine Release and Clearance
- Nigella Sativa (Black Seed / Black Cumin)
- Holy Basil (Tulsi) — Adaptogenic Support
- Vitamin D — More Important Than People Realize
- Omega-3 Fatty Acids (EPA/DHA)
- Palmitoylethanolamide (PEA)
- Bromelain
- N-Acetylcysteine (NAC)
- The Practical Stack — A Sample Routine
- What the Natural Stack Is NOT
- Product Quality — What to Look For
- Start Slow
- Key Research Papers
- Research Papers (PubMed)
- Connections
- Featured Videos
1. Where Natural Stabilizers Fit in MCAS Treatment
Let’s start with the most important sentence on this page: natural mast cell stabilizers are never a replacement for H1 and H2 antihistamines in symptomatic MCAS. If you are having flushing, hives, GI reactions, tachycardia, or anaphylactoid episodes, the prescription foundation is non-negotiable — see H1 and H2 Blocker Stacks and Cromolyn and Ketotifen.
Where natural stabilizers earn their place is as an adjunct layer on top of that foundation. They can blunt baseline mediator release, reduce the frequency and intensity of flares, and address the oxidative and inflammatory soup that prescription antihistamines don’t directly touch. Patients frequently find that after 2–3 months of a well-built natural stack, they can titrate their ketotifen or cromolyn doses down — not eliminate them, but reduce the load. For patients who can’t tolerate certain prescriptions (mast cell reactions to dyes, fillers, or the active molecule itself), a natural-heavy regimen sometimes becomes the functional primary therapy by necessity.
The trials are mostly small. Quality of evidence varies dramatically from compound to compound. What follows is an honest tier-by-tier look.
2. Quercetin — The Best-Studied Natural Stabilizer
Quercetin is a flavonoid found in onions, apples, capers, and berries. Among natural compounds studied for mast cell stabilization, quercetin has the deepest and most consistent literature.
Mechanism
Quercetin inhibits mast cell degranulation primarily by reducing intracellular calcium influx and inhibiting protein kinase C (PKC) activity — both upstream of granule release. It also inhibits COX-2 and lipoxygenase, dampening prostaglandin and leukotriene synthesis, and suppresses release of TNF-α, IL-6, IL-8, and other pro-inflammatory cytokines from activated mast cells.
Evidence
In vitro and animal data are strong. Small human trials in allergic rhinitis, interstitial cystitis, chronic prostatitis, and chronic fatigue syndrome show modest but measurable benefit. It is not a magic bullet, but among natural compounds it is the closest to one.
Dose
500–1000 mg, 2–3 times daily with meals. Bioavailability is notoriously poor for plain quercetin dihydrate and is improved substantially by taking it with food (especially some fat).
Forms
- Quercetin dihydrate — cheapest, poorest absorption
- Quercetin phytosome — bound to phosphatidylcholine (e.g. Thorne Quercetin Phytosome); 6–10x better absorption
- EMIQ (enzymatically modified isoquercitrin) — the most bioavailable form on the market
Products
Thorne Quercetin Phytosome, Pure Encapsulations Quercetin, Source Naturals Activated Quercetin (a quercetin + bromelain + vitamin C combo — bromelain is itself a mild mast cell influence).
Drug Interactions
Mild CYP3A4 inhibition, theoretically affecting some medications but clinically rarely significant at typical doses. May modestly affect anticoagulation. Separate from iron supplements by 2 hours (quercetin chelates iron).
Cost
$20–45/month at therapeutic doses.
3. Luteolin — Quercetin’s Slightly-More-Potent Cousin
Luteolin is structurally similar to quercetin (another flavonoid, found in celery, parsley, artichoke, and thyme) but is frequently described by researchers as the more potent mast cell stabilizer of the pair. Its standout feature for MCAS: it crosses the blood-brain barrier better than quercetin, which makes it particularly useful for the neurologic side of MCAS — brain fog, anxiety, noise and light sensitivity, neuroinflammation.
Dose
100–300 mg/day in divided doses. Less is needed than quercetin because of higher intrinsic potency.
Forms and Products
Often found in combination with quercetin. Algonot NeuroProtek is a physician-formulated luteolin + quercetin + rutin combination developed by Theoharis Theoharides specifically for MCAS and autism-related mast cell activation. Stand-alone products include Swanson Luteolin and Pure Encapsulations Luteolin.
Cost
$40–80/month.
4. Vitamin C — High Doses Inhibit Histamine Release and Increase Clearance
Ascorbic acid is the most mundane-looking supplement on this list and one of the more reliably helpful for MCAS.
Mechanism
Vitamin C inhibits mast cell degranulation directly and accelerates the activity of diamine oxidase and histaminase, the enzymes that clear circulating histamine. The practical consequence: serum histamine drops measurably with sustained vitamin C supplementation.
Dose
500–2000 mg/day in divided doses. Liposomal vitamin C is better absorbed and causes far less GI upset. For refractory patients under IV-practitioner care, IV vitamin C (25–100 g) is sometimes used.
Caution
Chronic doses above 2000 mg/day carry a small kidney-stone risk, especially with a history of calcium oxalate stones. Individual bowel tolerance caps the oral dose — exceed it and you get osmotic diarrhea.
Forms and Products
Ascorbic acid (cheapest, acidic), sodium ascorbate (stomach-friendly buffered), liposomal vitamin C (best absorbed, pricier). Reputable brands include Thorne Liposomal, LivOn Labs, and Pure Encapsulations.
Cost
$10–40/month.
5. Nigella Sativa (Black Seed / Black Cumin)
An ancient remedy with modern evidence. The active compound is thymoquinone.
Mechanism
Thymoquinone inhibits histamine release and prostaglandin D2 synthesis, reduces pro-inflammatory cytokine output, and has direct antimicrobial activity.
Evidence
Several small randomized trials in allergic rhinitis, asthma, and atopic eczema show symptom reduction. No dedicated MCAS trials yet, but mechanistic overlap is strong.
Dose
1–2 tsp cold-pressed black seed oil/day, or 500 mg twice daily in capsule form, standardized to ≥1% thymoquinone.
Products
Amazing Herbs Premium Black Seed Oil, Life Extension Black Cumin Seed Oil.
Warnings
May potentiate blood thinners; use caution at high doses with SSRIs.
Cost
$20–40/month.
6. Holy Basil (Tulsi) — Adaptogenic + Mild Stabilizer
Holy basil (Ocimum sanctum) is an Ayurvedic adaptogen. Its value in MCAS is less about direct mast cell stabilization (which is modest) and more about blunting the cortisol-CRH axis that drives stress-triggered flares.
Mechanism
Reduces cortisol reactivity to psychological stress, which indirectly lowers mast cell activation via the CRH-mast-cell pathway. Mild direct stabilizing effect as well.
Dose
300–600 mg standardized extract/day, or 2–3 cups tulsi tea daily.
Products
Organic India Tulsi Holy Basil, Himalaya Holy Basil.
Best For
Patients whose flares are clearly stress-triggered — bad week at work, argument, poor sleep. Less useful for food or chemical triggers.
Cost
$10–25/month.
7. Vitamin D — More Important Than People Realize
Vitamin D status correlates so strongly with allergic and mast cell disease severity that checking it should be reflex for any MCAS patient. Low 25-OH vitamin D is associated with worse asthma, worse atopic dermatitis, worse chronic urticaria, and worse MCAS symptom burden.
Mechanism
Vitamin D directly regulates mast cell reactivity via the vitamin D receptor on mast cells themselves, modulates T-regulatory cell function, and dampens Th2 skew.
Dose
Target a serum 25-OH vitamin D of 50–80 ng/mL. For most adults this means 5000 IU D3 daily, but the correct dose is whatever gets your level into range. Retest every 3–6 months.
Cofactors
Take vitamin K2 (MK-7 100–200 mcg/day) alongside D3 to direct calcium deposition into bone rather than soft tissue and arteries.
Products
Thorne D/K2 Drops, Pure Encapsulations D3/K2, or any third-party-tested brand.
Cost
$8–20/month.
8. Omega-3 Fatty Acids (EPA/DHA)
Not a stabilizer in the classical sense, but an essential substrate for the resolvins and protectins that actively terminate inflammation.
Mechanism
EPA and DHA shift eicosanoid balance away from pro-inflammatory arachidonic-acid-derived mediators toward resolving mediators. Also modestly stabilize mast cell membranes by incorporating into phospholipid bilayers.
Dose
2–4 g combined EPA+DHA per day — higher than general-population recommendations. For MCAS you want a real anti-inflammatory dose, not a wellness dose.
Forms
Triglyceride form absorbs best, followed by ethyl ester, then phospholipid (krill). Third-party testing for mercury, PCBs, and oxidation is critical — rancid fish oil is pro-inflammatory.
Products
Nordic Naturals ProOmega, Carlson Elite EPA Gems, Thorne Super EPA.
Cost
$30–60/month at therapeutic dose.
9. Palmitoylethanolamide (PEA) — Newer Kid on the Block
PEA is an endogenous fatty acid amide structurally related to the endocannabinoids. It has a growing evidence base in chronic pain, neuropathy, and, increasingly, MCAS.
Mechanism
PEA binds the PPAR-α receptor, inhibits mast cell degranulation (sometimes described in the literature as “ALIA” — autacoid local inflammation antagonism), and reduces neuropathic and inflammatory pain.
Dose
300–600 mg, 2–3 times daily. Micronized PEA absorbs substantially better than standard powder.
Evidence
Promising randomized data in peripheral neuropathy, sciatic pain, and endometriosis-related pain. Growing off-label use in MCAS, where the combination of mast cell suppression plus neuropathic pain relief is especially welcome.
Products
Gencor Levagen PEA (micronized), Enzymatic Therapy PEA.
Cost
$40–80/month.
10. Bromelain — From Pineapple Stem
A proteolytic enzyme with indirect anti-inflammatory and mast cell effects, often paired with quercetin to improve absorption and add its own inflammation-dampening action.
Dose
500–1000 mg between meals for the anti-inflammatory effect. With meals if used as a digestive enzyme (different indication).
Combinations
Frequently stacked with quercetin — e.g. Source Naturals Activated Quercetin.
Caution
Amplifies blood thinners. Stop 2 weeks before any surgery.
11. N-Acetylcysteine (NAC) — Glutathione Precursor
NAC is a precursor to glutathione, the intracellular antioxidant that activated mast cells deplete rapidly. Raising glutathione levels reduces the oxidative stress that drives mast cell over-reactivity.
Dose
600–1200 mg twice daily.
Note
The FDA briefly restricted OTC NAC sales a few years ago; it is currently available again, but the regulatory status continues to evolve. Availability may change.
12. The Practical Stack — A Sample Routine
An integrated daily stack built from the above, suitable as an adjunct layer on top of a prescription antihistamine foundation:
- AM: quercetin 500 mg + vitamin C 1000 mg + vitamin D 5000 IU + K2 100 mcg + omega-3 2 g
- Midday: quercetin 500 mg + vitamin C 500 mg + bromelain 500 mg (between meals)
- Evening: quercetin 500 mg + PEA 300 mg (with dinner)
Total cost: approximately $100–180/month for the full stack. Add luteolin, black seed oil, or holy basil as indicated by symptom profile.
13. What the Natural Stack Is NOT
- Not a replacement for prescription H1 + H2 antihistamines in symptomatic MCAS.
- Not for severe flares. If you’re crashing, use your rescue medications and, if needed, epinephrine. Supplements don’t work on that timescale.
- Not “safe” just because it’s “natural.” Drug interactions, quality issues, and idiosyncratic reactions are real. MCAS patients in particular react unpredictably to things “normal” people don’t.
- Not a substitute for addressing root triggers — diet, sleep, stress, environmental exposures, infections. See Triggers and Flare Management.
14. Product Quality — What to Look For
- Third-party testing — look for NSF, USP, ConsumerLab, or Informed-Sport certification.
- Avoid fillers — excessive magnesium stearate, FD&C dyes, titanium dioxide, and artificial flavors can all trigger reactions in MCAS patients. Clean capsules only.
- Prefer single-ingredient formulations first, so if you react to something you know what caused it. Combination products come later once you’ve established tolerance of each component.
- Reputable brands: Thorne, Pure Encapsulations, Designs for Health, Nordic Naturals, Jarrow, NOW Foods (lower tier but consistently tested).
- Avoid: proprietary blends that hide doses, undisclosed ingredient sources, MLM supplements (Young Living, doTERRA, Herbalife, etc.), and house-brand Amazon generics with no certificate of analysis.
15. Start Slow
Introduce one supplement at a time, 3–7 days each, starting at half the target dose. MCAS patients react to additives, dyes, capsule material, and sometimes the compound itself in ways that are impossible to predict in advance. Track everything in a flare diary — symptom, time, suspected trigger — so you can attribute reactions correctly rather than abandoning a useful supplement for the wrong reason. Cross-reference with the triggers workflow in Triggers and Flare Management.
If you react to a single-ingredient product, try a different brand before giving up on the molecule — fillers vary wildly. A Thorne quercetin and a bargain-brand quercetin are, in a meaningful sense, different products.
16. Key Research Papers
- Mlcek J, Jurikova T, Skrovankova S, Sochor J. Quercetin and its anti-allergic immune response. Nutrients. 2016;8(3):167.
- Jafarinia M, et al. Quercetin with the potential effect on allergic diseases. Allergy, Asthma & Clinical Immunology. 2020.
- Theoharides TC, Stewart JM, Hatziagelaki E, Kolaitis G. Brain “fog,” inflammation and obesity: key aspects of neuropsychiatric disorders improved by luteolin. Frontiers in Neuroscience. 2017.
- Yip KH, Kolesnikoff N, Yu C, et al. Mechanisms of vitamin D’s action on the immune response and mast cells. BioFactors. 2020.
17. Research Papers
Live PubMed searches for the peer-reviewed literature on natural mast cell stabilizers and related MCAS adjuncts.
- PubMed: Quercetin and mast cells
- PubMed: Luteolin, mast cells, and MCAS
- PubMed: Vitamin C and histamine
- PubMed: Nigella sativa and allergic disease
- PubMed: Vitamin D and mast cells
- PubMed: PEA (palmitoylethanolamide) and mast cells
- PubMed: Natural mast cell stabilizers
- PubMed: Omega-3s and mast cell inflammation
Connections
- MCAS Overview
- Quercetin
- H1 & H2 Blocker Stacks
- Triggers & Flares
- Cromolyn & Ketotifen
- Vitamin C
- Holy Basil (Tulsi)
- Testing Guide
- Low-Histamine Diet
- Mediators & Symptom Map
- Hereditary Alpha-Tryptasemia
- POTS
- SIBO
- Vitamin D3
- Black Seed
- NAC
- MCAS Hormone Sensitivity