Shortness of Breath
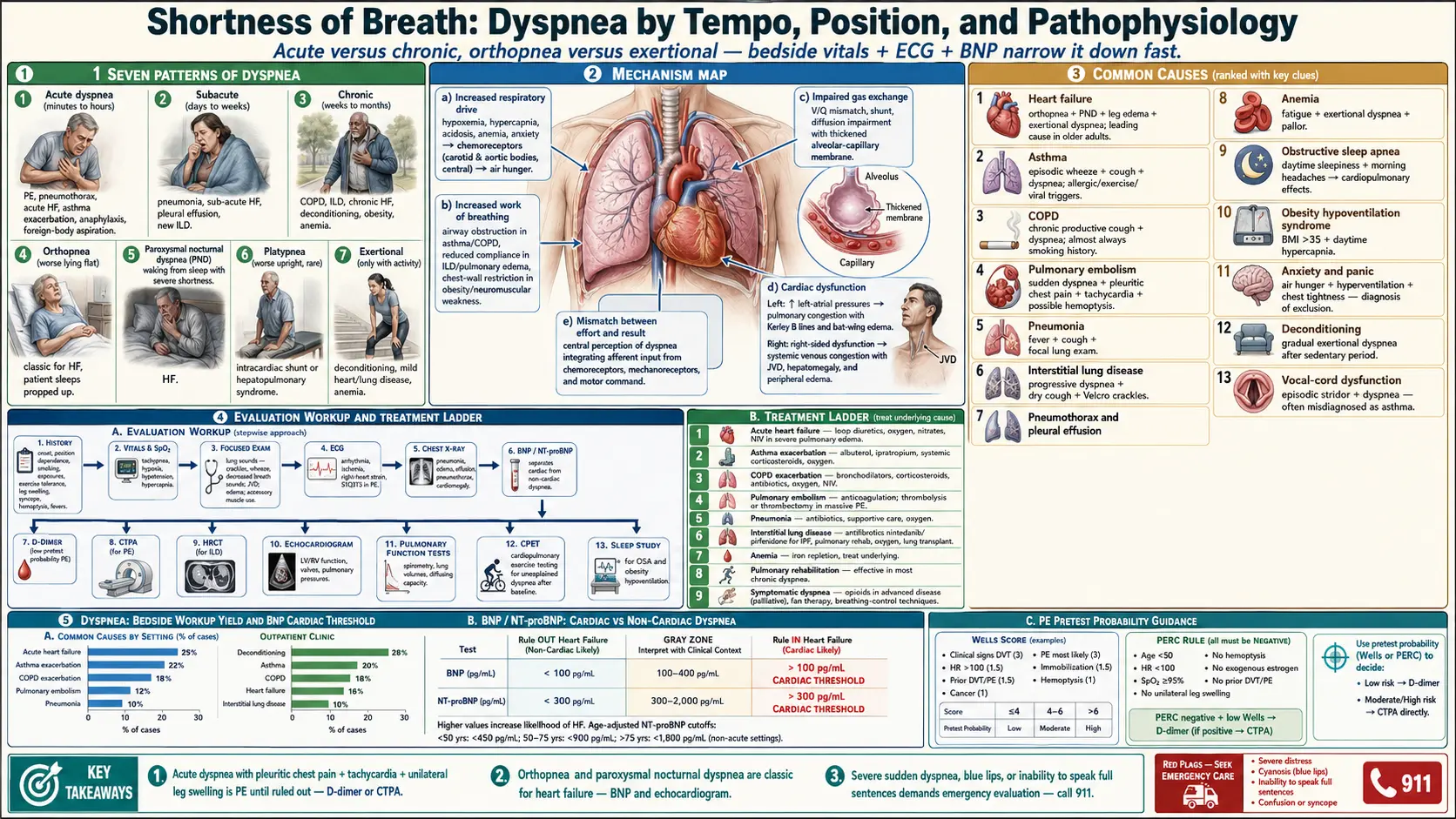

Table of Contents
- Overview
- Types of Dyspnea
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Shortness of breath — or dyspnea — is the subjective experience of breathing discomfort. It is one of the most common reasons for ambulance calls and ER visits, and a frequent reason adults stop exercising before they realize anything is wrong with their heart or lungs. Like chest pain, dyspnea can mean almost anything — deconditioning, anemia, anxiety, asthma, heart failure, pulmonary embolism, ILD, or cancer — and the workup is layered: a quick set of bedside vitals and an ECG narrow it down at the bedside, with imaging and pulmonary function tests filling in the rest.
Types of Dyspnea
- Acute dyspnea — sudden onset over minutes to hours; suggests pulmonary embolism, pneumothorax, acute heart failure, asthma exacerbation, anaphylaxis, foreign-body aspiration.
- Subacute dyspnea — days to weeks; often pneumonia, sub-acute heart failure, pleural effusion, or new ILD.
- Chronic dyspnea — weeks to months; COPD, ILD, chronic heart failure, deconditioning, obesity, anemia.
- Orthopnea — dyspnea worse lying flat; classic for heart failure.
- Paroxysmal nocturnal dyspnea — waking from sleep with severe shortness of breath; heart failure.
- Platypnea — dyspnea worse upright; rare; suggests intracardiac shunt or hepatopulmonary syndrome.
- Exertional dyspnea — only with activity; deconditioning, mild heart or lung disease, anemia.
Common Causes
- Heart failure — orthopnea, PND, leg edema, exertional dyspnea; one of the leading causes in older adults.
- Asthma — episodic wheeze, cough, and dyspnea; often triggered by allergens, exercise, viral infections.
- COPD — chronic productive cough and dyspnea, almost always with smoking history.
- Pulmonary embolism — sudden dyspnea, pleuritic chest pain, tachycardia, possible hemoptysis.
- Pneumonia — fever, cough, focal lung exam.
- Interstitial lung disease — progressive dyspnea, dry cough, Velcro crackles.
- Pneumothorax and pleural effusion — sudden unilateral chest pain and dyspnea.
- Anemia — fatigue and exertional dyspnea, often pallor.
- Obstructive sleep apnea — daytime sleepiness, morning headaches; over time cardiopulmonary effects produce dyspnea.
- Obesity hypoventilation syndrome — especially BMI >35 with daytime hypercapnia.
- Anxiety and panic disorder — air hunger, hyperventilation, chest tightness; diagnosis of exclusion.
- Deconditioning — gradual exertional dyspnea after prolonged sedentary period or illness.
- Vocal-cord dysfunction — episodic stridor and dyspnea, often misdiagnosed as asthma.
Mechanisms
- Increased respiratory drive — from hypoxemia, hypercapnia, acidosis, anemia, or anxiety stimulates chemoreceptors and produces air hunger.
- Increased work of breathing — airway obstruction (asthma, COPD), reduced compliance (ILD, pulmonary edema), or chest-wall restriction (obesity, neuromuscular weakness).
- Impaired gas exchange — ventilation-perfusion mismatch, shunt, diffusion impairment.
- Cardiac dysfunction — elevated left-atrial pressures cause pulmonary congestion; right-sided dysfunction causes systemic venous congestion.
- Mismatch between effort and result — the central perception of dyspnea integrates afferent input from chemoreceptors, mechanoreceptors, and motor command, producing the subjective sensation.
Evaluation
- History — onset, position dependence, smoking, exposures, exercise tolerance, leg swelling, syncope, hemoptysis, fevers.
- Vital signs and oxygen saturation — tachypnea, hypoxia, hypotension, hypercapnia.
- Focused exam — lung sounds (crackles, wheeze, decreased), JVD, edema, accessory muscle use.
- ECG — arrhythmia, ischemia, right-heart strain.
- Chest X-ray — pneumonia, edema, effusion, pneumothorax, cardiomegaly.
- BNP / NT-proBNP — helps separate cardiac from non-cardiac dyspnea.
- D-dimer — in low-pretest-probability patients to rule out PE.
- CT pulmonary angiogram — for suspected PE; HRCT for ILD.
- Echocardiogram — left and right ventricular function, valves, pulmonary pressures.
- Pulmonary function tests — spirometry, lung volumes, diffusing capacity for chronic dyspnea.
- Cardiopulmonary exercise testing (CPET) — for unexplained dyspnea after baseline workup.
- Sleep study — for OSA and obesity hypoventilation.
Management
- Treat the underlying cause — this is the cornerstone; everything else is supportive.
- Acute heart failure — loop diuretics, oxygen, vasodilators (nitrates), non-invasive ventilation in severe pulmonary edema.
- Asthma exacerbation — albuterol, ipratropium, systemic corticosteroids, oxygen.
- COPD exacerbation — bronchodilators, corticosteroids, antibiotics, oxygen, NIV.
- Pulmonary embolism — anticoagulation; thrombolysis or thrombectomy in massive PE.
- Pneumonia — antibiotics, supportive care, oxygen.
- ILD — antifibrotics (nintedanib, pirfenidone for IPF), pulmonary rehabilitation, oxygen, lung transplant in selected.
- Anemia — iron repletion, treat underlying cause.
- Pulmonary rehabilitation — effective in most chronic dyspnea.
- Symptomatic dyspnea — opioids in advanced disease (palliative); fan therapy; breathing-control techniques.
When to Seek Medical Care
- Severe sudden dyspnea, blue lips, or unable to speak full sentences — call 911.
- Dyspnea with chest pain, syncope, or unilateral leg swelling (suspect PE).
- Dyspnea with fever and productive cough (suspect pneumonia).
- Orthopnea or PND in someone with known or suspected heart disease.
- Hemoptysis, especially in smokers or with recent immobility.
- Progressive exertional dyspnea over weeks to months.
- Dyspnea in a pregnant woman, postpartum, or postoperative patient (PE risk).
- Wheeze that does not respond to a rescue inhaler.
Connections
- All Symptoms
- COPD
- Asthma
- Pulmonary Embolism
- Anemia
- Heart Failure
- Pneumonia
- Obstructive Sleep Apnea
- Interstitial Lung Disease
- Edema
- Chest Pain
- Pleural Effusion
- Anxiety
- Obesity
- Arrhythmia
- Pulmonary Hypertension
- Chronic Cough
- Allergies
- Lymphoma
References & Research
Historical Background
The systematic taxonomy of dyspnea began with William Harvey's 17th-century circulation work and was refined by 20th-century physiologists. The MRC dyspnea scale (1959) and the Borg scale (1982) standardized symptom reporting; cardiopulmonary exercise testing in the 1980s let clinicians separate ventilatory, cardiac, and gas-exchange limitations.
Key Research Papers
- Parshall MB, Schwartzstein RM, Adams L, et al. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. American Journal of Respiratory and Critical Care Medicine. 2012;185(4):435-452.
- Mahler DA, O'Donnell DE. Recent advances in dyspnea. Chest. 2015;147(1):232-241.
- Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. New England Journal of Medicine. 2002;347(3):161-167.
- Konstantinides SV, Meyer G. The 2019 ESC guidelines on acute pulmonary embolism. European Heart Journal. 2019;40(42):3453-3455.
- Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine. 2013;188(8):e13-e64.
- Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. New England Journal of Medicine. 2014;370(22):2071-2082.
- Currow DC, McDonald C, Oaten S, et al. Once-daily opioids for chronic dyspnea: a dose increment and pharmacovigilance study. Journal of Pain and Symptom Management. 2011;42(3):388-399.
- Coccia CB, Palkowski GH, Schweitzer B, Motsohi T, Ntusi NA. Dyspnoea: pathophysiology and a clinical approach. South African Medical Journal. 2016;106(1):32-36.
- Berliner D, Schneider N, Welte T, Bauersachs J. The differential diagnosis of dyspnea. Deutsches Ärzteblatt International. 2016;113(49):834-845.
- Banzett RB, Schwartzstein RM. Dyspnea: don't just look, ask! American Journal of Respiratory and Critical Care Medicine. 2015;192(12):1404-1405.
PubMed Topic Searches
- Dyspnea evaluation
- BNP and heart-failure diagnosis
- Cardiopulmonary exercise testing for dyspnea
- Pulmonary rehabilitation in COPD
- Opioids for refractory dyspnea
- Vocal-cord dysfunction