Pleural Effusion
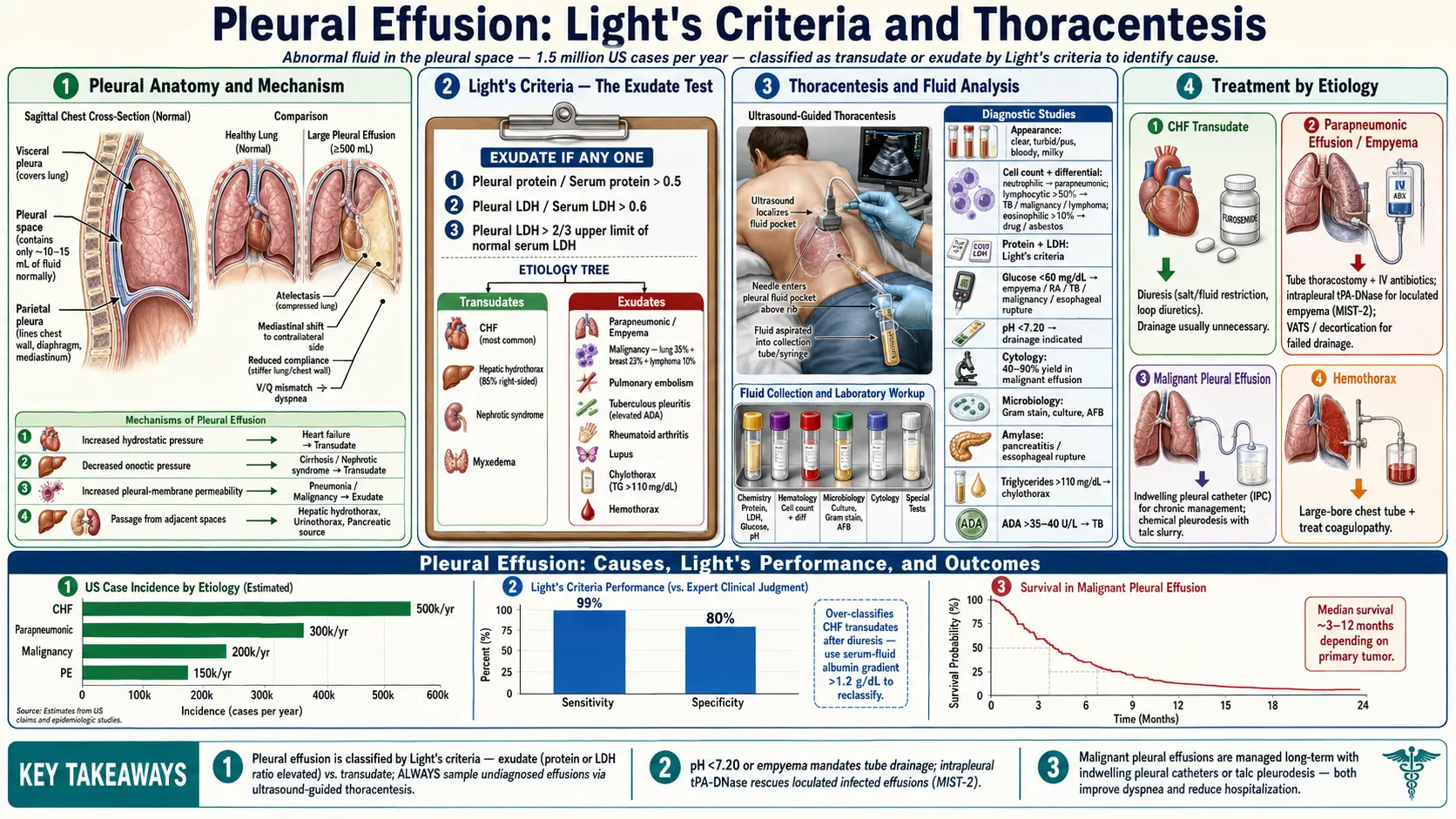
A pleural effusion is an abnormal accumulation of fluid in the pleural space — the thin cavity between the visceral pleura (covering the lung) and the parietal pleura (lining the chest wall). Normally only 15–20 mL of lubricating fluid occupies this space; effusions large enough to detect clinically typically exceed 200–300 mL. The critical first step in management is classifying the fluid as transudative or exudative using Light's criteria, which guides the entire subsequent diagnostic and treatment pathway.
Table of Contents
- Transudative vs. Exudative: Light's Criteria
- Transudative Causes
- Exudative Causes
- Symptoms and Clinical Diagnosis
- Imaging
- Diagnostic Thoracentesis
- Pleural Fluid Analysis
- Parapneumonic Effusions and Empyema
- Malignant Pleural Effusion
- Pulmonary Embolism, TB, and Other Causes
- Chylothorax
- Recurrent Effusion Management
- References & Research
- Featured Videos
Transudative vs. Exudative: Light's Criteria
The classification of pleural effusion as transudative or exudative is the fundamental first step because the differential diagnosis and treatment strategies differ substantially. Transudates result from imbalances in hydrostatic pressure and oncotic pressure that drive fluid across intact pleural membranes. Exudates result from inflammation, infection, malignancy, or impaired lymphatic drainage that increases pleural membrane permeability or blocks fluid clearance.
Light's Criteria
Published by Dr. Richard Light in 1972, Light's criteria remain the gold standard for fluid classification, with sensitivity of approximately 98% for exudates. An effusion is classified as exudative if at least one of the following three criteria is met:
- Pleural fluid protein / serum protein ratio >0.5
- Pleural fluid LDH / serum LDH ratio >0.6
- Pleural fluid LDH > two-thirds the upper limit of normal for serum LDH
If none of these criteria are met, the effusion is classified as transudative. The high sensitivity of Light's criteria comes with a cost: approximately 25% of transudates (especially those from heart failure treated with diuretics) are misclassified as exudates because diuresis concentrates pleural fluid protein and LDH. In this scenario, the serum-to-pleural fluid albumin gradient (serum albumin minus pleural albumin) helps: a gradient >1.2 g/dL strongly suggests a transudate despite exudative Light's criteria.
Transudative Causes
Transudative effusions result from systemic conditions affecting Starling forces across the pleural membrane. Because the pleural membrane itself is not diseased, the fluid has low protein and low LDH content.
Heart Failure (Most Common Cause of All Pleural Effusions)
Congestive heart failure (CHF) is the single most common cause of pleural effusions, accounting for up to 500,000 new cases per year in the United States. The mechanism is elevated hydrostatic pressure in pulmonary capillaries (left heart failure) and systemic venules (right heart failure), which drives ultrafiltrate across the visceral and parietal pleura faster than lymphatics can drain it. Effusions from CHF are typically bilateral (70%) or right-sided; unilateral left-sided effusion in a patient with apparent CHF should prompt further investigation for another etiology. Treatment is directed at the underlying heart failure (diuresis, afterload reduction). Therapeutic thoracentesis may be needed for large symptomatic effusions before cardiac compensation is achieved.
Cirrhosis (Hepatic Hydrothorax)
Hepatic hydrothorax — a pleural effusion in the setting of liver cirrhosis and portal hypertension — occurs in approximately 5–10% of cirrhotics. The primary mechanism is migration of ascitic fluid through small defects in the diaphragm into the pleural space (usually right-sided, occasionally bilateral or left-sided). The effusion can recur rapidly after thoracentesis when the underlying ascites is not controlled. Treatment targets the cirrhosis and ascites (sodium restriction, diuretics, transjugular intrahepatic portosystemic shunt, liver transplantation). Pleurodesis has a high failure rate in hepatic hydrothorax but can be attempted as a bridge to transplant.
Nephrotic Syndrome
Severe hypoalbuminemia from nephrotic syndrome (serum albumin <2.0 g/dL) reduces plasma oncotic pressure, allowing fluid to accumulate in multiple compartments including the pleural space. Effusions are typically bilateral and small. Treatment of the underlying nephropathy is the primary approach.
Other Transudative Causes
- Hypoalbuminemia from any cause (malnutrition, protein-losing enteropathy)
- Peritoneal dialysis (peritoneal fluid leak through diaphragm)
- Urinothorax (urine leak into pleural space — pleural creatinine > serum creatinine)
- Superior vena cava obstruction
- Myxedema (hypothyroidism)
Exudative Causes
Exudative effusions result from increased pleural membrane permeability, impaired lymphatic drainage, or direct pleural involvement by disease. They have higher protein and LDH content than transudates.
Parapneumonic Effusion (Most Common Exudative Cause)
A parapneumonic effusion is any pleural effusion in the setting of bacterial pneumonia, lung abscess, or bronchiectasis. It is the most common cause of exudative effusions, occurring in approximately 40% of hospitalized pneumonia patients. The majority are uncomplicated (free-flowing, sterile, pH >7.2, glucose >40 mg/dL) and resolve with antibiotic treatment of the pneumonia. A minority progress to complicated parapneumonic effusion or empyema (see below).
Malignancy
Malignant pleural effusion (MPE) is the second most common cause of exudative effusions overall. It occurs when metastatic tumor cells directly invade the pleural space or block mediastinal lymphatics, increasing pleural fluid production and impairing drainage. The most common primary cancers causing MPE are lung cancer (~35%), breast cancer (~25%), lymphoma (~10%), and ovarian cancer (~5%). Mesothelioma — a primary malignancy of the pleura itself — always involves the pleura directly. Effusions are typically large, recur rapidly after thoracentesis (within days to weeks), and carry poor prognosis (median survival 3–12 months depending on primary cancer type).
Tuberculosis
TB is the most common cause of exudative pleural effusion globally, though it is less common in developed countries. Tuberculous pleuritis results from a delayed hypersensitivity reaction to mycobacterial antigens released into the pleural space (usually from a subpleural focus), not from direct mycobacterial invasion. The fluid is typically lymphocyte-predominant (>90% lymphocytes), with low glucose and low pH in established disease. Adenosine deaminase (ADA) level in pleural fluid is elevated (>40 IU/L) in TB pleuritis with high sensitivity (~95%) and specificity (~90%) in high-prevalence settings — it is one of the most useful rapid diagnostic tests for TB effusion. Culture of pleural fluid for Mycobacterium tuberculosis is positive in only 25–40% of cases; pleural biopsy with culture yields higher positivity (~80%).
Pulmonary Embolism
Pleural effusion occurs in approximately 30% of patients with pulmonary embolism. The effusion results from pulmonary infarction (causing inflammatory reaction at the pleural surface) or from transient pleural ischemia. Characteristically the fluid may be bloody (hemorrhagic transudate or exudate), small to moderate in size, and resolves with anticoagulation treatment of the PE. The presence of a pleural effusion in a patient with pleuritic chest pain and dyspnea should always prompt consideration of PE. Because the effusion can be either transudative or exudative, it does not reliably distinguish PE from other causes — the clinical context and diagnostic testing for PE are paramount.
Symptoms and Clinical Diagnosis
The symptoms of pleural effusion are produced by compression of adjacent lung tissue and by pleural irritation.
Common Symptoms
- Dyspnea: The most common symptom; severity correlates roughly with effusion size and rate of accumulation. Rapidly accumulating effusions (as in malignancy) may cause severe dyspnea at moderate volumes; slowly accumulating chronic effusions (CHF) may be surprisingly well tolerated at large volumes.
- Pleuritic chest pain: Sharp, positional pain that worsens with breathing or coughing; indicates parietal pleural irritation. Common in parapneumonic effusions, PE, and TB; typically absent in CHF and malignancy (parietal pleura less inflamed).
- Non-productive cough: Compression of adjacent lung parenchyma.
- Symptoms of underlying disease: Fever and cough (pneumonia), peripheral edema (CHF), weight loss and hemoptysis (malignancy), night sweats (TB).
Physical Examination
The classic triad of pleural effusion on physical examination:
- Dullness to percussion: The most sensitive finding; requires ~400 mL of fluid to detect reliably.
- Absent or reduced breath sounds: Over the effusion.
- Decreased tactile fremitus: Fluid attenuates transmission of voice sounds to the chest wall.
Egophony (E to A change in voice transmission) may be heard at the upper border of the effusion. Mediastinal shift away from the effusion suggests a large effusion or trapped lung.
Imaging
Chest X-ray
Chest X-ray remains the initial imaging modality. On the posterior-anterior (PA) view, a meniscus sign (blunting of the costophrenic angle with a concave upper border) is visible with approximately 200–300 mL of fluid. Massive effusions can opacify an entire hemithorax with contralateral mediastinal shift. A lateral decubitus film can detect free-flowing effusions as small as 50–100 mL by showing fluid layering dependent to gravity.
Ultrasound
Thoracic ultrasound has transformed pleural procedures. Bedside ultrasound:
- Detects as little as 20 mL of pleural fluid — more sensitive than X-ray
- Distinguishes free-flowing effusions from loculated ones (important for drainage planning)
- Differentiates effusion from consolidation or pleural thickening
- Guides safe thoracentesis needle insertion in real time (reduces pneumothorax rate from ~5–10% with blind approach to <2% with ultrasound guidance)
- Identifies complex characteristics (septations, fibrin strands) suggesting empyema
CT Chest
Contrast-enhanced CT is invaluable for characterizing the pleural space, identifying the underlying cause, and planning more complex interventions:
- Identifies pleural thickening, nodularity, or masses suggesting malignancy or mesothelioma
- Detects loculations within the effusion
- Evaluates lung parenchyma for pneumonia, masses, or pulmonary infarcts
- CT with contrast can demonstrate pleural enhancement in empyema ("split pleura sign")
- CT pulmonary angiography can evaluate for PE simultaneously
Diagnostic Thoracentesis
Thoracentesis — needle aspiration of pleural fluid — is indicated for any clinically significant new or unexplained pleural effusion. In a patient with classic bilateral CHF effusions and no atypical features, it is reasonable to defer thoracentesis and treat the CHF, but any asymmetry, fever, or failure to respond to treatment should prompt fluid sampling.
Procedure
Thoracentesis is performed with the patient seated upright (if possible) with the arms supported, allowing the effusion to layer dependently in the posterior costophrenic sulcus. Ultrasound guidance is the standard of care. A small-gauge needle (22G) is inserted over the superior border of the lower rib to avoid the neurovascular bundle running along the inferior margin. Local anesthesia (lidocaine) is instilled into the pleura before aspiration. Pneumothorax, the most significant procedural risk, occurs in approximately 1–2% with ultrasound guidance.
Diagnostic vs. Therapeutic Thoracentesis
Diagnostic thoracentesis removes a small sample (typically 30–60 mL) for laboratory analysis. Therapeutic thoracentesis removes a larger volume to relieve dyspnea — typically up to 1,500 mL per procedure. Removing more than 1,500 mL at one sitting increases the risk of re-expansion pulmonary edema, which can cause severe hypoxemia. Patients should stop aspiration if they develop cough, chest tightness, or significant discomfort.
Pleural Fluid Analysis
The choice of tests to send on pleural fluid depends on the clinical context, but a systematic initial panel is efficient.
Appearance
- Clear/straw-colored: Typical transudate; also thin exudates.
- Turbid/cloudy: Suggests empyema (pus), chylothorax (fat), or high cellularity.
- Frank pus: Empyema — requires drainage regardless of other parameters.
- Bloody (hemorrhagic): Most importantly, malignancy, PE with infarct, and trauma. True hemothorax (hematocrit >50% of peripheral blood) requires chest tube drainage.
- Milky/turbid after centrifugation: Chylothorax — supernatant remains turbid due to chylomicrons (pseudochylothorax becomes clear after centrifugation).
Key Biochemical Tests
- Protein and LDH (with simultaneous serum): Light's criteria classification — mandatory on every initial tap.
- Glucose: Low pleural fluid glucose (<60 mg/dL, or pleural/serum ratio <0.5) narrows the differential to: empyema/complicated parapneumonic, rheumatoid pleuritis, malignancy (extensive), TB, esophageal rupture (very low, near 0 mg/dL), and lupus pleuritis.
- pH: Measured with a blood gas analyzer (not pH paper) on a heparinized, air-free specimen. pH <7.2 in the context of parapneumonic effusion indicates complicated parapneumonic effusion requiring chest tube drainage. Also low in empyema, esophageal rupture, malignancy, rheumatoid pleuritis, TB, and urinothorax. Never aspirate on room air.
- Cell count and differential: Neutrophil predominance (>50%) suggests acute processes: parapneumonic, PE, early TB. Lymphocyte predominance (>50–80%) suggests TB, malignancy, lymphoma, chronic chylothorax. Eosinophilia (>10%) seen in air or blood in pleural space, drug reactions, parasitic infection, Churg-Strauss.
- Cytology: Sensitivity for malignancy approximately 60–70% on a single sample; improved with larger volumes and repeat sampling. Negative cytology does not exclude malignancy — especially mesothelioma (low cytologic detection rate).
- Culture and Gram stain: For suspected infection; send in blood culture bottles to improve yield.
- Adenosine deaminase (ADA): Elevated (>40 IU/L) in TB pleuritis; highly useful in high-prevalence settings.
Parapneumonic Effusions and Empyema
Parapneumonic effusions progress through three stages, and management depends on the stage at presentation.
Stage 1: Uncomplicated (Exudative) Parapneumonic Effusion
Free-flowing, sterile fluid with pH >7.2, glucose >40 mg/dL, LDH <1000 IU/L, and negative Gram stain/culture. Resolves with antibiotics alone; does not require drainage. Most parapneumonic effusions are at this stage.
Stage 2: Complicated (Fibrinopurulent) Parapneumonic Effusion
Bacteria have entered the pleural space; fibrin strands begin to form loculations. pH <7.2, glucose <40 mg/dL, or positive Gram stain/culture indicates a complicated parapneumonic effusion. Chest tube drainage is mandatory — antibiotics alone will not resolve it, and progression to empyema is likely without drainage. A small-bore chest tube (14–16 Fr) placed under ultrasound guidance is as effective as large-bore tubes for most parapneumonic effusions and is better tolerated.
Stage 3: Empyema
Frank pus in the pleural space. Requires drainage. Loculated empyemas may require multiple tubes, ultrasound-guided repositioning, or surgical intervention (video-assisted thoracoscopic surgery, VATS).
Intrapleural Fibrinolytics: MIST1 and MIST2 Trials
Two landmark randomized trials tested the strategy of instilling fibrinolytics (clot-dissolving agents) through the chest tube to break down fibrin loculations and improve drainage:
- MIST1 (2005): Streptokinase vs. placebo in 430 patients with complicated parapneumonic effusion or empyema. Result: no benefit from streptokinase — no difference in death, need for surgery, or hospital stay. This was a major negative trial that dampened enthusiasm for single-agent fibrinolytics.
- MIST2 (2011): Factorial design testing tPA (alteplase), DNase (dornase alfa), both combined, or placebo. Result: the combination of tPA + DNase significantly improved pleural fluid drainage (reduced chest X-ray opacity), reduced surgical referral rate, and shortened hospital stay. Neither drug alone was significantly better than placebo. The combination works because tPA lyses fibrin (which traps the collection) while DNase breaks down DNA from neutrophils (which increases viscosity, preventing drainage). This combination is now used in clinical practice for complicated effusions not responding to tube drainage alone.
Malignant Pleural Effusion
Malignant pleural effusions (MPE) are a major source of dyspnea and suffering in patients with advanced cancer. The effusion is confirmed as malignant by cytological or histological evidence of malignant cells in the pleural fluid or on pleural biopsy (not merely the presence of an effusion in a cancer patient, which could be parapneumonic or related to treatment).
Management Principles
The goals are symptom relief and minimizing the number and invasiveness of repeat procedures. Two proven strategies for recurrent MPE:
Pleurodesis
Pleurodesis involves instilling a sclerosing agent (most commonly talc) into the pleural space via a chest tube or during VATS to fuse the visceral and parietal pleura together, obliterating the pleural space and preventing fluid re-accumulation. Talc pleurodesis at VATS (poudrage) has higher success rates (~80–90%) than bedside talc slurry via chest tube (~60–70%). The lung must be capable of full expansion (no trapped lung) for pleurodesis to work — if the lung cannot expand to reach the chest wall, the pleural surfaces cannot be apposed and pleurodesis fails.
Indwelling Pleural Catheter (IPC)
An indwelling pleural catheter (e.g., PleurX) is a small-bore tunneled catheter inserted into the pleural space under local anesthesia that remains in place permanently, allowing the patient or caregiver to drain fluid at home as needed (typically 2–3 times per week). IPCs are particularly suitable for patients with trapped lung (pleurodesis contraindicated), those with poor performance status who cannot tolerate VATS, and those who prefer ambulatory management.
TIME2 Trial
The TIME2 randomized trial (2012) compared talc pleurodesis versus IPC as first-line management for malignant pleural effusion. Both strategies achieved equivalent dyspnea relief over 12 months. IPC had a lower rate of successful pleurodesis but allowed outpatient management. Spontaneous pleurodesis occurred in approximately 46% of IPC patients (the catheter eventually becomes unnecessary). The choice between IPC and pleurodesis should be individualized based on patient preference, performance status, trapped lung, and life expectancy.
Pulmonary Embolism, TB, and Other Causes
Pleural Effusion in Pulmonary Embolism
Approximately 30% of PE patients develop a pleural effusion, usually small and unilateral on the side of the embolism. The effusion may be transudative (early, from transient ischemic pleural injury) or exudative (after pulmonary infarction). The classic triad of PE — pleuritic chest pain, dyspnea, hemoptysis — is actually uncommon as a complete triad; most patients have only one or two of these features. Any unexplained exudative effusion (particularly bloody) in a patient with risk factors for PE warrants CT pulmonary angiography. Treatment is anticoagulation for the PE; the effusion generally resolves without specific intervention.
Tuberculous Pleuritis
TB pleuritis presents as an acute febrile illness with pleuritic chest pain and exudative effusion in a patient with TB risk factors (endemic exposure, immunosuppression, incarceration). The chest X-ray may show a unilateral effusion without parenchymal infiltrate (primary TB pleuritis), which can be misdiagnosed as a parapneumonic effusion. Elevated ADA (>40 IU/L) with lymphocyte-predominant exudate should prompt empirical TB treatment pending culture results in endemic areas. Untreated TB pleuritis resolves spontaneously but up to 65% of patients develop pulmonary or extrapulmonary TB within 5 years — treatment is mandatory.
Mesothelioma
Malignant pleural mesothelioma arises from mesothelial cells and is strongly associated with asbestos exposure (30–40 year latency). It presents with unilateral effusion (often massive), progressive dyspnea, and chest pain. The effusion is often hemorrhagic or serosanguineous. Cytology has low sensitivity (~20–30%) for mesothelioma. Pleural biopsy (image-guided or thoracoscopic) with immunohistochemistry is required for diagnosis. Median survival is 12–18 months; multimodal therapy including chemotherapy (pemetrexed + platinum), immunotherapy, and selected surgical approaches may extend survival in eligible patients.
Chylothorax
Chylothorax is accumulation of chyle (lymphatic fluid rich in chylomicrons, triglycerides, and lymphocytes) in the pleural space, resulting from disruption or obstruction of the thoracic duct or major lymphatic tributaries. The fluid is milky or opalescent; the pleural fluid triglyceride level >110 mg/dL confirms chylothorax. Causes include:
- Traumatic/post-surgical: Most common cause in developed countries — thoracic surgery, central line placement, neck dissection. The thoracic duct is vulnerable during left-sided thoracic procedures.
- Malignancy: Lymphoma (the most common malignant cause), lung cancer, mediastinal tumors obstructing thoracic duct.
- Idiopathic: Especially in neonates.
Management: reduce chyle production with a medium-chain triglyceride (MCT) diet (MCTs are absorbed directly into portal circulation, bypassing the thoracic duct) or total parenteral nutrition; chest tube drainage; consider thoracic duct embolization or surgical ligation for high-output leaks (>1 L/day) persisting beyond 1–2 weeks.
Recurrent Effusion Management
When a pleural effusion recurs rapidly after initial thoracentesis (typically within 1–4 weeks), the approach shifts from diagnostic to definitive management of recurrence:
- Treat the underlying cause: For transudates, this is the priority — optimize heart failure therapy, treat cirrhosis, manage nephrotic syndrome. Repeated thoracentesis alone for a treatable transudate is poor practice.
- Pleurodesis: For recurrent exudates (particularly malignant) when the lung fully re-expands and the patient is an acceptable candidate. Talc is the most effective sclerosant.
- Indwelling pleural catheter (IPC): For recurrent malignant effusions or trapped lung where pleurodesis is not feasible.
- VATS with pleural biopsy and pleurodesis: Preferred when tissue diagnosis of malignancy has not yet been established and effusion is recurrent — diagnostic and therapeutic in one procedure.
- Pleuroperitoneal shunt: Rarely used; reserved for chylothorax or hepatic hydrothorax refractory to other measures.
References & Research
Key Research Papers
- Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972;77(4):507-513. PMID 4642731
- Maskell NA, Davies CW, Nunn AJ, et al; First Multicenter Intrapleural Sepsis Trial (MIST1) Group. U.K. controlled trial of intrapleural streptokinase for pleural infection. N Engl J Med. 2005;352(9):865-874. PMID 15745977
- Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med. 2011;365(6):518-526. PMID 21830966
- Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA. 2012;307(22):2383-2389. — Search PubMed
- Sahn SA. The diagnostic value of pleural fluid analysis. Semin Respir Crit Care Med. 1995;16(5):269-278. — Search PubMed
- Porcel JM, Light RW. Diagnostic approach to pleural effusion in adults. Am Fam Physician. 2006;73(7):1211-1220. — Search PubMed
- Hooper C, Lee YC, Maskell N; BTS Pleural Guideline Group. Investigation of a unilateral pleural effusion in adults: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65(Suppl 2):ii4-17. PMID 20696692
- Morales-Rull JL, Hernandez N, Solheiro-Gomez A, et al. Prevalence and prognostic impact of pleural effusion in acute heart failure. Eur J Heart Fail. 2016;18(7):817-826. — Search PubMed
- Porcel JM. Pearls and myths in pleural fluid analysis. Respirology. 2011;16(1):44-52. — Search PubMed
- Light RW. Parapneumonic effusions and empyema. Clin Chest Med. 2006;27(2):255-263. — Search PubMed
- Villena Garrido V, Cases Viedma E, Fernandez Villar A, et al. Recommendations of diagnosis and treatment of pleural effusion. Update. Arch Bronconeumol. 2014;50(6):235-249. — Search PubMed
- Bintcliffe OJ, Maskell NA. Spontaneous pneumothorax. BMJ. 2014;348:g2216. — Search PubMed
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Pleural Effusion. Each link opens a live PubMed query.
- Pleural effusion Light's criteria
- Malignant pleural effusion management
- Pleural empyema fibrinolytic treatment
- Indwelling pleural catheter malignant effusion
- Tuberculous pleuritis adenosine deaminase
- Thoracentesis ultrasound guidance
- Heart failure pleural effusion
- Hepatic hydrothorax cirrhosis
- Pulmonary embolism pleural effusion
- Chylothorax thoracic duct management
Connections
- Pulmonology
- Heart Failure
- Pulmonary Embolism
- Pneumonia
- Pulmonary Hypertension
- Lung Cancer
- Pulmonary Fibrosis
- Pneumothorax
- Cirrhosis