Chest Pain
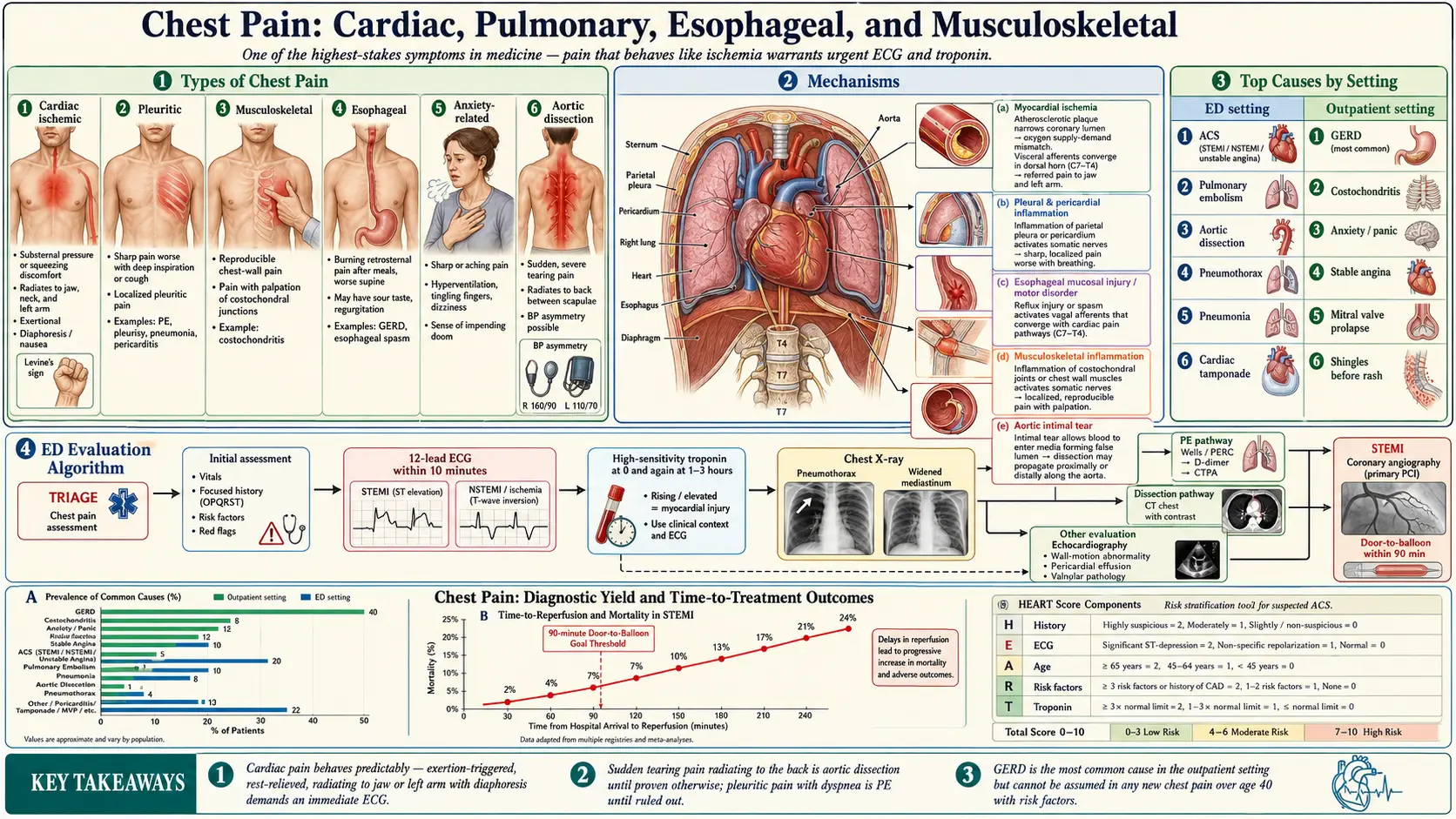

Table of Contents
- Overview
- Types of Chest Pain
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Chest pain is one of the most common reasons for emergency-department visits and one of the highest-stakes symptoms in medicine, because the same complaint can mean a paper cut or a heart attack. Most chest pain is benign — muscle strain, anxiety, or reflux — but a meaningful minority signals an acute coronary syndrome, pulmonary embolism, aortic dissection, or other life threat. The clinically useful distinction is not what chest pain feels like (cardiac pain is famously variable) but how it behaves: pain that comes on with exertion and resolves with rest, with diaphoresis or radiation to the jaw or left arm, in someone with cardiovascular risk factors, deserves urgent evaluation regardless of the descriptor.
Types of Chest Pain
- Cardiac ischemic pain (angina, myocardial infarction) — pressure or tightness, often substernal, with radiation to jaw, neck, or left arm; provoked by exertion or stress; relieved (at first) by rest or nitroglycerin.
- Pleuritic pain — sharp, worse with deep breath or cough; suggests pulmonary embolism, pleurisy, pneumonia, pericarditis.
- Musculoskeletal pain — reproducible with palpation or movement; costochondritis, rib injury, muscle strain.
- Esophageal pain — burning, often after meals or lying down; may be indistinguishable from cardiac pain.
- Anxiety-related pain — sharp or aching, often with hyperventilation, paresthesias, panic; often resolves with breathing slowing.
- Aortic dissection pain — tearing, ripping pain that radiates to the back; sudden onset; surgical emergency.
Common Causes
- Coronary artery disease and acute coronary syndromes — stable angina, unstable angina, NSTEMI, STEMI.
- Heart failure and cardiomyopathy — chest discomfort with shortness of breath, exercise intolerance.
- Pericarditis and myocarditis — sharp pleuritic chest pain, worse supine, better leaning forward.
- Aortic dissection — sudden tearing pain, blood-pressure asymmetry between arms; surgical emergency.
- Pulmonary embolism — pleuritic chest pain, dyspnea, tachycardia, possible hemoptysis.
- Pneumothorax — sudden unilateral pleuritic pain with dyspnea.
- Pneumonia and pleurisy — pleuritic pain with fever, cough, abnormal lung exam.
- GERD and esophageal spasm — burning chest pain, especially after meals or supine; often the most common cause in the outpatient setting.
- Costochondritis and Tietze syndrome — reproducible chest-wall tenderness; benign.
- Panic and anxiety — chest tightness with hyperventilation and tingling.
- Mitral valve prolapse — common, usually benign source of palpitations and atypical chest pain.
- Herpes zoster (shingles) before rash — unilateral dermatomal pain.
Mechanisms
- Myocardial ischemia — oxygen demand exceeds supply because of obstructive coronary disease or coronary vasospasm; visceral afferents converge with somatic dermatomes, producing referred pain to jaw, neck, and arm.
- Pleural and pericardial inflammation — sensitive parietal surfaces produce sharp, position- and breath-dependent pain.
- Esophageal mucosal injury and motor disorders — acid exposure or spasm activates vagal and spinal afferents that share central pathways with cardiac afferents, explaining clinical overlap.
- Musculoskeletal inflammation or strain — well-localized somatic pain, reproducible with palpation.
- Aortic intimal tear — abrupt, severe, tearing pain from dissection plane propagation.
Evaluation
- History — onset, character, radiation, provoking and relieving factors, associated symptoms (dyspnea, diaphoresis, syncope), risk factors (age, smoking, diabetes, family history), recent surgery or immobility (PE risk).
- 12-lead ECG — first test in any concerning chest pain; repeat if pain changes.
- High-sensitivity troponin — serial measurements at presentation and 1–3 hours; cornerstone of MI diagnosis.
- Chest X-ray — rule out pneumothorax, pneumonia, widened mediastinum (dissection).
- D-dimer plus CT pulmonary angiogram — if PE is suspected by Wells / PERC criteria.
- CT chest with contrast — if aortic dissection is suspected.
- Echocardiogram — for wall-motion abnormalities, pericardial effusion, valvular disease.
- Stress testing or coronary CT angiography — for stable, intermediate-risk chest pain in the outpatient setting.
- Coronary angiography — gold standard for high-risk presentations; emergent for STEMI.
- Esophageal evaluation — if non-cardiac chest pain persists; pH-impedance, manometry, upper endoscopy.
Management
- STEMI — immediate primary PCI within 90 minutes of first medical contact; aspirin, P2Y12 inhibitor, anticoagulation, beta-blocker, statin.
- NSTEMI / unstable angina — aspirin, P2Y12 inhibitor, anticoagulation, early invasive strategy in high-risk patients.
- Stable angina — lifestyle (smoking cessation, exercise, Mediterranean diet), statin, antiplatelet, beta-blocker, nitrates as needed; revascularization for refractory or anatomically high-risk disease.
- Pulmonary embolism — anticoagulation; thrombolytics or thrombectomy in massive or sub-massive PE.
- Aortic dissection — immediate surgical repair (Type A) or aggressive blood-pressure control (Type B).
- GERD — PPI, lifestyle measures, weight loss; consider fundoplication if refractory.
- Costochondritis — NSAIDs, reassurance, rest.
- Anxiety / panic disorder — CBT, SSRIs, breathing retraining.
When to Seek Medical Care
- Crushing, squeezing, or pressure-like chest pain — especially with shortness of breath, sweating, nausea, or radiation to jaw, neck, or left arm. Call 911.
- Sudden severe tearing pain radiating to the back, particularly with hypertension or known aneurysm.
- Chest pain with sudden severe dyspnea, low oxygen saturation, or unilateral leg swelling (suspect PE).
- Loss of consciousness or near-syncope during chest pain.
- Chest pain in a patient with known coronary disease that is more frequent, more severe, or occurring at rest.
- Pleuritic chest pain with fever, productive cough, or recent surgery.
- Any new chest pain in a patient over 40 with cardiovascular risk factors that has not been previously evaluated.
Connections
- Pulmonary Embolism
- Anxiety
- Cardiomyopathy
- Coronary Artery Disease
- Heart Failure
- Pneumonia
- GERD
- Shortness of Breath
- Hypertension
- Heart Palpitations
- Myocarditis
- Arrhythmia
- Reflux
- Inflammatory Markers
- Cardiovascular Disease
- Sickle Cell Disease
- Tuberculosis
- Dizziness
References & Research
Historical Background
The systematic study of chest pain dates to William Heberden's 1768 description of "angina pectoris." The 20th century brought the ECG (Einthoven, 1903), troponin assays in the 1990s, and the concept of door-to-balloon time in primary PCI. The 2021 AHA/ACC chest pain guideline replaced "atypical/typical" terminology with risk-stratified pathways, recognizing that women, the elderly, and diabetics often present with non-classic ischemic symptoms.
Key Research Papers
- Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain. Circulation. 2021;144(22):e368-e454.
- Reichlin T, Twerenbold R, Reiter M, et al. Introduction of high-sensitivity troponin assays. New England Journal of Medicine. 2009;361(9):858-867.
- Lee TH, Goldman L. Evaluation of the patient with acute chest pain. New England Journal of Medicine. 2000;342(16):1187-1195.
- Collet JP, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal. 2021;42(14):1289-1367.
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism. European Heart Journal. 2020;41(4):543-603.
- Fanaroff AC, Rymer JA, Goldstein SA, Simel DL, Newby LK. Does this patient with chest pain have acute coronary syndrome? JAMA. 2015;314(18):1955-1965.
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation. 2010;121(13):e266-e369.
- Hellenkamp K, Kaeberich A, Schwung J, et al. Risk stratification and management of intermediate-risk acute pulmonary embolism. Journal of the American College of Cardiology. 2017;69(12):1536-1544.
- Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features, and Rome IV. Gastroenterology. 2016;150(6):1262-1279.
- Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327(7):662-675.
PubMed Topic Searches
- Chest pain evaluation in the emergency department
- High-sensitivity troponin rule-out pathways
- Coronary CT angiography for chest pain
- Pulmonary embolism diagnosis
- Aortic dissection management
- Non-cardiac chest pain (esophageal)