Fatigue
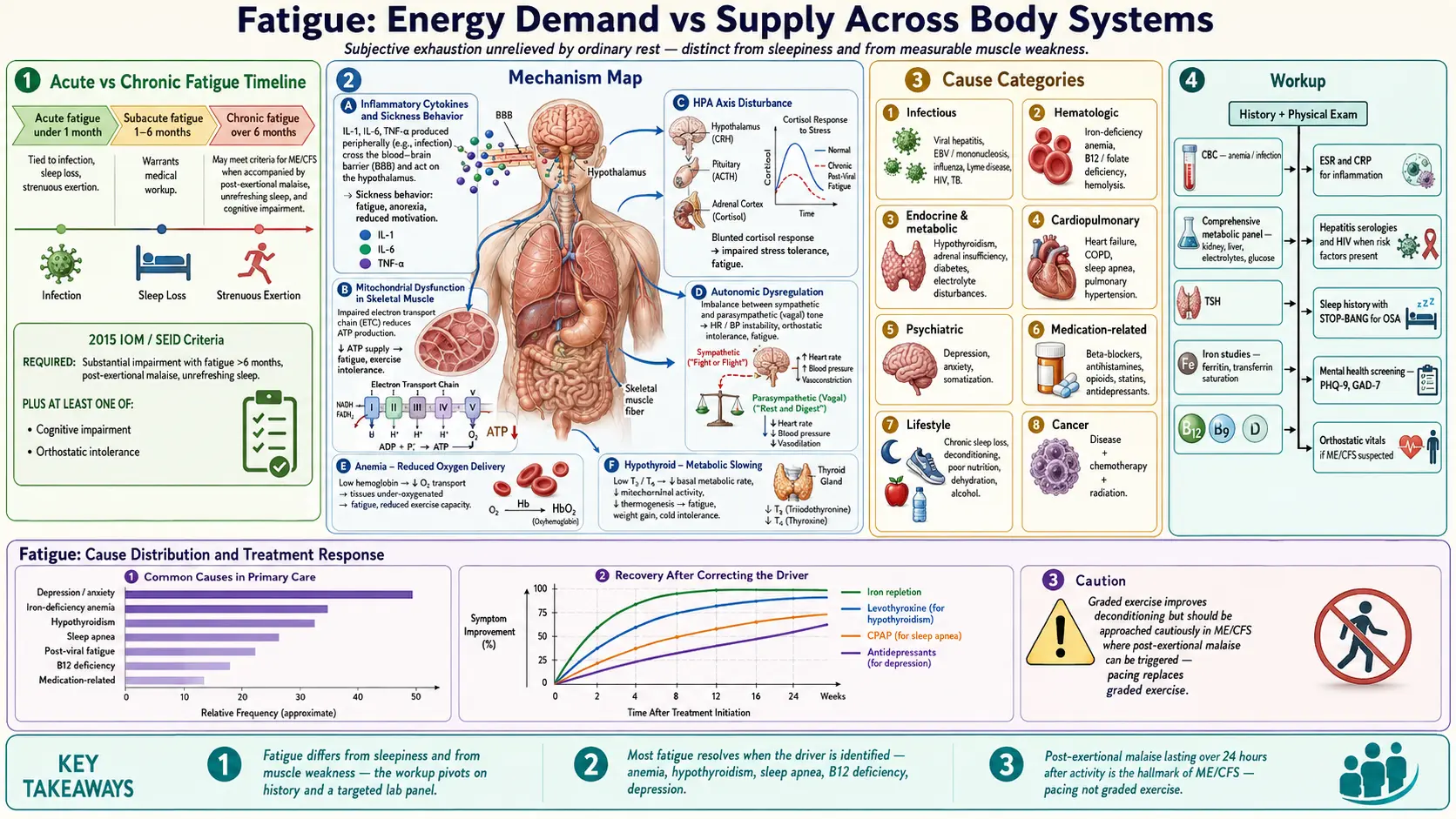

Table of Contents
- Overview
- Evaluating Fatigue — Red Flags vs Common Causes
- Medical Causes — Endocrine
- Medical Causes — Cardiac and Pulmonary
- Medical Causes — Infectious and Hematologic
- Medical Causes — Rheumatologic and Other
- Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS)
- Diagnostic Workup
- Treatment by Cause
- Connections
- References & Research
- Featured Videos
Overview
Fatigue is one of the most common presenting complaints in primary care, accounting for 20–30% of general practitioner visits across all age groups. It is a subjective feeling of tiredness, lack of energy, or exhaustion that is not relieved by ordinary rest. Clinically, it is important to distinguish fatigue from three overlapping symptoms: sleepiness (a compelling desire to fall asleep, primarily driven by sleep debt or circadian disruption), weakness (a measurable reduction in muscle force generation, as in myopathy or neuromuscular disease), and dyspnea (effort limitation due to breathlessness, as in heart failure or COPD). Patients often conflate these, and targeted history-taking is required to separate them, because each implies a different differential diagnosis and workup.
Normal fatigue is physiologically expected after strenuous exertion, sleep deprivation, or acute illness — it resolves with adequate rest, is proportionate to the precipitating cause, and does not impair baseline function once recovery is complete. Pathological fatigue is disproportionate to any recent activity, persists despite adequate rest, and meaningfully impairs occupational performance, social function, or activities of daily living. The onset of pathological fatigue, its relationship to exertion (including delayed worsening 24–48 hours post-activity — post-exertional malaise), associated symptoms, and time course are the most critical history elements.
Fatigue is classified by duration: acute (<1 month), subacute (1–6 months), and chronic (>6 months). The differential diagnosis shifts substantially across these categories. Acute fatigue is usually infectious, medication-related, or stress-driven. Chronic fatigue has a broader differential that includes psychiatric disorders (depression is the single most common cause in primary care, accounting for approximately 40% of unselected chronic fatigue cases), sleep disorders (particularly obstructive sleep apnea), metabolic and endocrine disease, rheumatologic conditions, chronic infections, and — when criteria are met after exclusion of other causes — myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS).
Evaluating Fatigue — Red Flags vs Common Causes
Red Flags Requiring Urgent Evaluation
- Weight loss ≥10% of body weight combined with fatigue — raises concern for malignancy, tuberculosis, or HIV until proven otherwise
- Lymphadenopathy — suggests lymphoma, HIV, or infectious mononucleosis; assess node size, firmness, and distribution
- Organomegaly — hepatosplenomegaly points toward lymphoma, leukemia, or chronic hepatic disease
- Night sweats — classic "B symptoms" of lymphoma; also seen in TB, HIV, and other chronic infections
- Unexplained fever — infectious etiology, malignancy, or autoimmune disease
- Anemia on CBC — hemolysis, occult GI blood loss, bone marrow failure, or infiltration
- Neurological symptoms (diplopia, limb weakness, ataxia, cognitive decline) — multiple sclerosis, myasthenia gravis, or CNS disease
- Cardiac symptoms (exertional chest pain, syncope, orthopnea, edema) — heart failure or valvular disease
- Age >50 with new-onset fatigue — malignancy must be excluded before attributing fatigue to a benign cause
Most Common Causes in Primary Care
- Psychological and psychiatric disorders (approximately 40%) — depression is the single most common cause of chronic fatigue in primary care; anxiety disorders, burnout, and adjustment disorder are also prevalent; always screen with PHQ-9 and GAD-7
- Sleep disorders — obstructive sleep apnea is the most under-recognized cause, particularly in middle-aged men; also insomnia, shift-work disorder, and restless legs syndrome; Epworth Sleepiness Scale (ESS) score >10 is highly suggestive of significant sleep-disordered breathing
- Anemia — iron deficiency is most common, especially in premenopausal women with heavy menstrual bleeding; check CBC plus ferritin; occult GI blood loss must be considered in all adults
- Hypothyroidism — affects 2–4% of women; even subclinical hypothyroidism (TSH 4.5–10 mIU/L with normal free T4) can cause significant fatigue; TSH is the single best screening test
- Medications — beta-blockers, first-generation antihistamines, benzodiazepines, opioids, statins (via myopathy), antiepileptics, antipsychotics, and chemotherapy agents are common culprits; medication reconciliation is an essential step in every fatigue workup
- Lifestyle factors — physical deconditioning, chronic sleep deprivation (<7 hours/night), poor nutritional intake, and alcohol use disorder all produce significant fatigue that can mimic pathological causes
Medical Causes — Endocrine
Hypothyroidism is a cardinal cause of fatigue and is frequently missed because its onset is gradual. The classic constellation includes fatigue, cold intolerance, weight gain, constipation, dry skin, hair thinning, periorbital puffiness, and bradycardia. Even subclinical hypothyroidism — defined as an elevated TSH (4.5–10 mIU/L) with a normal free T4 — causes fatigue and cognitive slowing in a substantial proportion of patients. Diagnosis: TSH as initial screen; add free T4 if TSH is abnormal. Treatment: levothyroxine, with dose titrated to a goal TSH of 0.5–2.5 mIU/L; energy improvement typically requires 6–8 weeks at target dose. Some patients report superior symptom control with combined T4 + T3 (liothyronine) therapy, though evidence from randomized trials is mixed.
Adrenal insufficiency presents with profound, often disabling fatigue accompanied by hyperpigmentation (primary adrenal insufficiency only — caused by excess ACTH stimulating melanocortin receptors in skin), orthostatic hypotension, hyponatremia, and hyperkalemia. Secondary adrenal insufficiency (from pituitary disease or glucocorticoid withdrawal) lacks hyperpigmentation but is otherwise similar. Diagnosis: morning cortisol (8 AM); if borderline (3–18 mcg/dL), confirm with ACTH stimulation test (cosyntropin 250 mcg IV). Addisonian crisis risk is substantial during intercurrent illness — patients require sick-day glucocorticoid doubling rules and an emergency injectable kit.
Diabetes mellitus causes fatigue through multiple mechanisms: hyperglycemia impairs cellular energy metabolism directly, while hypoglycemic episodes (in treated patients) cause acute profound fatigue. The classic triad of polyuria, polydipsia, and fatigue in a patient with risk factors (obesity, family history, age >45) should prompt immediate glucose and A1c testing. Even well-controlled diabetes can cause fatigue through recurrent hypoglycemia, autonomic neuropathy, or sleep disruption from nocturia.
Hypercalcemia causes the classically described constellation of "bones, groans, moans, and stones" — fatigue, constipation, polyuria, nephrolithiasis, and bone pain. Mild hypercalcemia (10.5–12 mg/dL) commonly presents with fatigue alone. The two most common causes in outpatients are primary hyperparathyroidism and malignancy. Diagnosis: total calcium (corrected for albumin) + intact PTH; PTH-independent hypercalcemia (low PTH, elevated calcium) points toward malignancy or granulomatous disease.
Male hypogonadism (low testosterone) manifests as fatigue, reduced libido, mood disturbances (depression-like), reduced muscle mass, and increased adiposity. Prevalence rises with age; also common in men with chronic illness, opioid use, or obesity. Diagnosis: morning total testosterone (8–10 AM; repeat if borderline); confirm with LH and FSH to distinguish primary (testicular) from secondary (pituitary) hypogonadism.
Cushing's syndrome paradoxically combines fatigue with symptoms of cortisol excess: truncal obesity, easy bruising, purple abdominal striae, proximal muscle weakness, hypertension, hyperglycemia, and osteoporosis. Screening tests include 24-hour urine free cortisol, late-night salivary cortisol (two measurements), and low-dose (1 mg) overnight dexamethasone suppression test. Fatigue in Cushing's is likely mediated by sleep disruption, metabolic derangements, and HPA axis dysregulation.
Medical Causes — Cardiac and Pulmonary
Heart failure is a major cause of exertional fatigue, classically accompanied by dyspnea (especially orthopnea and paroxysmal nocturnal dyspnea), dependent edema, and reduced exercise tolerance. NT-proBNP or BNP is the best initial biomarker; echocardiogram characterizes systolic vs. diastolic dysfunction, ejection fraction, and valvular disease. Treatment follows the HFrEF (reduced ejection fraction) guideline-directed medical therapy framework: loop diuretics for volume overload, ACEi/ARB/ARNI (sacubitril-valsartan), beta-blockers (carvedilol, metoprolol succinate), and mineralocorticoid antagonists (spironolactone, eplerenone).
Valvular heart disease — particularly aortic stenosis — produces the classic triad of exertional fatigue, syncope (or pre-syncope), and exertional chest pain. Severe AS is a hemodynamic emergency; mean gradient >40 mmHg on echo with reduced valve area (<1.0 cm²) requires intervention. Mitral regurgitation causes volume-overload fatigue with a characteristic holosystolic murmur radiating to the axilla. Echocardiography is diagnostic for all valvular lesions.
Obstructive sleep apnea (OSA) is arguably the most under-recognized cause of chronic fatigue, especially in middle-aged men. Key features: loud snoring, witnessed apneas by bed partner, nocturia, morning headaches, and unrefreshing sleep. The Epworth Sleepiness Scale (ESS score >10) and STOP-BANG questionnaire (≥3 points: high risk) are validated screening tools. Polysomnography (PSG) is the gold standard; home sleep apnea testing is appropriate for high-pretest-probability patients without significant comorbidities. CPAP is first-line treatment; 10% weight loss can eliminate OSA in overweight patients; mandibular advancement devices are effective for mild-to-moderate OSA in patients who cannot tolerate CPAP.
COPD causes fatigue through multiple mechanisms: impaired gas exchange, increased work of breathing, systemic inflammation, and deconditioning. Spirometry showing FEV1/FVC <0.70 post-bronchodilator is diagnostic. Fatigue in COPD correlates more strongly with exercise capacity (6-minute walk distance) than with FEV1 alone.
Pulmonary arterial hypertension (PAH) presents insidiously with exertional fatigue, progressive dyspnea, and ultimately syncope. Mean age at diagnosis is 50–65 years; female predominance. Estimated right ventricular systolic pressure >40 mmHg on echo warrants right heart catheterization for confirmation (mPAP ≥20 mmHg). Treatment includes pulmonary vasodilators (phosphodiesterase-5 inhibitors, endothelin receptor antagonists, prostacyclin analogs).
Medical Causes — Infectious and Hematologic
Anemia produces fatigue through reduced oxygen-carrying capacity — pallor, exertional dyspnea, palpitations, and tachycardia accompany the fatigue in moderate-to-severe cases. The specific type determines evaluation and treatment. Iron deficiency anemia (IDA): microcytic MCV <80 fL + ferritin <30 ng/mL; most common in premenopausal women (menstrual loss) and in GI blood loss; do not assume IDA is dietary in men or postmenopausal women without colonoscopy. Vitamin B12 deficiency: macrocytic MCV >100 fL; subacute combined degeneration of the spinal cord (posterior columns + corticospinal tracts) in severe cases; check methylmalonic acid and homocysteine if B12 is borderline (200–400 pg/mL). Anemia of chronic disease (ACD): normocytic, low serum iron, but elevated ferritin and transferrin saturation <20%; occurs in chronic infections, autoimmune disease, and malignancy; treat the underlying condition; IV iron or erythropoiesis-stimulating agents (ESAs) per disease-specific guidelines.
Infectious mononucleosis (EBV) is the classic post-infectious fatigue syndrome in adolescents and young adults (peak age 15–25). The triad of fever, exudative pharyngitis, and cervical lymphadenopathy with splenomegaly is typical. Splenic rupture (rare but life-threatening) mandates avoidance of contact sports until spleen normalizes by ultrasound. Diagnosis: monospot (heterophile antibody) — false-negative rate 10–15% in first week; EBV VCA IgM is more sensitive. Post-viral fatigue lasting 4–6 weeks after acute illness is typical and expected; fatigue persisting >6 months may represent transition to ME/CFS in susceptible individuals.
HIV should be screened in all adults aged 15–64 at least once (CDC recommendation), and in any patient with unexplained fatigue regardless of perceived risk. The 4th-generation HIV Ag/Ab combination test detects both p24 antigen and HIV antibodies — sensitivity exceeds 99.9% at 4 weeks post-exposure. Acute HIV (primary infection, 2–4 weeks post-exposure) can present as a mononucleosis-like illness with fever, pharyngitis, lymphadenopathy, rash, and profound fatigue — a presentation often initially misdiagnosed.
Chronic hepatitis C is often asymptomatic for decades, but fatigue is the most commonly reported symptom and may precede detectable liver fibrosis. Risk factors: intravenous drug use (historical or current), blood transfusion before 1992, tattoos with non-sterile equipment, or birth between 1945–1965 (baby boomer screening cohort). Diagnosis: anti-HCV antibody → confirmatory HCV RNA if antibody positive. Effective treatment with direct-acting antivirals (DAAs) achieves sustained virologic response (SVR, functional cure) in >95% of treated patients, with significant improvement in fatigue scores post-SVR.
Tuberculosis can present with fatigue as a prominent early symptom before pulmonary symptoms develop, particularly in immunocompromised patients, immigrants from high-burden countries, and incarcerated individuals. The classic triad: night sweats, weight loss, and productive cough ± hemoptysis. Screening: TST (tuberculin skin test) or IGRA (interferon-gamma release assay, e.g., QuantiFERON-TB Gold Plus). Active TB: chest CT + sputum AFB smear/culture/NAAT (Xpert MTB/RIF).
Lyme disease in the early disseminated phase can produce fatigue, arthralgias, and neurological symptoms (Lyme neuroborreliosis). Fatigue without a prior erythema migrans rash or tick exposure history should be worked up carefully before attributing to Lyme. Diagnosis: two-tier serologic testing (ELISA followed by Western blot); false-positive ANA and rheumatoid factor can confuse the picture. Post-Lyme disease syndrome — persistent fatigue after adequately treated Lyme — is a recognized entity but remains clinically controversial; evidence does not support prolonged antibiotic courses.
Medical Causes — Rheumatologic and Other
Systemic lupus erythematosus (SLE): fatigue is present in >90% of SLE patients and is often the most debilitating symptom — more disabling than arthritis or rash in many patients' self-reported experience. SLE fatigue is multifactorial: disease activity, anemia, depression, fibromyalgia overlap, sleep disruption, and medication effects all contribute. Screening: ANA (sensitivity >95% for SLE, but low specificity); if ANA positive or clinical suspicion high, add anti-dsDNA, anti-Sm, complement C3/C4, CBC, urinalysis with microscopy.
Rheumatoid arthritis (RA): fatigue is a dominant complaint even when joint disease is well-controlled, affecting 70–80% of RA patients. Mechanisms include systemic inflammation (elevated TNF-alpha, IL-6), anemia of chronic disease, pain-disrupted sleep, and depression. Initial workup: RF, anti-CCP antibodies (more specific than RF), ESR, CRP, CBC. Symmetric small joint involvement with morning stiffness exceeding one hour is the classic presentation.
Fibromyalgia: diffuse musculoskeletal pain + fatigue + unrefreshing sleep + cognitive symptoms ("fibro fog" — slowed processing, working memory difficulties) + multiple somatic complaints without objective inflammation. No diagnostic lab abnormality — diagnosis is clinical. The 2016 ACR criteria require widespread pain (>3 months, multiple body regions) plus symptom severity scale. Fibromyalgia overlaps significantly with ME/CFS, depression, and irritable bowel syndrome; presence of one does not exclude the others.
Chronic kidney disease (CKD): uremic fatigue (from nitrogenous waste accumulation) + fatigue from reduced erythropoietin production → normocytic anemia. eGFR <30 mL/min/1.73m² is associated with significant fatigue burden. Anemia of CKD responds to ESA therapy (epoetin alfa, darbepoetin alfa) when Hgb <10 g/dL, per KDIGO guidelines; target Hgb 10–11.5 g/dL to avoid cardiovascular risk from over-correction.
Celiac disease: fatigue + GI symptoms (diarrhea, bloating, abdominal pain) + iron deficiency anemia unresponsive to oral iron replacement should raise suspicion. Malabsorption of iron, B12, folate, and vitamin D all contribute to fatigue. Diagnosis: anti-tissue transglutaminase IgA (TTG-IgA) + total IgA (to exclude IgA deficiency as a false-negative cause); confirm with small bowel biopsy (Marsh III lesions). A gluten-free diet results in dramatic energy improvement in confirmed celiac disease.
Medication-induced fatigue is extremely common and underappreciated. Major culprits: beta-blockers (reduce cardiac output response to exercise); first-generation antihistamines (diphenhydramine, hydroxyzine — cross the blood-brain barrier); benzodiazepines (especially long-acting — diazepam); opioids; statins (can cause myopathy with elevated CK — check if patient reports muscle-related fatigue); antiepileptics (carbamazepine, valproate, topiramate); antipsychotics; interferon-based therapies; chemotherapy and hormonal cancer therapies (aromatase inhibitors, androgen deprivation). Medication reconciliation must be systematic in every fatigue workup.
Depression and anxiety: fatigue is a DSM-5 criterion for major depressive disorder and is present in nearly all depressed patients. It is both a symptom of the mood disorder and a consequence of the sleep disruption, autonomic arousal, and HPA dysregulation that depression produces. PHQ-9 score ≥10 has 88% sensitivity for major depression in primary care. Anxiety disorders produce fatigue through chronic sympathetic activation, hyperarousal-driven poor sleep, and energy depletion from constant worry. Treating the mood disorder often resolves the fatigue — but fatigue can also persist as a residual symptom requiring additional intervention.
Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS)
ME/CFS is a serious, complex, multi-system illness characterized by profound fatigue that does not improve with rest and that is worsened by exertion. Its pathophysiology is incompletely understood but increasingly recognized as involving genuine biological dysfunction — not a functional or psychosomatic disorder. Prevalence: 0.8–2.5% of the general population; three times more common in females; peak onset in the 20s–40s, though all ages are affected. The illness frequently begins after an infectious trigger.
Post-infectious onset: ME/CFS often follows a viral illness — historically, Epstein-Barr virus, enteroviruses, and HTLV were most commonly implicated. Long COVID (post-COVID syndrome) has dramatically expanded the ME/CFS patient population: 10–20% of COVID-19 survivors develop long COVID, and a substantial subset meet formal ME/CFS criteria — making COVID-19 the most impactful ME/CFS trigger in history. Other infections (Q fever, Giardia, Ross River virus) have also been documented as triggers in epidemiological studies.
2015 IOM / SEID diagnostic criteria (all four required):
- Substantial reduction or impairment in the ability to engage in pre-illness levels of occupational, educational, social, or personal activities, lasting more than 6 months, accompanied by fatigue that is not the result of ongoing excessive exertion and is not substantially alleviated by rest
- Post-exertional malaise (PEM) — the cardinal hallmark: a worsening of ALL symptoms after minimal physical or cognitive exertion, often delayed 12–48 hours, that can last days to weeks and is severe enough to be temporarily debilitating. PEM distinguishes ME/CFS from depression, deconditioning, and most other fatigue states; patients often describe it as a "crash" or "relapse"
- Unrefreshing sleep — patients wake feeling as exhausted as before sleep; sleep study findings may show reduced deep sleep and increased light sleep stages, or alpha-wave intrusion
- Cognitive impairment ("brain fog") — reduced information processing speed, working memory deficits, word-finding difficulties, difficulty concentrating — OR orthostatic intolerance — worsening of symptoms upon standing, lightheadedness, palpitations, near-syncope, consistent with dysautonomia or POTS-like physiology; tested with the NASA lean test or formal tilt-table test
Proposed pathophysiology: research increasingly points toward mitochondrial dysfunction (impaired oxidative phosphorylation + reduced ATP production, documented by 2-day CPET showing abnormal VO2 and anaerobic threshold on day 2 despite normal day 1 — the "2-day CPET" signature); immune dysregulation (NK cell functional deficiency, cytokine network abnormalities, possible autoantibodies against adrenergic and muscarinic receptors); autonomic nervous system dysfunction (reduced baroreflex sensitivity, POTS-like features in up to 30%); HPA axis abnormalities (blunted cortisol response); and gut microbiome disruption (reduced microbial diversity, increased intestinal permeability).
Treatment — no curative therapy exists; management is supportive and symptom-targeted:
- Pacing — the most important intervention: activity pacing within the "energy envelope" to avoid PEM triggers; heart rate monitoring (keeping HR below anaerobic threshold, approximately 60% of max HR or 220-age) to guide activity; "stop before symptoms start" principle
- Graded Exercise Therapy (GET) is contraindicated for patients with PEM — GET was previously recommended based on the now-discredited "perpetuating fear-avoidance" model; the 2021 NICE guideline NG206 explicitly removed GET from recommendations after evidence showed it worsens outcomes in ME/CFS patients with PEM
- Orthostatic intolerance: increased salt intake (8–10 g/day); increased fluid intake (3 L/day); compression garments (waist-high); pharmacological options — fludrocortisone, beta-blockers (propranolol low-dose), ivabradine (particularly for inappropriate sinus tachycardia), midodrine for hypotension-predominant dysautonomia
- Sleep management: sleep hygiene; low-dose tricyclics (amitriptyline 10–25 mg) or cyclobenzaprine for sleep quality; melatonin with attention to circadian timing; avoid daytime sleeping beyond short rests (limits nighttime sleep quality)
- Low-dose naltrexone (LDN): emerging evidence — 1.5–4.5 mg at bedtime; proposed mechanism is transient opioid receptor antagonism triggering upregulation of endogenous opioids + glial modulation (reduced microglial activation); multiple open-label studies and patient registries show improvement in pain, fatigue, and cognitive symptoms; randomized controlled trials underway
- Rintatolimod (Ampligen): double-stranded RNA immunomodulator; shown improvement in exercise tolerance in two randomized trials; FDA expedited review; limited availability in research settings
- Pain management: duloxetine (for fatigue + pain in overlapping fibromyalgia); low-dose naltrexone; gabapentin cautiously (sedation can worsen fatigue)
- Cognitive symptoms: modafinil used off-label with variable benefit; cognitive rehabilitation adapted for energy limitations; pacing of cognitive tasks parallels physical pacing
Diagnostic Workup
Initial Panel (all patients with fatigue >2 weeks)
- CBC with differential — anemia, leukopenia (SLE, viral), lymphocytosis (EBV, viral), thrombocytopenia
- Ferritin — most sensitive single test for iron deficiency; ferritin <30 ng/mL diagnostic of iron depletion even with normal Hgb
- TSH — primary thyroid screening; if elevated, add free T4
- Basic metabolic panel (BMP) — electrolytes, glucose, calcium, creatinine, BUN
- Liver function tests (LFTs) — AST, ALT, alkaline phosphatase, total bilirubin
- Urinalysis — proteinuria (CKD, SLE), glucosuria (DM), hematuria (malignancy)
- HIV 4th-generation Ag/Ab combination test — all adults 15–64 per CDC
- ESR and CRP — elevated in inflammatory, infectious, and malignant conditions
- Hemoglobin A1c — diabetes screening in patients >45 years or with overweight/obesity/family history
- Vitamin B12 and folate — macrocytic anemia, neurological symptoms, vegans/vegetarians
- ANA — screening for connective tissue disease in women with fatigue + systemic symptoms
Second-Tier Testing (targeted by clinical suspicion)
- Morning cortisol (8 AM) ± ACTH stimulation test — adrenal insufficiency suspected (hyperpigmentation, hyponatremia, hypotension)
- PPD/IGRA (QuantiFERON-TB Gold) — TB risk factors present
- HCV antibody — risk factors for hepatitis C (IVDU, transfusion before 1992, birth 1945–1965)
- HBsAg + HBcAb — hepatitis B exposure history or endemic country origin
- Polysomnography (PSG) or home sleep apnea testing — STOP-BANG ≥3 or ESS >10
- Morning total testosterone (8–10 AM) + LH + FSH — men with low libido, mood changes, reduced muscle mass
- Echocardiogram — cardiac symptoms, BNP elevation, or valvular murmur
- Anti-TTG-IgA + total IgA — celiac disease suspected (GI symptoms + iron deficiency refractory to oral replacement)
- EBV VCA IgM and heterophile antibody (monospot) — young adults with pharyngitis + lymphadenopathy
- Free T4 + anti-TPO antibodies — if TSH borderline or Hashimoto's thyroiditis suspected
- PTH + 25-OH vitamin D + urine calcium — if total calcium elevated or hypercalcemia suspected
Psychological Screening
- PHQ-9 — validated 9-item depression screen; score ≥10 warrants diagnostic interview for major depression
- GAD-7 — 7-item generalized anxiety screen; score ≥10 indicates moderate-to-severe anxiety
- Epworth Sleepiness Scale (ESS) — 8-item daytime sleepiness questionnaire; score >10 suggests pathological sleepiness
- STOP-BANG questionnaire — 8-item OSA risk score; ≥3 = high risk for OSA
- Validated burnout screening (Maslach Burnout Inventory) — especially in healthcare workers, first responders, caregivers
- Detailed sleep history — bedtime, wake time, sleep latency, nocturnal awakenings, snoring, witnessed apneas, nocturia
Treatment by Cause
- Iron deficiency anemia: ferrous sulfate 325 mg orally three times daily taken between meals for maximum absorption; ferrous gluconate if GI side effects limit compliance (nausea, constipation); IV iron (ferric carboxymaltose, ferumoxytol, low-molecular-weight iron dextran) for malabsorption, intolerance, or rapid repletion needed; always identify and treat the source of blood loss — do not assume dietary cause in men or postmenopausal women
- Hypothyroidism: levothyroxine 1.6 mcg/kg/day as starting dose (lower — 25–50 mcg/day — in elderly or cardiac disease); titrate by TSH every 6–8 weeks; goal TSH 0.5–2.5 mIU/L; full energy improvement typically requires 6–8 weeks at therapeutic dose; consider adding low-dose liothyronine (T3) for patients with persistent fatigue despite normal TSH on T4 monotherapy
- Obstructive sleep apnea: CPAP is first-line (AHI reduction >50%); adherence is the critical challenge — ensure mask fitting, consider heated humidification; mandibular advancement device (MAD) for mild-moderate OSA or CPAP intolerance; weight loss 10% can eliminate or significantly improve OSA; positional therapy (sleep position trainer) for purely supine OSA; hypoglossal nerve stimulation (Inspire) for CPAP-refractory moderate-severe OSA
- Depression: SSRIs are first-line (sertraline 50–200 mg, escitalopram 10–20 mg — both well-tolerated, favorable side effect profiles); SNRIs (venlafaxine, duloxetine) for comorbid pain or anxiety; bupropion has activating properties and may preferentially improve fatigue and concentration with less weight gain; aerobic exercise ≥150 minutes/week has evidence-based antidepressant effect comparable to SSRIs in mild-moderate depression and specifically improves fatigue
- ME/CFS: pacing within energy envelope; treat orthostatic intolerance aggressively (salt, fluids, compression, medications as above); LDN 1.5–4.5 mg at bedtime; avoid graded exercise therapy; multidisciplinary care with ME/CFS-knowledgeable providers; connect with patient advocacy organizations (MEAction, Solve ME/CFS Initiative) for peer support and research updates
- Vitamin B12 deficiency: intramuscular cyanocobalamin 1000 mcg daily × 7 days, then weekly × 4 weeks, then monthly (classic schedule for pernicious anemia / malabsorption); alternatively, high-dose oral B12 1000–2000 mcg daily is effective even in pernicious anemia via passive absorption (does not require intrinsic factor at this dose); neurological symptoms may take 6–12 months to partially or fully recover
- Adrenal insufficiency: hydrocortisone 15–20 mg/day in divided doses (e.g., 10 mg morning + 5 mg early afternoon — mimic the natural diurnal cortisol rhythm); fludrocortisone 0.05–0.1 mg daily for primary AI with mineralocorticoid deficiency; sick day rules (double or triple hydrocortisone dose for fever or illness); emergency injectable hydrocortisone 100 mg IM/IV kit for addisonian crisis prevention; MedicAlert bracelet
- Anemia of chronic disease: treat the underlying inflammatory or infectious condition primarily; ESAs (epoetin alfa, darbepoetin alfa) per disease-specific guidelines in CKD (target Hgb 10–11.5 g/dL) and chemotherapy-related anemia; IV iron can improve response to ESAs when transferrin saturation <20% + ferritin <500 ng/mL
- OSA in heart failure: adaptive servo-ventilation (ASV) is contraindicated in HFrEF with central sleep apnea (SERVE-HF trial showed increased mortality); auto-titrating CPAP or bilevel PAP per sleep specialist guidance
- Celiac disease: strict lifelong gluten-free diet; dietitian referral essential; energy improvement typically begins within 4–8 weeks of complete gluten removal; monitor for nutritional deficiencies (iron, B12, folate, D, calcium) and supplement accordingly
Connections
- Anemia
- Depression
- Anxiety
- Chronic Fatigue Syndrome / ME/CFS
- Thyroid Disorders
- Obstructive Sleep Apnea
- Hepatitis C
- Heart Failure
- Diabetes
- Deep Vein Thrombosis
- Lymphoma
- Mononucleosis
- Lupus / SLE
- Fibromyalgia
- Insomnia
- Kidney Disease
- Unexplained Weight Loss
- Night Sweats
- Iron
- Vitamin B12
References & Research
Historical Background
The systematic medical study of fatigue as a distinct clinical entity began in earnest with George Beard's 1869 description of "neurasthenia" — a condition of nervous exhaustion attributed to the demands of modern industrial life. Beard's framework dominated for decades despite lacking mechanistic underpinning. The modern concept of post-viral fatigue crystallized through two pivotal American outbreaks in the mid-1980s: the 1984–1985 Lake Tahoe, Nevada outbreak (initially called "Raggedy Ann syndrome" and erroneously attributed to EBV) and a concurrent Lyndonville, New York outbreak. These outbreaks, combined with a surge in clinical case series, prompted the CDC to convene an expert panel that published the first formal case definition for chronic fatigue syndrome in 1988 (Holmes criteria), subsequently refined in the widely adopted 1994 Fukuda criteria.
The 2015 Institute of Medicine (IOM) report marked the most significant paradigm shift: renaming the condition Systemic Exertion Intolerance Disease (SEID), explicitly recognizing it as a biological illness distinct from psychiatric disorders, and elevating post-exertional malaise as the cardinal diagnostic criterion — a move that simultaneously improved diagnostic specificity and challenged the cognitive behavioral / graded exercise therapy models that had dominated treatment guidelines. The COVID-19 pandemic dramatically accelerated ME/CFS research: with 10–20% of COVID-19 survivors developing long COVID and a significant subset meeting ME/CFS criteria, the patient population expanded by millions globally, attracting NIH RECOVER Initiative funding and renewed scientific urgency. The parallel recognition that identical post-infectious mechanisms may drive both post-COVID and classical ME/CFS has generated the most promising mechanistic research in the field's history.
Key Research Papers
- Fukuda K, Straus SE, Hickie I, et al. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med. 1994;121(12):953-959.
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. National Academies Press. 2015.
- Dantzer R, Heijnen CJ, Kavelaars A, Laye S, Capuron L. The neuroimmune basis of fatigue. Trends Neurosci. 2014;37(1):39-46.
- Afari N, Buchwald D. Chronic fatigue syndrome: a review. Am J Psychiatry. 2004;161(2):221-236.
- Larun L, Brurberg KG, Odgaard-Jensen J, Price JR. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst Rev. 2019;(10):CD003200.
- NICE guideline NG206: Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. National Institute for Health and Care Excellence. 2021.
- Rosenthal TC, Majeroni BA, Pretorius R, Malik K. Fatigue: an overview. Am Fam Physician. Search PubMed
- Mullington JM, Haack M, Toth M, Serrador JM, Meier-Ewert HK. Cardiovascular, inflammatory, and metabolic consequences of sleep deprivation. Prog Cardiovasc Dis. 2009;51(4):294-302.
- Wessely S, Chalder T, Hirsch S, Wallace P, Wright D. Psychological symptoms, somatic symptoms, and psychiatric disorder in chronic fatigue and chronic fatigue syndrome. Am J Psychiatry. 1996;153(8):1050-1059.
- Natelson BH, Haghighi MH, Ponzio NM. Evidence for the presence of immune dysfunction in chronic fatigue syndrome. Clin Diagn Lab Immunol. 2002;9(4):747-752.
- Klimas NG, Koneru AO. Chronic fatigue syndrome: inflammation, immune function, and neuroendocrine interactions. Curr Rheumatol Rep. 2007;9(6):482-487.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133-146.
PubMed Topic Searches
- ME/CFS diagnosis and criteria
- Fatigue evaluation in primary care
- Post-exertional malaise in ME/CFS
- Hypothyroidism and fatigue
- Sleep apnea and fatigue
- Long COVID and fatigue