Jaundice
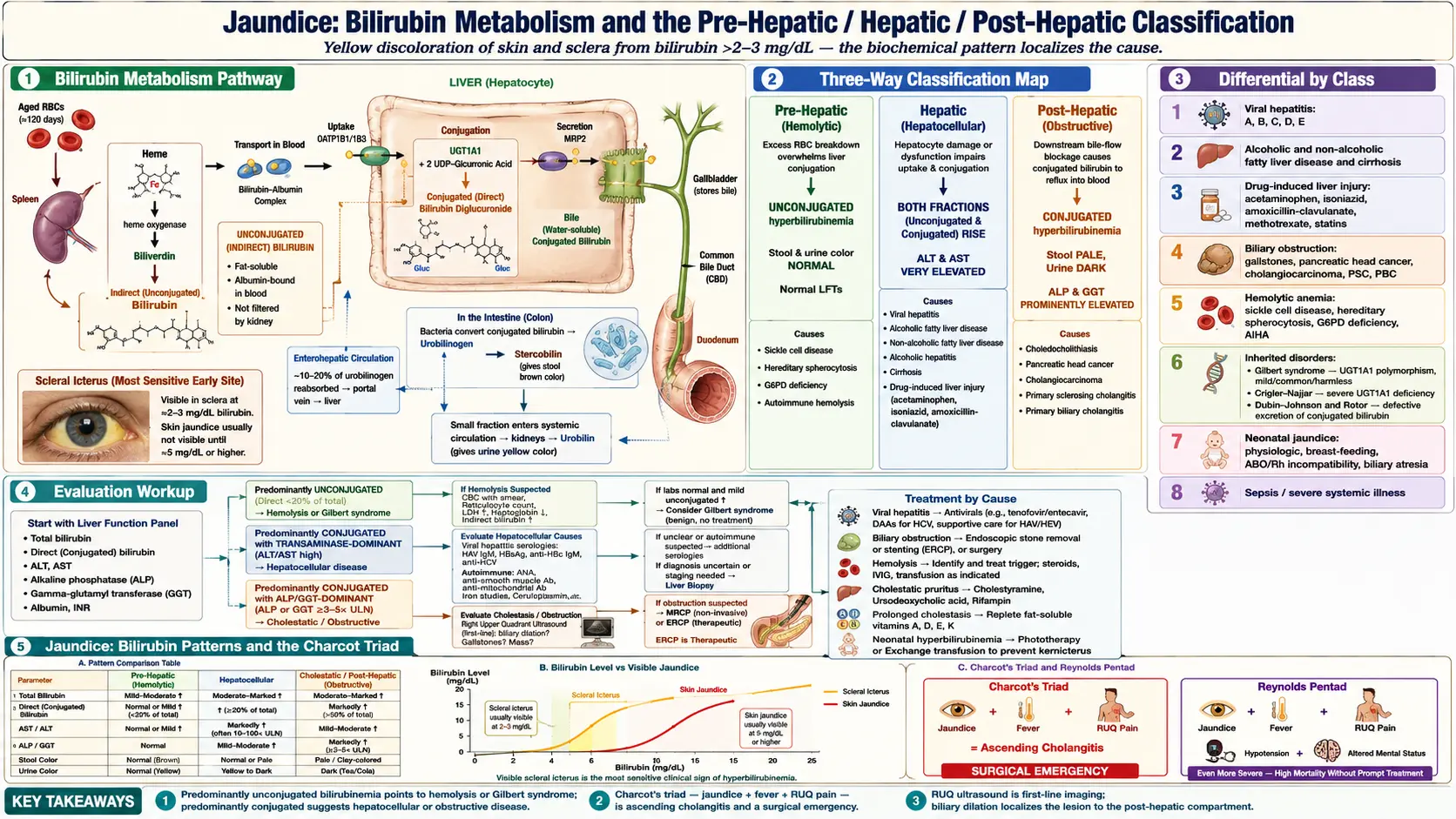
Table of Contents
- Overview
- Bilirubin Metabolism
- Classification
- Common Causes
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Jaundice (also called icterus) is the yellow discoloration of the skin, sclerae, and mucous membranes caused by elevated levels of bilirubin in the bloodstream. Bilirubin is a pigment formed during the normal breakdown of red blood cells; it is processed by the liver and excreted in bile. When any step in this pathway is disrupted, bilirubin accumulates and stains tissues yellow. Visible jaundice typically appears when serum bilirubin exceeds 2-3 mg/dL.
Bilirubin Metabolism
Aged red blood cells are broken down in the spleen, releasing heme. Heme is converted to unconjugated (indirect) bilirubin, which is fat-soluble and bound to albumin in blood. The liver uptakes unconjugated bilirubin and conjugates it with glucuronic acid via the enzyme UGT1A1, producing water-soluble conjugated (direct) bilirubin. This is secreted into bile, passes through the biliary tree into the small intestine, and is converted by gut bacteria into urobilinogen and stercobilin (which gives stool its brown color). Disruption at any of these steps produces jaundice with characteristic biochemical patterns.
Classification
- Pre-hepatic (hemolytic) — excess red cell breakdown overwhelms the liver's conjugation capacity, producing unconjugated hyperbilirubinemia. Stool and urine color are usually normal.
- Hepatic (hepatocellular) — liver cells are damaged or dysfunctional, impairing both uptake and conjugation. Both bilirubin fractions rise; transaminases (ALT, AST) are typically very elevated.
- Post-hepatic (obstructive) — bile flow is blocked downstream from the liver (gallstones, tumors, strictures). Conjugated bilirubin refluxes into blood; alkaline phosphatase and GGT rise prominently. Stool becomes pale and urine darkens.
Common Causes
- Viral hepatitis — hepatitis A, B, C, D, E.
- Alcoholic and non-alcoholic fatty liver disease, alcoholic hepatitis, cirrhosis.
- Drug-induced liver injury — acetaminophen overdose, isoniazid, amoxicillin-clavulanate, methotrexate, statins.
- Biliary obstruction — gallstones (choledocholithiasis), pancreatic head cancer, cholangiocarcinoma, primary sclerosing cholangitis, primary biliary cholangitis.
- Hemolytic anemia — sickle cell disease, hereditary spherocytosis, G6PD deficiency, autoimmune hemolysis.
- Inherited disorders — Gilbert syndrome (mild, common, harmless), Crigler-Najjar, Dubin-Johnson, Rotor syndrome.
- Neonatal jaundice — physiologic, breast-feeding, ABO/Rh incompatibility, biliary atresia.
- Sepsis and severe systemic illness — through multiple mechanisms.
Evaluation
- Liver function panel — total and direct bilirubin, ALT, AST, alkaline phosphatase, GGT, albumin, INR.
- Complete blood count and reticulocyte count — to evaluate for hemolysis.
- Viral hepatitis serologies — HAV IgM, HBsAg, anti-HBc IgM, anti-HCV.
- Autoimmune workup — ANA, anti-smooth muscle, anti-mitochondrial antibodies.
- Right upper quadrant ultrasound — first-line imaging for biliary dilation and gallstones.
- MRCP or ERCP — for suspected obstruction; ERCP allows therapeutic intervention.
- Liver biopsy — when noninvasive workup is inconclusive.
Management
Treatment is directed at the underlying cause. Viral hepatitis may resolve spontaneously or require antiviral therapy; biliary obstruction often needs endoscopic stone removal or stenting; hemolysis requires identification and treatment of the trigger. Severe jaundice can cause itching (treated with cholestyramine, ursodeoxycholic acid, or rifampin), and prolonged cholestasis may impair fat-soluble vitamin absorption (A, D, E, K). Newborns with significant hyperbilirubinemia receive phototherapy or, in extreme cases, exchange transfusion to prevent kernicterus.
When to Seek Medical Care
- Any new yellowing of the skin or eyes in an adult should prompt prompt medical evaluation.
- Jaundice with fever, right upper quadrant pain, and chills (Charcot's triad) suggests ascending cholangitis, a surgical emergency.
- Jaundice with confusion, easy bruising, or abdominal swelling suggests acute liver failure.
- Newborn jaundice within the first 24 hours of life or persisting beyond two weeks.
Connections
- Hepatitis
- Sickle Cell Disease
- Cirrhosis
- Liver Disease
- Pale Stool
- Hepatitis C
- Gallbladder Disease
- Dark Urine
- Hepatitis B
- Milk Thistle
- Non-Alcoholic Fatty Liver Disease
- Anemia
- Sepsis
- GGT
- Complete Blood Count
- Fatigue
- Abdominal Pain
- Urinalysis
- Liver Cancer
- Hepatitis: History and Discovery — how epidemic jaundice was traced to distinct viruses.
- Biliary Atresia — the surgical cause of conjugated newborn jaundice; the Kasai window closes near 60 days.
- Neonatal Jaundice (Neonatal Hyperbilirubinemia) — the newborn form, where rising bilirubin can threaten the brain.
- Hereditary Spherocytosis — an inherited red-cell membrane defect causing lifelong hemolysis with jaundice.
References & Research
Historical Background
Jaundice was recognized in the writings of Hippocrates as a sign of liver illness. The biochemical basis was established in the 19th century when Rudolf Virchow described bilirubin as the yellow pigment of bile, and Hijmans van den Bergh's 1913 diazo reaction allowed clinicians to distinguish conjugated from unconjugated bilirubin — the key step in localizing the cause. The Gilbert syndrome, the most common inherited cause of mild unconjugated hyperbilirubinemia, was described by Augustin Gilbert in 1901.
Key Research Papers
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. New England Journal of Medicine. 2000;342(17):1266-1271.
- Fevery J. Bilirubin in clinical practice: a review. Liver International. 2008;28(5):592-605.
- Roche SP, Kobos R. Jaundice in the adult patient. American Family Physician. 2004;69(2):299-304.
- Beuers U. Drug insight: mechanisms and sites of action of ursodeoxycholic acid in cholestasis. Nature Clinical Practice Gastroenterology & Hepatology. 2006;3(6):318-328.
- American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297-316.
- Wagner M, Trauner M. Recent advances in understanding and managing cholestasis. F1000Research. 2016;5:705.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of cholestatic liver diseases. Journal of Hepatology. 2009;51(2):237-267.
- Bosma PJ, Chowdhury JR, Bakker C, et al. The genetic basis of the reduced expression of bilirubin UDP-glucuronosyltransferase 1 in Gilbert's syndrome. New England Journal of Medicine. 1995;333(18):1171-1175.