Dark Urine
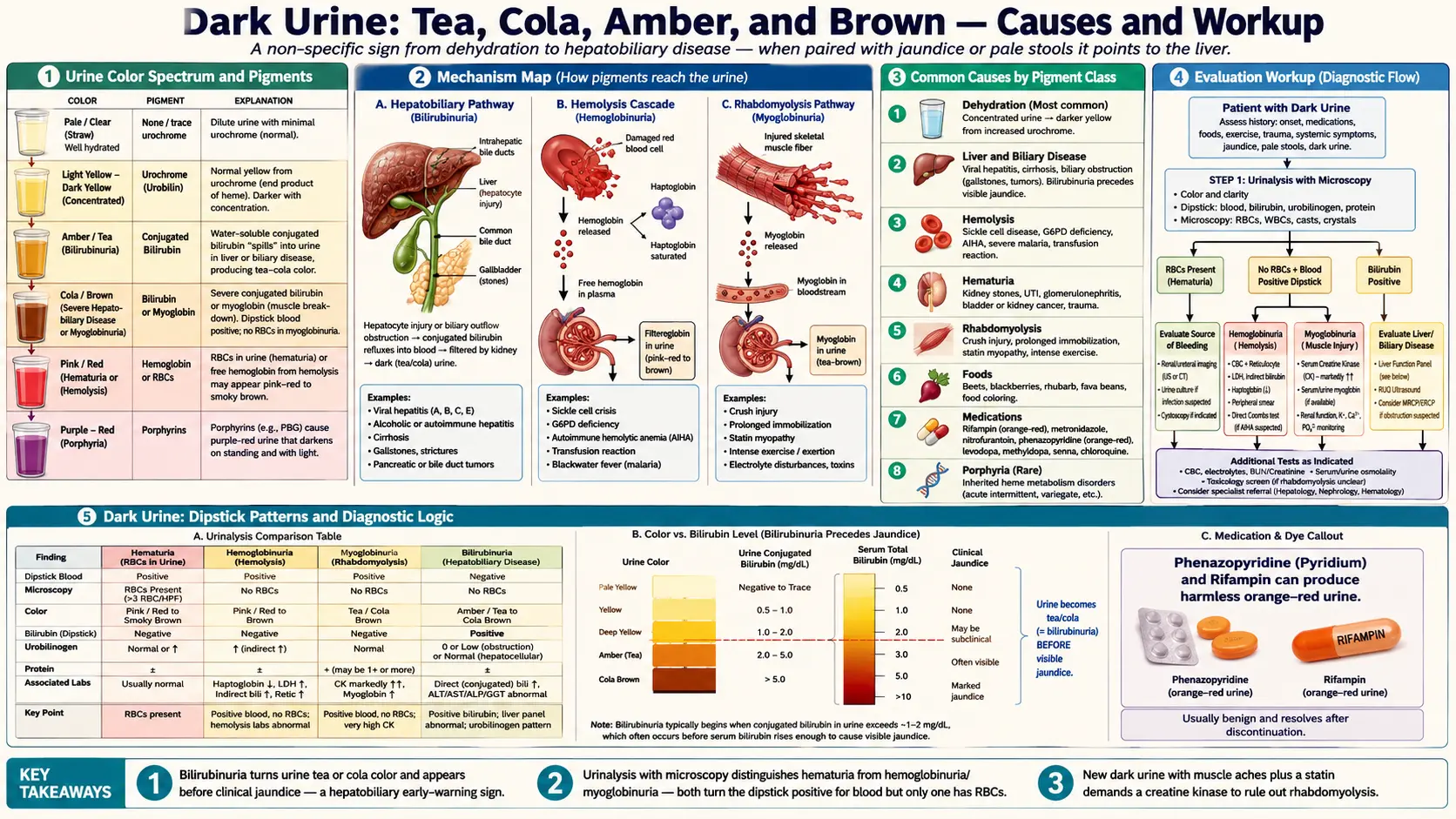

Table of Contents
- Overview
- What Determines Urine Color
- Common Causes
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Dark urine describes urine that appears tea-, cola-, brown-, or amber-colored rather than the normal pale to medium yellow. It is a non-specific sign that can reflect simple dehydration, medications and foods, blood in the urine, muscle breakdown, or — most importantly — liver and biliary disease. When dark urine accompanies jaundice, pale stools, fatigue, or right upper quadrant pain, it strongly suggests a hepatobiliary problem and warrants prompt evaluation.
What Determines Urine Color
Normal urine color comes from urochrome (urobilin), a yellow pigment derived from the breakdown of hemoglobin and ultimately bilirubin. The deeper the color, the more concentrated the urine. Several other substances can change urine color dramatically:
- Conjugated bilirubin — water-soluble, spills into urine when liver or biliary disease is present, producing tea or cola color.
- Hemoglobin or red blood cells — pink, red, or smoky brown urine from hematuria or hemolysis.
- Myoglobin — released during muscle breakdown (rhabdomyolysis), produces tea-colored urine that tests positive for "blood" but contains no red cells.
- Porphyrins — purple-red urine that may darken on standing in porphyria.
Common Causes
- Dehydration — the most common cause; concentrated urine appears darker yellow or amber.
- Liver and biliary disease — viral hepatitis, cirrhosis, biliary obstruction (gallstones, tumors). Conjugated bilirubin appears in urine before clinical jaundice is visible.
- Hemolysis — sickle cell crisis, G6PD deficiency, autoimmune hemolytic anemia, transfusion reactions, severe malaria (blackwater fever).
- Hematuria — kidney stones, urinary tract infection, glomerulonephritis, bladder or kidney cancer, trauma.
- Rhabdomyolysis — crush injury, prolonged immobilization, statin myopathy, intense exercise.
- Foods — beets, blackberries, rhubarb, fava beans, food coloring.
- Medications — rifampin, metronidazole, nitrofurantoin, phenazopyridine (orange-red), levodopa, methyldopa, senna, chloroquine.
- Porphyria — rare inherited disorders of heme metabolism.
Evaluation
- Urinalysis with microscopy — distinguishes hematuria (red cells present) from hemoglobinuria/myoglobinuria (positive blood, no cells) and detects bilirubin and urobilinogen.
- Liver function panel — bilirubin (total and direct), ALT, AST, alkaline phosphatase, GGT.
- Complete blood count and reticulocyte count — for hemolysis.
- Creatine kinase — markedly elevated in rhabdomyolysis.
- Urine culture — if infection is suspected.
- Imaging — renal ultrasound or CT for stones, masses, or obstructive uropathy; right upper quadrant ultrasound for biliary disease.
Management
Management depends entirely on the underlying cause. Mild dehydration resolves with fluids. Hepatitis-related dark urine improves as liver inflammation subsides. Biliary obstruction may need endoscopic stone removal or stenting. Rhabdomyolysis requires aggressive intravenous hydration to protect the kidneys. Drug-related discoloration resolves when the medication is stopped. Pyridium and rifampin discoloration is harmless and expected.
When to Seek Medical Care
- Dark urine accompanied by yellow skin or eyes (jaundice).
- Visible blood, clots, or pink/red discoloration not explained by foods.
- Associated flank or abdominal pain, fever, or chills.
- After significant muscle injury, prolonged immobilization, or new statin therapy with muscle aches.
- Persistent dark urine despite adequate hydration.
Connections
- Jaundice
- Hepatitis
- Liver Disease
- Kidney Stones
- Sickle Cell Disease
- Pale Stool
- Urinary Tract Infections
- Cirrhosis
- Anemia
- Urinalysis
- Kidney Disease
- Fatigue
- Abdominal Pain
- Non-Alcoholic Fatty Liver Disease
- Malaria
- Hepatitis B
- Hepatitis C
- Loss Of Appetite
- Kidney Cancer
References & Research
Historical Background
Examination of urine — uroscopy — has been a cornerstone of medicine since antiquity, with detailed color charts in use throughout the medieval period. Modern dipstick urinalysis emerged in the 1950s, allowing rapid bedside detection of bilirubin, urobilinogen, blood, protein, and other markers. The recognition that conjugated bilirubinuria precedes clinical jaundice in liver disease has made urine testing an early warning system for hepatobiliary illness.
Key Research Papers
- Cohen RA, Brown RS. Microscopic hematuria. New England Journal of Medicine. 2003;348(23):2330-2338.
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. New England Journal of Medicine. 2009;361(1):62-72.
- Aycock RD, Kass DA. Abnormal urine color. Southern Medical Journal. 2012;105(1):43-47.
- Kelly JD, Fawcett DP, Goldberg LC. Assessment and management of non-visible haematuria in primary care. BMJ. 2009;338:a3021.
- Anderson KE, Bloomer JR, Bonkovsky HL, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Annals of Internal Medicine. 2005;142(6):439-450.
- Simerville JA, Maxted WC, Pahira JJ. Urinalysis: a comprehensive review. American Family Physician. 2005;71(6):1153-1162.
- Tracz MJ, Alam J, Nath KA. Physiology and pathophysiology of heme: implications for kidney disease. Journal of the American Society of Nephrology. 2007;18(2):414-420.