Dizziness and Vertigo
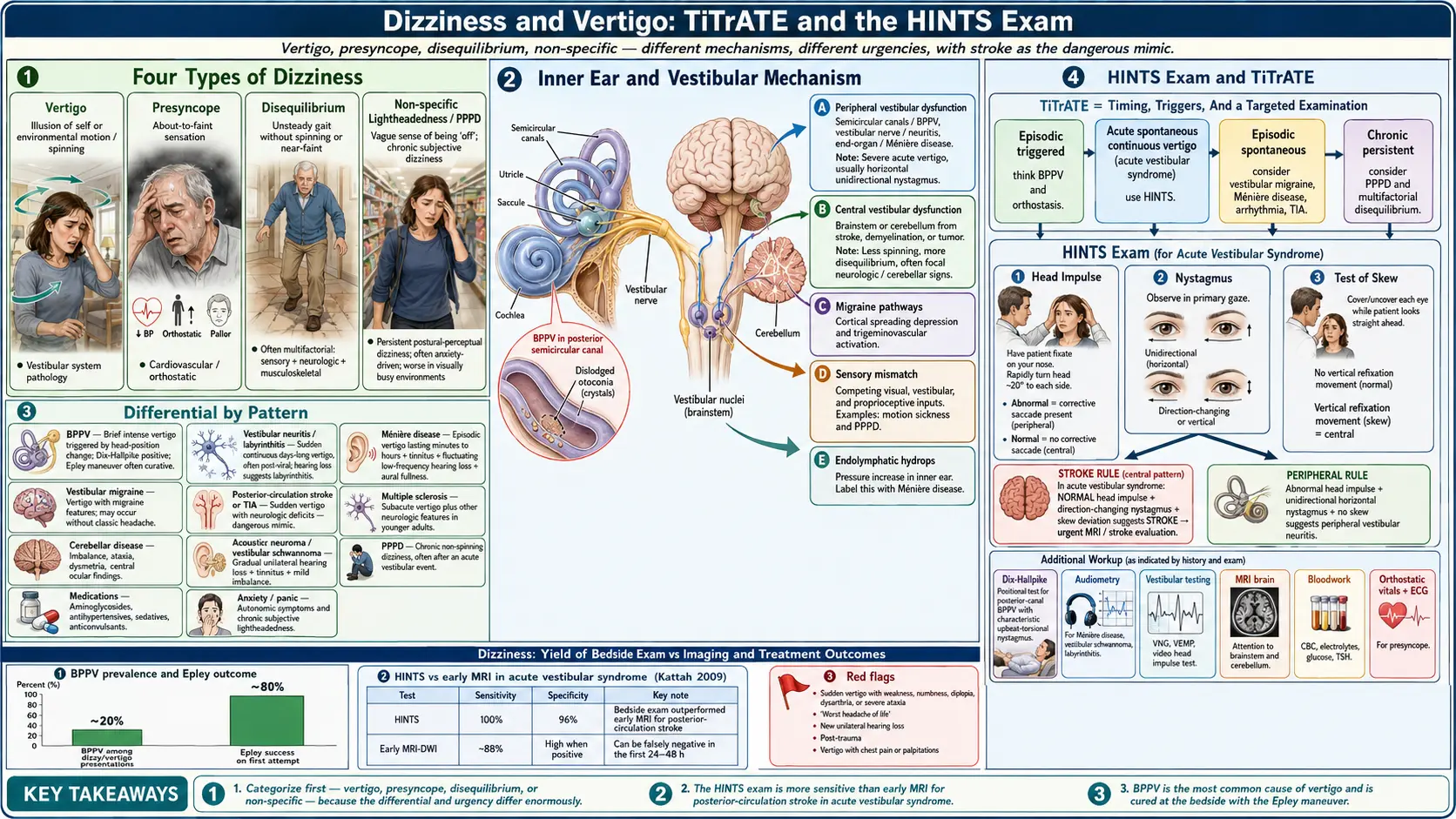


Table of Contents
- Classification: Vertigo vs Presyncope vs Disequilibrium
- BPPV — Most Common Cause of Vertigo
- Vestibular Neuritis and Labyrinthitis
- Meniere's Disease
- Central Vertigo — Stroke
- Orthostatic Hypotension and Presyncope
- Persistent Postural Perceptual Dizziness (PPPD)
- Workup Algorithm
- Connections
- References & Research
- Featured Videos
Classification: Vertigo vs Presyncope vs Disequilibrium vs Non-specific
The first task in any dizziness evaluation is determining which type the patient is describing — this single step dictates the entire differential and level of urgency.
True vertigo is the illusion of rotation or movement of the self or the environment. It always implies peripheral or central vestibular pathology. Peripheral causes include BPPV, labyrinthitis, and Meniere's disease. Central causes include brainstem and cerebellar stroke or tumor.
Presyncope is the sensation of an imminent faint — often described as lightheadedness or graying of vision — and is a cardiovascular or autonomic symptom, not a vestibular one. The workup focuses on ECG, tilt table testing, and orthostatic vital signs rather than vestibular function tests.
Disequilibrium is impaired balance on standing or walking without a head sensation. It is usually a sensorimotor problem — most commonly multifactorial in the elderly — combining peripheral neuropathy, reduced vision, diminished proprioception, cerebellar ataxia, or parkinsonism.
Non-specific or psychological dizziness — a floating, rocking, or swaying sensation without true rotation — is common in anxiety and panic. Persistent postural-perceptual dizziness (PPPD) is the unified diagnostic category for chronic functional dizziness.
BPPV — Most Common Cause of Vertigo
Benign paroxysmal positional vertigo accounts for approximately 50% of recurrent vertigo cases and is the single most common peripheral vestibular disorder. The mechanism involves otoconia — calcium carbonate crystals normally embedded in the utricle — that dislodge and migrate into the posterior semicircular canal (80–90% of cases). When the head changes position, these free-floating canaliths generate abnormal fluid currents, producing a brief intense burst of vertigo and nystagmus.
Any head position change can trigger an attack: lying down, turning in bed, looking up (as when reaching for a high shelf), or bending forward. The critical diagnostic feature is duration — attacks last only 5 to 30 seconds. There is no hearing loss and no tinnitus.
The Dix-Hallpike test is the gold standard: the head is turned 45 degrees toward the affected side, the patient is rapidly lowered to supine, and the examiner watches for upbeat-torsional nystagmus (fast phase toward the affected ear, onset after a 5–20 second latency, fatigable on repeated testing — these three features indicate peripheral origin and distinguish BPPV from a central cause).
The Epley canalith repositioning maneuver achieves immediate relief in about 80% of patients and can be repeated if the first attempt fails. Patients are advised to avoid sleeping on the affected side for 48 hours after treatment. For the less common horizontal canal BPPV, the Lempert (BBQ roll) maneuver is used, guided by direction-changing horizontal nystagmus patterns.
Vestibular Neuritis and Labyrinthitis
Vestibular neuritis is viral inflammation of the vestibular nerve, most likely from herpes simplex type 1 reactivation (HSV-1 has been identified in autopsy specimens of vestibular ganglia). It presents as sudden, severe, continuous vertigo — maximum at onset, then gradually improving over days to weeks as the brain's central vestibular compensation circuits adapt. There is no hearing loss and no tinnitus.
Acute treatment includes methylprednisolone (40 mg tapering course), which improves long-term recovery of vestibular function when started within 72 hours. Vestibular suppressants (meclizine, diazepam) provide symptomatic relief during the first 48–72 hours but should then be discontinued — prolonged use delays central compensation. Vestibular physical therapy (Cawthorne-Cooksey exercises, gaze stabilization exercises) significantly accelerates recovery and should be started as soon as the patient can tolerate head movement.
Labyrinthitis presents identically but adds sensorineural hearing loss and tinnitus because the cochlea is also inflamed. An audiogram is required at presentation and follow-up to track hearing recovery. Bacterial labyrinthitis is rare and serious, requiring IV antibiotics to prevent spread to the meninges.
Meniere's Disease
Meniere's disease is caused by endolymphatic hydrops — excess endolymph in the cochlear and vestibular labyrinth that periodically ruptures Reissner's membrane, mixing endo- and perilymph, and producing episodic attacks. The classic tetrad: aural fullness → low-frequency sensorineural hearing loss → low-pitched roaring tinnitus → vertigo lasting 20 minutes to 12 hours.
The duration of vertigo attacks is diagnostically critical: episodes of Meniere's last 20 minutes to 12 hours (longer than BPPV's seconds, shorter than vestibular neuritis's days). Hearing loss is fluctuating early in the disease — it recovers between attacks — but eventually becomes permanent and typically unilateral.
Diagnostic evaluation includes audiometry (low-frequency SNHL), electrocochleography (elevated summating potential-to-action potential ratio), and MRI to exclude acoustic neuroma (vestibular schwannoma). Treatment begins conservatively: low-sodium diet (less than 2,000 mg/day) and thiazide diuretics (hydrochlorothiazide/triamterene, acetazolamide). Betahistine is widely prescribed in Europe with modest evidence. For medically refractory vertigo, intratympanic gentamicin ablates vestibular function on the affected side, controlling vertigo in 80–90% of cases at the cost of worsening hearing loss in that ear. Endolymphatic sac surgery and vestibular nerve section are options when hearing is worth preserving.
Central Vertigo — Stroke
The most dangerous diagnosis to miss in acute dizziness is posterior circulation stroke. The HINTS exam — Head Impulse test, Nystagmus pattern, Test of Skew — is a three-step bedside examination that outperforms early MRI in identifying posterior fossa stroke.
Head impulse test (HIT): a normal HIT (no corrective saccade after rapid head movement) in the setting of acute vestibular syndrome is a central red flag. A corrective saccade (an abnormal HIT) suggests peripheral pathology. Nystagmus: direction-changing nystagmus or pure vertical nystagmus indicates a central cause. Peripheral nystagmus is unidirectional and suppressed by gaze fixation. Test of Skew: vertical skew deviation (one eye positioned higher than the other) is a reliable indicator of brainstem pathology. A HINTS result of normal HIT + direction-changing or vertical nystagmus + skew deviation has sensitivity 100% and specificity 96% for posterior fossa stroke — superior to diffusion-weighted MRI in the first 24–72 hours, which misses 12% of posterior fossa strokes during the initial window.
PICA territory strokes produce Wallenberg syndrome (severe vertigo, dysphagia, ipsilateral facial numbness, contralateral body numbness, Horner's syndrome). AICA strokes can mimic BPPV in onset but add ipsilateral hearing loss. Cerebellar strokes produce profound gait ataxia and truncal instability.
Vestibular migraine is the most common cause of recurrent episodic vertigo after BPPV. It predominantly affects young women. Episodes last 5 minutes to 72 hours and are associated with headache (though not necessarily during every episode), phonophobia, and photophobia. Treatment follows migraine management protocols: acute therapy with triptans, prophylaxis with topiramate, propranolol, venlafaxine, or valproate.
Orthostatic Hypotension and Presyncope
Orthostatic hypotension is defined as a sustained drop of at least 20 mmHg systolic or 10 mmHg diastolic within 3 minutes of standing. The most common cause is volume depletion — dehydration, bleeding, diuretics, or diarrhea. Neurogenic causes include diabetic autonomic neuropathy, multiple system atrophy (MSA), pure autonomic failure, and Lewy body disease. Medications are a frequent culprit: antihypertensives, alpha-blockers, tricyclic antidepressants, Parkinson's disease medications, and nitrates.
Initial orthostatic hypotension occurs within the first 30 seconds of standing and is physiological in some individuals. Delayed orthostatic hypotension (developing after 3 or more minutes) often indicates neurogenic autonomic failure. Vasovagal syncope is triggered by emotional stimuli, heat, or prolonged standing and is preceded by a prodrome of nausea, diaphoresis, and pallor. Tilt table testing confirms the diagnosis; treatment includes physical countermeasures (leg crossing, squatting), salt and fluid loading, and fludrocortisone for recurrent cases.
POTS (Postural Orthostatic Tachycardia Syndrome) produces a heart rate rise of 30 bpm or more within 10 minutes of standing without a blood pressure drop. It predominantly affects young women and has surged in incidence post-COVID-19. Patients experience chronic fatigue, cognitive symptoms (“brain fog”), and exercise intolerance alongside positional dizziness.
Persistent Postural Perceptual Dizziness (PPPD)
PPPD is the most common cause of chronic dizziness in vestibular specialist referral centers, yet it is not a structural or neurological diagnosis — it is a functional disorder arising from maladaptive threat-appraisal, postural hypervigilance, and failure of the brain's normal vestibular-anxiety downregulation circuits. It was previously called “phobic postural vertigo,” “chronic subjective dizziness,” and several other terms, which were unified into PPPD by the Bárány Society in 2017.
Diagnostic criteria (ICVD 2017): symptoms lasting 3 or more months; a floating, rocking, or unsteady sensation (not true rotational vertigo); worsened by upright posture, active or passive motion, and complex visual environments (busy supermarkets, scrolling screens, cars passing); often precipitated by an acute vestibular event (BPPV, neuritis, concussion, panic attack) that resolved but left residual hypersensitivity.
The mechanism involves the brain's failure to downregulate the hyperalert postural control system after a genuine acute vestibular threat — a kind of maladaptive learned response where normal vestibular signals are interpreted as threatening. Treatment combines cognitive-behavioral therapy (the strongest evidence base, addressing catastrophizing and avoidance behaviors), SSRIs or SNRIs (sertraline, venlafaxine; effective over an 8–12 week trial; treat the underlying anxiety component), and vestibular physical therapy with gradual motion exposure. Combination of all three approaches produces the best outcomes.
Workup Algorithm
Acute onset of seconds' duration with positional trigger: BPPV is the most likely diagnosis — perform Dix-Hallpike. If non-positional, consider cardiac arrhythmia (Holter monitor) or hyperventilation.
Acute constant vestibular syndrome lasting days: apply the HINTS exam urgently. If any central HINTS feature (normal HIT, direction-changing/vertical nystagmus, or skew deviation), treat as posterior fossa stroke and proceed to MRI with DWI plus MRA of the posterior circulation — do not be reassured by a negative initial MRI, which may miss early stroke.
Episodic vertigo lasting minutes to hours: consider Meniere's (hearing loss + low-pitched tinnitus), vestibular migraine (headache history + photophobia), TIA (brief duration + vascular risk factors), or anxiety/PPPD.
Chronic dizziness: PPPD (constant swaying, position- and motion-sensitive), orthostatic hypotension (postural timing, check standing vitals), or presbystasis (elderly multisensory balance loss).
Investigations to order by context: audiogram for any vertigo with hearing complaints; MRI posterior fossa for central HINTS features, first episodic vertigo without BPPV diagnosis, or atypical features; ECG and Holter for presyncope; tilt table testing for suspected POTS or vasovagal syncope; videonystagmography (VNG) and video head impulse test (vHIT) in specialist referral for canal paresis quantification.
Connections
- Lightheadedness
- Multiple Sclerosis
- Headache
- Stroke
- Migraine
- Tinnitus
- Vertigo / Menière’s Disease
- Numbness & Tingling
- POTS
- Vestibular Migraine
- Anxiety
- Depression
- Chest Pain
- Magnesium
- Nausea & Vomiting
- Acesulfame Potassium
- Epilepsy
- Ginkgo Biloba
References & Research
Historical Background
Robert Bárány earned the 1914 Nobel Prize for his work on caloric testing and the physiology of the vestibular system. John Epley's 1980 paper describing canalith repositioning transformed BPPV from a chronic, debilitating disorder into a condition treatable in under five minutes without medication. The HINTS exam was formally validated by Kattah and Newman-Toker in 2009, demonstrating that a three-step bedside oculomotor examination outperformed early diffusion-weighted MRI for identifying posterior circulation stroke in patients with acute vestibular syndrome. Vestibular migraine was formally codified in 2012 by the Bárány Society and the International Headache Society. PPPD was unified from multiple overlapping diagnoses by the Bárány Society in 2017.
Key Research Papers
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome. Stroke. https://doi.org/10.1161/STROKEAHA.109.551234 2009;40(11):3504-3510.
- Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngology — Head and Neck Surgery. https://doi.org/10.1177/0194599816689667 2017;156(3 Suppl):S1-S47.
- Staab JP, Eckhardt-Henn A, Horii A, et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD). Journal of Vestibular Research. https://doi.org/10.3233/VES-170622 2017;27(4):191-208.
- Bhattacharyya N, et al. Clinical practice guideline: Menière’s disease (2020). Otolaryngology — Head and Neck Surgery. https://doi.org/10.1177/0194599820909438 2020;162(2 Suppl):S1-S55.
- Kim JS, Kim HJ. Inferior vestibular neuritis. Journal of Neurology. https://doi.org/10.1007/s00415-012-6550-7 2012;259(8):1553-1560.
- Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria. Journal of Vestibular Research. https://doi.org/10.3233/VES-2012-0453 2012;22(4):167-172.
- Newman-Toker DE, Edlow JA. TiTrATE: a novel approach to diagnosing acute dizziness and vertigo. Neurologic Clinics. https://doi.org/10.1016/j.ncl.2015.04.011 2015;33(3):577-599.
- Furman JM, Cass SP. Benign paroxysmal positional vertigo. New England Journal of Medicine. https://doi.org/10.1056/NEJM199906033402206 1999;341(21):1590-1596.
- McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD005397.pub4 2015;(1):CD005397.
- Sajjadi H, Paparella MM. Meniere's disease. The Lancet. https://doi.org/10.1016/S0140-6736(08)61161-7 2008;372(9636):406-414.
- Kim JS, Zee DS. Benign paroxysmal positional vertigo. New England Journal of Medicine. https://doi.org/10.1056/NEJMcp1100780 2014;370(12):1138-1147.
- Welgampola MS, Bradshaw AP, Lechner C, Halmagyi GM. Bedside assessment of acute dizziness and vertigo. Neurologic Clinics. https://doi.org/10.1016/j.ncl.2015.04.003 2015;33(3):551-564.
PubMed Topic Searches
- BPPV and the Epley maneuver
- HINTS exam for vestibular stroke
- Meniere's disease treatment
- Vestibular migraine
- Persistent postural-perceptual dizziness (PPPD)
- POTS and post-COVID dizziness