Tinnitus
A comprehensive guide to understanding and managing tinnitus from a Naturopathic Doctor perspective, including conventional treatments and evidence-based natural approaches.
Interactive Visualization Hearing & the Cochlea — send a sound wave in Slide the frequency and watch the traveling wave peak land on its tonotopic place inside the cochlea. Launch →Table of Contents
- What Is Tinnitus?
- Subjective vs. Objective Tinnitus
- Common Causes of Tinnitus
- Vascular Causes
- Neurological Factors
- Risk Factors
- Conventional Treatments
- Natural and Naturopathic Approaches
- Sound Therapy and Masking
- Stress and Tinnitus Connection
- Dietary Triggers
- Neck and Jaw Therapy
- Acupuncture Research
- Lifestyle Modifications
- Cautions and When to Seek Medical Attention
- References & Research
- Featured Videos
What Is Tinnitus?
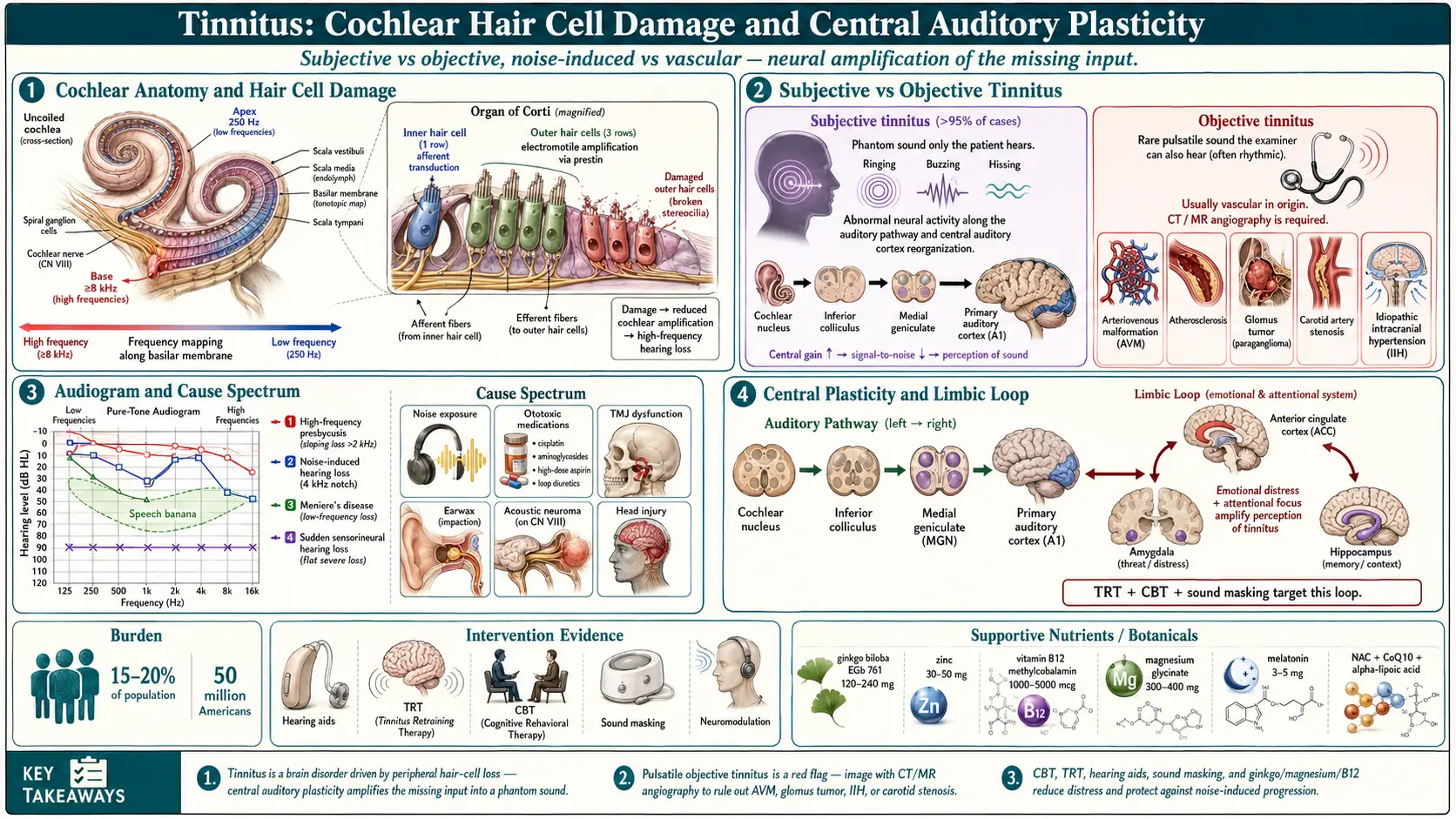
Tinnitus is the perception of sound in the ears or head without an external acoustic source. It affects an estimated 15 to 20 percent of the population and becomes more prevalent with age. The phantom sounds may be described as:
- Ringing — the most commonly reported form
- Buzzing — a low-frequency humming or vibration
- Hissing — resembling steam or white noise
- Clicking, roaring, or pulsing — less common variants
Tinnitus is not a disease itself but rather a symptom of an underlying condition affecting the auditory pathway. It can be intermittent or continuous, occur in one or both ears, and range from a mild nuisance to a severely debilitating experience that disrupts sleep, concentration, and emotional well-being.
Subjective vs. Objective Tinnitus
Understanding the distinction between these two categories is essential for proper evaluation and treatment.
Subjective Tinnitus
Subjective tinnitus is by far the most common form, accounting for over 95 percent of cases. Only the affected person can hear the sound. It originates from abnormal neural activity along the auditory pathway, from the cochlea to the auditory cortex. Damage to the hair cells in the inner ear is the most frequent trigger, causing the brain to misinterpret diminished auditory signals as phantom sound.
Objective Tinnitus
Objective tinnitus is rare and can be heard by an examiner using a stethoscope or sensitive microphone placed near the ear. It typically has a vascular or muscular origin, such as turbulent blood flow through narrowed vessels, arteriovenous malformations, or rhythmic contractions of the middle ear muscles or palatal muscles. Because objective tinnitus has an identifiable physical source, it is often treatable once the cause is addressed.
Common Causes of Tinnitus
Tinnitus can arise from a wide range of conditions affecting the ear, the auditory nerve, or the brain regions involved in sound processing.
Noise Exposure
Prolonged or sudden exposure to loud noise is one of the leading causes of tinnitus. Occupational noise (construction, manufacturing, military), recreational noise (concerts, headphones at high volume, firearms), and even a single explosive blast can permanently damage the delicate hair cells of the cochlea.
Age-Related Hearing Loss (Presbycusis)
As hearing naturally declines with age, the brain may compensate for reduced auditory input by amplifying internal neural signals, resulting in tinnitus. This form typically involves high-frequency hearing loss and is very common after age 60.
TMJ Disorders
The temporomandibular joint sits directly adjacent to the ear canal. Dysfunction of this joint, including misalignment, clenching, grinding, or arthritis, can refer pain and abnormal sensations to the ear, producing or worsening tinnitus.
Earwax Impaction
Excessive cerumen buildup can press against the tympanic membrane or occlude the ear canal, causing conductive hearing loss and tinnitus. This is one of the most easily reversible causes.
Meniere's Disease
This inner ear disorder involves abnormal fluid pressure in the endolymphatic system. It presents with episodic vertigo, fluctuating hearing loss, tinnitus, and a sensation of fullness in the affected ear.
Ototoxic Medications
Numerous medications can damage the auditory system and trigger or worsen tinnitus:
- Aspirin — particularly at high doses (more than 8 to 12 tablets daily); the effect is often reversible upon dose reduction
- NSAIDs — ibuprofen, naproxen, and other nonsteroidal anti-inflammatory drugs can cause reversible tinnitus
- Aminoglycoside antibiotics — gentamicin, tobramycin, and streptomycin are directly toxic to inner ear hair cells and can cause permanent damage
- Cisplatin — this chemotherapy agent is highly ototoxic and frequently causes irreversible tinnitus and hearing loss
- Loop diuretics — furosemide at high intravenous doses
- Quinine and antimalarials
Vascular Causes
Vascular tinnitus often produces a pulsatile sound that synchronizes with the heartbeat. It warrants careful evaluation because some underlying causes are serious.
- Atherosclerosis — cholesterol deposits stiffen and narrow blood vessels near the ear, creating turbulent flow that becomes audible
- High blood pressure — hypertension increases the force of blood flow through cranial vessels, making vascular sounds more perceptible
- Arteriovenous malformations — abnormal tangles of arteries and veins can generate audible turbulence
- Glomus tumors — benign vascular tumors at the base of the skull or within the middle ear
- Carotid artery stenosis — narrowing of the carotid artery can produce referred pulsatile tinnitus
- Idiopathic intracranial hypertension — elevated cerebrospinal fluid pressure, particularly in younger women
Pulsatile tinnitus should always be evaluated with imaging studies such as CT angiography, MR angiography, or Doppler ultrasound to rule out structural vascular abnormalities.
Neurological Factors
The brain plays a central role in tinnitus perception. Modern neuroscience views chronic tinnitus as a disorder of neural plasticity rather than simply an ear problem.
- Central auditory processing changes — when peripheral hearing is damaged, the auditory cortex undergoes reorganization, amplifying spontaneous neural activity that is perceived as sound
- Limbic system involvement — the amygdala and hippocampus attach emotional significance to the tinnitus signal, which explains why stress and anxiety intensify the perception
- Acoustic neuroma — a benign schwannoma on the vestibulocochlear nerve (cranial nerve VIII) can cause unilateral tinnitus and hearing loss
- Multiple sclerosis — demyelination of auditory pathways can rarely produce tinnitus
- Head and neck injuries — traumatic brain injury disrupts auditory processing networks
Risk Factors
Several factors increase the likelihood of developing tinnitus or experiencing it more severely:
- Age — incidence rises significantly after age 50
- Male sex — men are more frequently affected, likely due to greater occupational and recreational noise exposure
- Smoking — nicotine constricts blood vessels and impairs cochlear blood supply
- Cardiovascular disease — conditions affecting blood flow increase vascular tinnitus risk
- Anxiety and depression — bidirectional relationship; mental health conditions lower the threshold for tinnitus perception and distress
- Occupational noise exposure — military personnel, musicians, construction workers, and factory workers
- Chronic stress — heightens central nervous system arousal and tinnitus awareness
Conventional Treatments
There is currently no pharmaceutical cure for most forms of subjective tinnitus. Conventional management focuses on reducing the perception and impact of tinnitus.
Hearing Aids
For patients with coexisting hearing loss, hearing aids amplify ambient sounds and reduce the contrast between external silence and internal tinnitus. Many modern hearing aids include built-in tinnitus masking programs that generate low-level broadband noise.
Tinnitus Retraining Therapy (TRT)
TRT combines directive counseling with sound generators worn in or behind the ear. The goal is neuroplastic habituation, training the brain to reclassify the tinnitus signal as neutral background noise that no longer requires conscious attention. TRT typically requires 12 to 24 months of consistent use and has shown moderate to good long-term outcomes.
Cognitive Behavioral Therapy (CBT)
CBT is the most evidence-supported psychological intervention for tinnitus distress. It does not eliminate the sound but restructures the maladaptive thought patterns and emotional responses that amplify suffering. CBT addresses catastrophic thinking, sleep disruption, avoidance behaviors, and hypervigilance. Multiple randomized controlled trials demonstrate significant reductions in tinnitus distress, anxiety, and depression.
Medications
No medication is approved specifically for tinnitus, but certain drugs may be prescribed off-label to manage associated symptoms:
- Antidepressants (amitriptyline, nortriptyline) for tinnitus-related depression and insomnia
- Benzodiazepines (alprazolam) for short-term anxiety relief, though dependence limits long-term use
- Anticonvulsants (gabapentin) in select cases
Natural and Naturopathic Approaches
From a Naturopathic Doctor perspective, addressing tinnitus involves identifying and treating root causes, reducing inflammation and oxidative stress in the auditory system, supporting nerve health, and optimizing overall vitality. The following nutrients and botanicals have research support, though results vary among individuals.
Ginkgo Biloba
Ginkgo biloba extract (standardized to 24 percent flavone glycosides and 6 percent terpene lactones) is the most extensively studied botanical for tinnitus. It improves microcirculation to the cochlea, provides antioxidant protection, and modulates neurotransmitter activity. Typical dosing is 120 to 240 mg daily in divided doses. European studies, particularly using the EGb 761 extract, have shown benefit for tinnitus associated with cerebrovascular insufficiency. Results for other forms of tinnitus are mixed, and a trial of at least 8 to 12 weeks is recommended.
Zinc
Zinc is concentrated in the cochlea and is essential for proper auditory function. Deficiency is more common in older adults and has been correlated with tinnitus severity. Supplementation with 30 to 50 mg of zinc picolinate or zinc citrate daily has shown benefit in patients with documented low serum zinc levels. Testing zinc status before supplementation is advisable.
Vitamin B12
B12 deficiency can cause neurological damage including auditory nerve dysfunction. Studies have found a higher prevalence of B12 deficiency among tinnitus patients compared to controls. Supplementation with methylcobalamin (1000 to 5000 mcg daily, sublingual or intramuscular) may reduce tinnitus in deficient individuals. Serum B12 and methylmalonic acid levels should be checked.
Magnesium
Magnesium protects the inner ear from noise-induced damage by regulating glutamate release at the hair cell synapse. Excessive glutamate is excitotoxic to auditory neurons. Supplementation with 300 to 400 mg daily of magnesium glycinate or magnesium taurate may help prevent noise-induced tinnitus and support overall nerve function. Military studies have demonstrated reduced hearing damage in soldiers supplemented with magnesium before noise exposure.
Melatonin
Melatonin (3 to 5 mg at bedtime) has shown benefit for tinnitus-related sleep disturbance in multiple studies. It may also exert direct antioxidant effects in the inner ear. It is particularly useful for patients whose tinnitus is most bothersome at night.
N-Acetylcysteine (NAC)
NAC is a precursor to glutathione, the body's master antioxidant. It has demonstrated protective effects against noise-induced hearing damage in both animal and human studies. Doses of 600 to 1200 mg daily may help reduce oxidative stress in the cochlea, particularly when taken before or shortly after noise exposure.
Coenzyme Q10 (CoQ10)
CoQ10 supports mitochondrial energy production in the metabolically active cells of the inner ear. Some clinical studies have reported improvement in tinnitus with 100 to 300 mg daily, especially in patients with lower baseline CoQ10 levels. It also provides antioxidant protection and supports cardiovascular health.
Alpha-Lipoic Acid
Alpha-lipoic acid is a versatile antioxidant that crosses the blood-brain barrier and regenerates other antioxidants including vitamins C and E, and glutathione. Doses of 300 to 600 mg daily may support auditory nerve health and reduce age-related oxidative damage. It has particular relevance for tinnitus in patients with diabetes or metabolic syndrome.
Sound Therapy and Masking
Sound-based interventions aim to reduce the prominence of tinnitus by enriching the auditory environment.
- White noise machines — generate broadband sound that reduces the contrast between silence and tinnitus, particularly helpful for sleep
- Nature sounds — rain, ocean waves, and flowing water are common choices that provide gentle masking
- Notched music therapy — music with the frequency band matching the patient's tinnitus pitch removed; this approach aims to reduce cortical overrepresentation of the tinnitus frequency through lateral inhibition
- Neuromodulation-based sound therapy — newer approaches pair acoustic stimulation with vagus nerve or tongue stimulation to promote neuroplastic changes
- Hearing aid maskers — combination devices that amplify external sound while simultaneously generating tinnitus-masking noise
Sound enrichment should be used at a level just below the tinnitus rather than fully masking it, as partial masking promotes habituation while complete masking may delay it.
Stress and Tinnitus Connection
Stress and tinnitus exist in a vicious cycle. Stress activates the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis, increasing cortisol levels and heightening neural arousal throughout the brain, including the auditory cortex. This amplifies tinnitus perception. In turn, the distress caused by tinnitus generates further stress.
Effective stress management is therefore a cornerstone of tinnitus treatment:
- Mindfulness meditation — trains the brain to observe the tinnitus without reacting emotionally; mindfulness-based stress reduction programs have shown significant benefit in clinical trials
- Deep breathing exercises — activate the parasympathetic nervous system and reduce cortisol
- Progressive muscle relaxation — systematically releasing tension throughout the body reduces the physical component of stress
- Yoga and tai chi — combine physical movement, breathwork, and meditative awareness
- Adequate sleep — sleep deprivation worsens tinnitus; prioritizing sleep hygiene is essential
- Adaptogenic herbs — ashwagandha, rhodiola, and holy basil may support the stress response and reduce HPA axis hyperactivation
Dietary Triggers
Certain dietary substances can exacerbate tinnitus in susceptible individuals. Identifying and eliminating personal triggers through a structured elimination diet can be valuable.
Caffeine
Caffeine is a central nervous system stimulant that can increase neural excitability and worsen tinnitus in some people. However, research is mixed, and abrupt caffeine withdrawal can also temporarily worsen tinnitus. A gradual reduction trial over two to three weeks is recommended rather than sudden cessation.
Alcohol
Alcohol dilates blood vessels and increases blood flow to the inner ear, which may intensify tinnitus, particularly the pulsatile variety. It also disrupts sleep architecture, compounding nighttime tinnitus distress.
Sodium
Excess sodium intake promotes fluid retention, which can increase endolymphatic pressure in the inner ear. This is particularly relevant for patients with Meniere's disease. A low-sodium diet (under 1500 mg daily) is often recommended.
MSG (Monosodium Glutamate)
MSG is an excitatory neurotransmitter analogue. Glutamate excitotoxicity at the cochlear synapse is a proposed mechanism of noise-induced tinnitus. Avoiding MSG and other sources of free glutamate (hydrolyzed protein, autolyzed yeast extract) may benefit some patients.
Dietary Recommendations
An anti-inflammatory, nutrient-dense diet supports auditory health:
- Emphasize colorful vegetables, berries, and fruits rich in antioxidants
- Include omega-3 fatty acids from wild-caught fish, flaxseed, and walnuts
- Choose whole grains over refined carbohydrates to maintain stable blood sugar
- Minimize processed foods, refined sugar, and artificial additives
Neck and Jaw Therapy
Somatic tinnitus, tinnitus that can be modulated by movements of the head, neck, or jaw, is surprisingly common and represents an important treatment opportunity.
TMJ Assessment and Treatment
Temporomandibular joint dysfunction is a frequently overlooked contributor to tinnitus. Evaluation by a dentist or orofacial pain specialist may reveal clenching, grinding, malocclusion, or joint derangement. Treatments include:
- Custom oral appliances (night guards or splints) to reduce clenching forces
- Physical therapy targeting the muscles of mastication
- Myofascial release of the masseter, temporalis, and pterygoid muscles
Cervical Spine Therapy
Dysfunction of the upper cervical spine can alter somatosensory input to the dorsal cochlear nucleus, modulating tinnitus. Approaches include:
- Chiropractic adjustment of the upper cervical vertebrae
- Osteopathic manipulation
- Physical therapy with cervical strengthening and postural correction
- Craniosacral therapy
Acupuncture Research
Acupuncture has been used for tinnitus in Traditional Chinese Medicine for centuries. Modern research has yielded mixed but generally encouraging results.
- Several systematic reviews suggest that acupuncture may reduce tinnitus loudness and distress compared to sham acupuncture, though study quality varies
- Electroacupuncture, which adds mild electrical stimulation to the needles, may be more effective than manual acupuncture alone for tinnitus
- Common acupuncture points used for tinnitus include Tinggong (SI19), Tinghui (GB2), Ermen (TB21), Yifeng (TB17), and Zhongzhu (TB3)
- Scalp acupuncture targeting the auditory cortex region is a specialized technique with preliminary positive findings
- Acupuncture may work for tinnitus by modulating neural activity in the auditory pathway, improving local circulation, and reducing stress-related amplification
A course of 10 to 12 sessions is typically recommended before evaluating response. Acupuncture is generally safe and well tolerated and can be combined with other therapies.
Lifestyle Modifications
Daily habits play a significant role in tinnitus management. The following modifications support auditory health and reduce tinnitus severity:
- Hearing protection — use earplugs or noise-canceling headphones in loud environments; custom-molded musician earplugs attenuate sound evenly without distortion
- Volume management — follow the 60/60 rule for headphone use (no more than 60 percent volume for no more than 60 minutes at a time)
- Regular exercise — cardiovascular exercise improves blood flow to the cochlea, reduces stress, and supports overall nerve health; aim for 30 minutes of moderate activity most days
- Sleep hygiene — maintain consistent sleep and wake times, keep the bedroom dark and cool, use a sound machine if needed, and avoid screens before bed
- Smoking cessation — nicotine is vasoconstrictive and ototoxic; quitting significantly improves cochlear blood supply
- Limit ototoxic drug use — discuss alternatives with your prescribing physician when possible
- Stay socially engaged — social isolation worsens tinnitus distress; maintain connections and activities that provide purpose and enjoyment
- Blood sugar regulation — insulin resistance and diabetes are associated with increased tinnitus risk; maintain stable glucose through diet, exercise, and supplementation as needed
Cautions and When to Seek Medical Attention
While many cases of tinnitus can be managed with the approaches described above, certain presentations require prompt medical evaluation:
- Unilateral tinnitus — tinnitus in only one ear warrants evaluation for acoustic neuroma or other structural lesions with MRI
- Pulsatile tinnitus — rhythmic tinnitus synchronized with the heartbeat requires vascular imaging to rule out arteriovenous malformations, glomus tumors, or carotid stenosis
- Sudden onset tinnitus with hearing loss — sudden sensorineural hearing loss is a medical emergency requiring urgent treatment, often with high-dose corticosteroids, within 48 to 72 hours
- Tinnitus with neurological symptoms — dizziness, facial numbness, weakness, or visual changes accompanying tinnitus require immediate evaluation
- Severe emotional distress — if tinnitus is causing depression, anxiety, or suicidal ideation, seek professional mental health support immediately
Important notes on natural supplements:
- Always inform your healthcare providers about all supplements you are taking, as interactions with medications are possible
- Ginkgo biloba has blood-thinning properties and should be used cautiously with anticoagulant medications
- Zinc supplementation above 40 mg daily should be paired with 2 mg of copper to prevent copper depletion
- Supplements should complement, not replace, appropriate medical evaluation and treatment
- Work with a qualified Naturopathic Doctor or integrative practitioner to develop a personalized treatment plan
16. References & Research
Historical Background
Tinnitus has been documented since antiquity -- the ancient Egyptians described "bewitched ear" treatments in the Ebers Papyrus (circa 1550 BCE), and Hippocrates referenced ringing in the ears. The modern scientific study of tinnitus began with Jean-Marie Gaspard Itard, a French physician who published the first systematic clinical description in 1821. The neurophysiological model of tinnitus was developed by Pawel Jastreboff in 1990, establishing the basis for Tinnitus Retraining Therapy and shifting the paradigm from a peripheral ear problem to a central nervous system disorder.
Key Research Papers
- Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: causes and clinical management. Lancet Neurol. 2013;12(9):920-930.
- Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. 2014;151(2 Suppl):S1-S40.
- Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990;8(4):221-254.
- Martinez-Devesa P, Waddell A, Perera R, Theodoulou M. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev. 2010;(9):CD005233.
- Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013;382(9904):1600-1607.
- Hilton MP, Zimmermann EF, Hunt WT. Ginkgo biloba for tinnitus. Cochrane Database Syst Rev. 2013;(3):CD003852.
- Savage J, Waddell A. Tinnitus. BMJ Clin Evid. 2014;2014:0506.
- Person OC, Puga ME, da Silva EM, Torloni MR. Zinc supplementation for tinnitus. Cochrane Database Syst Rev. 2016;(11):CD009832.
- Shargorodsky J, Curhan GC, Farwell WR. Prevalence and characteristics of tinnitus among US adults. Am J Med. 2010;123(8):711-718.
- Shore SE, Roberts LE, Bhatt JM. Tinnitus models and mechanisms. Hear Res. 2016;338:52-62.
- Hoare DJ, Edmondson-Jones M, Sereda M, et al. Amplification with hearing aids for patients with tinnitus and co-existing hearing loss. Cochrane Database Syst Rev. 2014;(1):CD010151.
- Eggermont JJ, Roberts LE. The neuroscience of tinnitus. Trends Neurosci. 2004;27(11):676-682.
- Nondahl DM, Cruickshanks KJ, Huang GH, et al. Tinnitus and its risk factors in the Beaver Dam Offspring Study. Int J Audiol. 2011;50(5):313-320.
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Tinnitus. Each link opens a live PubMed query so you always see the most recent publications.
- Tinnitus review mechanism
- Cognitive behavioral therapy tinnitus
- Tinnitus retraining therapy
- Sound therapy masking tinnitus
- Ginkgo biloba tinnitus
- Zinc supplementation tinnitus
- Tinnitus noise exposure hearing loss
- Tinnitus functional neuroimaging
- Tinnitus transcranial magnetic stimulation
- Tinnitus prevalence epidemiology
- Tinnitus TMJ temporomandibular
Connections
- ENT
- Tinnitus: History and Origins — the same symptom across three thousand years of medicine — Egyptian and Hippocratic descriptions, the 1953 silence experiment, Jack Vernon and sound therapy, and Jastreboff’s neurophysiological model.
- Hearing & the Cochlea — interactive animation
- Ginkgo Biloba
- Tinnitus Remedies
- Zinc
- Ginkgo Biloba for Tinnitus
- Magnesium
- Sleep Hygiene
- Stress Management
- Vitamin B12
- Vertigo and Meniere's Disease
- Taurine
- Taurine for Tinnitus
- Glycine for Tinnitus
- Glycine
- Anxiety
- Hypertension
- NAC
- MSG
- Dizziness
- Hearing Loss
- Ear Infections
- Tinnitus Benefits Deep Dive — hub for the four evidence-graded deep-dive articles on causes, nutrients, sound therapy, and antioxidants.
- Tinnitus Causes and Triggers — what sets the ringing off, from noise and ototoxic drugs to TMJ, plus the modifiable trigger inventory.
- Tinnitus — B12, Magnesium and Zinc Status — the three deficiencies worth testing, with cutoffs and repletion protocols.
- Tinnitus — Sound Therapy and Habituation — hearing aids, TRT, masking, notched music, and CBT: the largest non-drug effect sizes.
- Tinnitus — NAC and Antioxidants — glutathione-precursor otoprotection against noise and cisplatin injury, and the Ginkgo Cochrane verdict.