Neuropsychiatric Lupus (NPSLE)
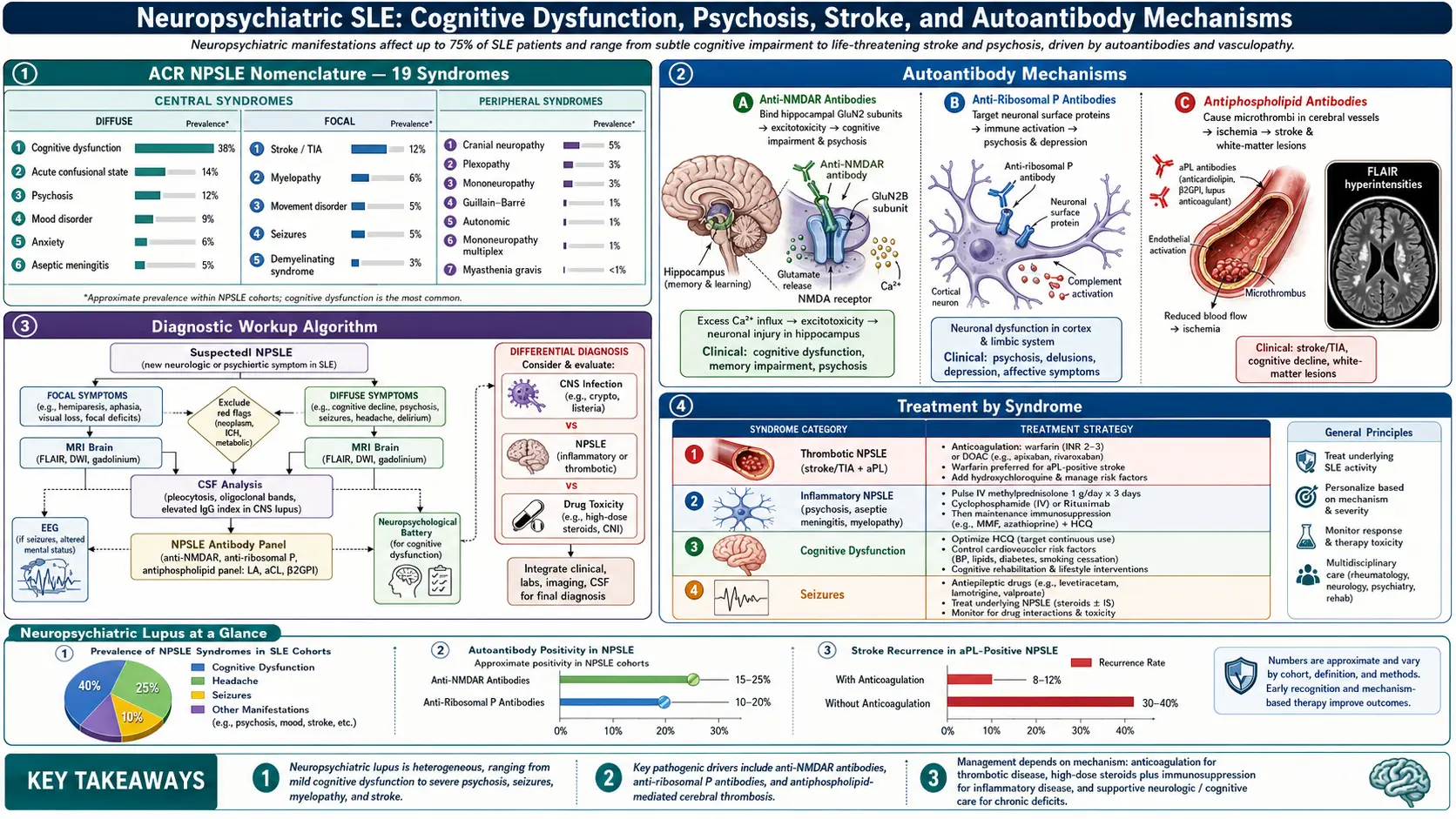
Table of Contents
- What Neuropsychiatric Lupus Is
- The ACR 1999 Nomenclature — 19 Syndromes
- CNS Syndromes in Detail
- PNS Syndromes in Detail
- The Attribution Problem — Primary vs Secondary
- Antiphospholipid Antibodies and Stroke
- Ribosomal P and Lupus Psychosis
- Workup — MRI, CSF, EEG, Neuropsych
- Treatment — Immunosuppress vs Anticoagulate
- Cognitive Rehabilitation and Daily Life
- Red Flags — When to Go to the ER
- Prognosis and Long-Term Outlook
- Key Research Papers
- Connections
- Featured Videos
What Neuropsychiatric Lupus Is
Neuropsychiatric systemic lupus erythematosus (NPSLE) is the umbrella label for any neurologic or psychiatric syndrome that appears in someone who has lupus. It includes everything from a bad migraine to a stroke, from "brain fog" to full-blown psychosis, from tingling feet to Guillain-Barré. The label is broad because lupus can attack almost any part of the nervous system — brain, spinal cord, cranial nerves, peripheral nerves, and the autonomic system that runs your blood pressure and digestion.
Depending on how strictly you count, somewhere between 30% and 75% of lupus patients develop at least one neuropsychiatric syndrome during their illness. About half of those episodes happen in the first year after diagnosis, and many show up before lupus is formally diagnosed, which is why neurologists and psychiatrists are often the first specialists a future lupus patient sees.
The hard part of NPSLE is not recognizing that something neurological is wrong — patients and families usually notice. The hard part is deciding whether lupus itself is causing the problem, or whether something else (an infection, a medication side effect, a clot, a metabolic imbalance) is to blame. That single question drives everything about treatment, and it is covered in the attribution section below.
The ACR 1999 Nomenclature — 19 Syndromes
In 1999 the American College of Rheumatology published a formal case-definition document listing 19 distinct neuropsychiatric syndromes that can be attributed to lupus. Twelve are central nervous system (CNS) problems; seven are peripheral nervous system (PNS) problems. This list is still the international reference standard — every modern NPSLE study uses it, and your rheumatologist's note will almost certainly reference one of these 19 labels.
Twelve CNS syndromes:
- Cognitive dysfunction
- Headache (including lupus headache and intracranial hypertension)
- Mood disorder (depression, mania, mixed features)
- Anxiety disorder
- Psychosis
- Acute confusional state (delirium)
- Seizure disorder
- Cerebrovascular disease (stroke, TIA, venous sinus thrombosis)
- Aseptic meningitis
- Demyelinating syndrome
- Movement disorder (most often chorea)
- Myelopathy (spinal cord involvement, including transverse myelitis)
Seven PNS syndromes:
- Polyneuropathy (length-dependent, often sensory-predominant)
- Mononeuropathy (single or multiple — mononeuritis multiplex)
- Acute inflammatory demyelinating polyradiculoneuropathy (Guillain-Barré syndrome)
- Autonomic disorder
- Plexopathy
- Cranial neuropathy
- Myasthenia gravis
Real patients often carry more than one label at a time. Someone with lupus may have cognitive dysfunction plus mood disorder plus a length-dependent polyneuropathy, and all three can flare and quiet down on different schedules. The list is not a menu of isolated diagnoses — it is a vocabulary for describing a moving target.
CNS Syndromes in Detail
Cognitive dysfunction is the single most common NPSLE manifestation, affecting up to 80% of lupus patients at some point when formally tested. Patients call it "lupus fog": trouble finding words, slower processing, short-term memory lapses, difficulty multitasking. On neuropsychological testing it typically hits attention, working memory, and executive function. Most cases are mild-to-moderate and fluctuate with disease activity. Severe dementia-level cognitive loss is rare but devastating when it happens.
Headache is controversial. Migraine and tension-type headaches are common in lupus, but studies disagree on whether they occur more often than in the general population. A dedicated "lupus headache" (severe, persistent, unresponsive to narcotics) was in the original nomenclature but has not held up well as a distinct entity. What is specific to lupus is cerebral venous sinus thrombosis presenting as a thunderclap or progressive headache, and idiopathic intracranial hypertension (pseudotumor cerebri), both of which require urgent imaging.
Mood disorder — mostly major depression — affects roughly one in four lupus patients. Untangling "depression caused by inflammation in the brain" from "depression caused by living with a serious chronic disease" is genuinely hard, and the treatment (SSRIs, therapy, exercise) overlaps regardless of cause. Mania is much rarer and should prompt a steroid review (see attribution).
Psychosis in lupus is uncommon (1–3% of patients) but dramatic when it appears: delusions, auditory or visual hallucinations, disorganized thinking. It is strongly associated with anti-ribosomal P antibodies and generally responds well to immunosuppression plus antipsychotics.
Seizures occur in 5–15% of lupus patients. Generalized tonic-clonic is the most common type, but any seizure pattern is possible. A single seizure during a flare does not automatically mean lifelong epilepsy — many patients never have a second one once lupus is controlled.
Stroke and TIA are among the most serious NPSLE manifestations. Lupus patients have roughly twice the stroke risk of age-matched controls, driven by a mix of accelerated atherosclerosis, antiphospholipid antibodies (see below), and Libman-Sacks endocarditis throwing emboli from the heart valves. For the general mechanics of stroke workup and recovery, see the Stroke page.
Aseptic meningitis presents with headache, stiff neck, fever, and photophobia, but CSF cultures are negative. NSAIDs (especially ibuprofen) and intravenous immunoglobulin (IVIG) can both trigger it in lupus patients — always check the medication list before calling it "primary" NPSLE.
Demyelinating syndromes look like multiple sclerosis on MRI and can be very hard to distinguish. Neuromyelitis optica (NMO) with AQP4 antibodies can coexist with lupus. When demyelination appears, a full aquaporin-4 and MOG antibody panel is essential before committing to an MS treatment plan that could worsen lupus.
Movement disorders in lupus usually take the form of chorea — irregular, dance-like involuntary movements. It is particularly associated with antiphospholipid antibodies and, historically, with rheumatic fever (Sydenham chorea). Treatment targets both the lupus and, when appropriate, the clotting risk.
Myelopathy, especially longitudinally extensive transverse myelitis, is a neurologic emergency. Patients describe a rapidly ascending band of numbness, weakness, or loss of bladder/bowel control. High-dose IV methylprednisolone within hours is the standard response; delays measurably worsen outcomes.
PNS Syndromes in Detail
Peripheral polyneuropathy affects 5–15% of lupus patients in most cohorts. The classic pattern is a slowly progressive, symmetrical, length-dependent sensory loss — numbness and tingling starting in the toes and creeping upward. A small-fiber variant produces burning pain and autonomic symptoms with normal nerve-conduction studies and requires a skin biopsy to confirm.
Mononeuropathy and mononeuritis multiplex (damage to one named nerve, or to several nerves in a random pattern) usually reflect true vasculitis of the small vessels feeding those nerves. It is a more aggressive presentation and typically warrants more aggressive immunosuppression.
Guillain-Barré syndrome (AIDP) — ascending weakness over days, areflexia, occasional respiratory failure — is rare in lupus but well documented. Treatment is the same as idiopathic GBS: IVIG or plasma exchange, plus ICU monitoring if respiration is threatened.
Autonomic disorder covers everything from orthostatic intolerance (lightheadedness on standing) to gastroparesis to bladder dysfunction. Tilt-table testing and autonomic function studies help document it objectively.
Plexopathy (damage to the brachial or lumbosacral plexus) is rare and usually presents as painful, asymmetric weakness of a whole limb.
Cranial neuropathies most often affect the facial nerve (Bell's palsy pattern), the trigeminal nerve (facial numbness), or the ocular motor nerves (double vision). Any new cranial neuropathy in a lupus patient earns an MRI with contrast to rule out inflammation in the brainstem or cavernous sinus.
Myasthenia gravis overlap — fatigable weakness, ptosis, diplopia, bulbar symptoms — is uncommon but well described. Both diseases are autoantibody driven, both run in autoimmune clusters, and rituximab can help both. For details on the underlying autoimmune neuromuscular junction disease, see the Myasthenia Gravis page.
The Attribution Problem — Primary vs Secondary
This is the central clinical decision in NPSLE, and it is harder than it sounds. "Primary" NPSLE means lupus itself is doing the neurologic damage — through inflammation, autoantibodies, vasculopathy, or thrombosis. "Secondary" NPSLE means the neurologic problem is real and the patient does have lupus, but the cause of the symptom is something else:
- Infection. Immunosuppressed lupus patients are vulnerable to meningitis, encephalitis, PML, listeria, cryptococcus, and opportunistic viruses. A confused, feverish lupus patient gets a lumbar puncture before anyone assumes it is a flare.
- Medication side effects. High-dose prednisone alone causes "steroid psychosis," mood swings, insomnia, and cognitive slowing. Hydroxychloroquine can rarely cause neuropsychiatric symptoms. Mycophenolate and cyclophosphamide can cause PRES (posterior reversible encephalopathy syndrome). NSAIDs and IVIG trigger aseptic meningitis. Opioids fog cognition.
- Metabolic and endocrine causes. Uremia from lupus nephritis, hyponatremia from SIADH, hypothyroidism, B12 deficiency, and hypoglycemia all produce neuropsychiatric symptoms in lupus patients and are cheap to rule out.
- Cardiovascular causes. Hypertensive emergencies, cardiac arrhythmias throwing emboli, and Libman-Sacks vegetations all produce neurologic events that look like NPSLE but require cardiology-led management.
- Psychosocial causes. Living with an unpredictable, painful, disfiguring autoimmune disease is, by itself, a cause of depression and anxiety that no immunosuppressant will fix.
The EULAR and ACR have published formal attribution models that score each neuropsychiatric episode on timing (did it start near the lupus diagnosis?), specificity (is this syndrome commonly seen in lupus?), and exclusion of alternative causes. Bortoluzzi and colleagues published a widely used Italian algorithm that classifies each event as attributed to lupus, unrelated, or uncertain. These tools are imperfect but they discipline the thinking and, crucially, they protect patients from being treated with cyclophosphamide for what turns out to be an infection.
Antiphospholipid Antibodies and Stroke
Roughly 30–40% of lupus patients carry antiphospholipid antibodies (aPL): lupus anticoagulant, anti-cardiolipin, and anti-beta-2-glycoprotein-I. These antibodies dramatically raise the risk of thrombotic events — deep vein thrombosis, pulmonary embolism, arterial clots, recurrent miscarriage, and, most relevant here, stroke, TIA, and cerebral venous sinus thrombosis.
A subset of lupus patients meet full criteria for secondary antiphospholipid syndrome (APS), which has its own management pathway: lifelong anticoagulation (usually warfarin with a target INR of 2–3 after venous events, or higher after arterial events) rather than lifelong immunosuppression. Direct oral anticoagulants (DOACs) like rivaroxaban have been shown to be inferior to warfarin in high-risk triple-positive APS and are generally avoided.
The practical consequence for NPSLE: every new focal neurologic event in a lupus patient earns an immediate aPL panel (if not already on file) plus vascular imaging. A stroke in a lupus patient with triple-positive aPL is a thrombotic event — it is treated with anticoagulation, not steroids. A stroke in a lupus patient with negative aPL and an active flare may instead be inflammatory and may need immunosuppression. Getting this distinction right matters enormously.
Ribosomal P and Lupus Psychosis
Anti-ribosomal P antibodies target three proteins (P0, P1, P2) on the 60S ribosomal subunit. They appear in 10–40% of lupus patients overall, and they have a specific clinical association with lupus psychosis and severe depression. The link was first described by Bonfa and colleagues in 1987 and has been replicated in multiple cohorts.
The association is not perfect — plenty of patients with anti-ribosomal P antibodies never develop psychosis, and some psychotic lupus patients test negative. But a positive anti-ribosomal P in a lupus patient with new psychiatric symptoms does shift the attribution meaningfully toward primary NPSLE and strengthens the case for immunosuppression. Ask your rheumatologist whether this antibody has been tested; it is not always included in standard panels.
Workup — MRI, CSF, EEG, Neuropsych
MRI of the brain with and without contrast is the first-line imaging study. Findings are often subtle or non-specific: small white-matter hyperintensities, cortical atrophy out of proportion to age, old infarcts, or — in active disease — new enhancing lesions. A normal MRI does not rule out NPSLE, particularly for cognitive dysfunction or mild psychiatric syndromes. MR angiography adds vessel imaging when stroke or vasculitis is suspected. MR venography is the test for cerebral venous sinus thrombosis.
Lumbar puncture and CSF analysis are essential when infection is on the table. In primary NPSLE, CSF may show mildly elevated protein, normal-to-mildly-elevated white cells (lymphocyte-predominant), normal glucose, and occasionally intrathecal production of IgG or oligoclonal bands. More importantly, CSF rules out bacterial meningitis, viral encephalitis, fungal infection, and carcinomatous meningitis. Nobody regrets a lumbar puncture in a confused, febrile lupus patient.
EEG is used when seizures, acute confusional state, or non-convulsive status epilepticus are suspected. Diffuse slowing is a non-specific but common finding in active NPSLE.
Formal neuropsychological testing is the gold standard for documenting cognitive dysfunction. A typical battery takes 2–4 hours and assesses attention, memory, processing speed, executive function, language, and visuospatial skills. The results establish a baseline, guide cognitive rehab, and document impairment for disability or accommodation purposes at work or school.
Bloodwork beyond the usual lupus panel should include CBC, comprehensive metabolic panel (including calcium, magnesium, phosphate), thyroid function, B12 and folate, ammonia (if encephalopathic), blood cultures (if febrile), and aPL panel. Anti-NMDA receptor antibodies, anti-MOG, and anti-aquaporin-4 are worth sending if the picture suggests encephalitis or a demyelinating syndrome.
Treatment — Immunosuppress vs Anticoagulate
NPSLE treatment forks at attribution. Once you have decided the event is primary and you have ruled out infection, the next fork is inflammatory vs thrombotic:
Inflammatory NPSLE (active flare, aseptic meningitis, myelitis, psychosis, severe cognitive decline, cranial neuropathy, cerebritis on MRI) is treated with immunosuppression. For severe or sight/life-threatening events the standard is IV methylprednisolone pulses (1 g daily for 3 days) followed by oral prednisone, plus an induction agent — usually cyclophosphamide or rituximab. Mycophenolate mofetil is increasingly used, particularly for maintenance. Belimumab and anifrolumab have growing roles as add-on therapy for moderate flares; see the biologics article.
Thrombotic NPSLE (stroke, TIA, venous sinus thrombosis in an aPL-positive patient) is treated with anticoagulation. Initial heparin transitions to warfarin with an INR target of 2–3 for venous events or 3–4 for arterial events. Aspirin alone is not enough for secondary stroke prevention in triple-positive APS. DOACs are generally avoided in high-risk APS.
Many patients need both: an active flare driving inflammation plus a hypercoagulable state driving clots. Combining anticoagulation with high-dose steroids raises bleeding risk and should be done with hematology input.
Specific syndromes have their own treatment notes:
- Seizures: standard anticonvulsants (levetiracetam is a common first choice, well tolerated with most immunosuppressants).
- Psychosis: antipsychotics plus immunosuppression. If the antibody signature fits, anti-ribosomal P positivity strengthens the case for aggressive immunotherapy.
- Mood and anxiety disorders: SSRIs or SNRIs, cognitive behavioral therapy, exercise, sleep hygiene. Not everything is a flare — a good therapist is often as important as the rheumatologist.
- Headache: standard migraine management (triptans, CGRP antagonists, magnesium, riboflavin). Sudden severe headache earns urgent imaging.
- Peripheral neuropathy: optimize lupus control, add gabapentin or duloxetine for neuropathic pain, screen for B12 and thyroid contributions.
- Myasthenic overlap: acetylcholinesterase inhibitors (pyridostigmine), plus immunosuppression coordinated between rheumatology and neurology.
Hydroxychloroquine stays on board through almost all of this. It reduces flare frequency, lowers thrombotic risk, improves lipid and glucose profiles, and is one of the few lupus drugs with a measurable survival benefit. See the hydroxychloroquine article for dosing and monitoring.
Cognitive Rehabilitation and Daily Life
Even after inflammation is controlled, many NPSLE patients have lingering cognitive symptoms. This is where cognitive rehabilitation — a structured, often under-prescribed intervention — earns its place.
- Speech-language pathology or occupational therapy with cognitive-rehab training: external strategies (written checklists, phone reminders, a daily planner) plus internal strategies (chunking, spaced repetition, single-tasking).
- Sleep is medicine. Untreated sleep apnea, insomnia, and fragmented sleep will mimic and amplify lupus fog. A sleep study is often the single highest-yield intervention.
- Aerobic exercise at moderate intensity most days of the week improves cognition measurably in lupus cohorts and has an antidepressant effect that rivals SSRIs for mild-to-moderate depression.
- Medication audit. Prednisone, opioids, benzodiazepines, anticholinergics, and some anticonvulsants all dull cognition. Review the full list with your rheumatologist and look for anything that could be de-prescribed or swapped.
- Accommodations. Under the Americans with Disabilities Act (ADA), documented cognitive dysfunction qualifies for workplace accommodations — extra time on deadlines, a quieter workspace, written rather than verbal task assignments, flexible start times. Students qualify under Section 504 and IDEA for similar accommodations. A formal neuropsych report is the paperwork that unlocks these.
- Mental health care. A therapist who understands chronic illness is not optional. Cognitive behavioral therapy reduces depression, anxiety, and disease-related catastrophizing and indirectly improves lupus self-management.
Red Flags — When to Go to the ER
Most NPSLE symptoms are chronic and can be worked up in clinic. Some are emergencies. Go to the emergency department now, not tomorrow, if you have:
- Sudden severe headache (thunderclap), especially with neck stiffness, vomiting, or confusion.
- Sudden weakness or numbness on one side of the body, slurred speech, facial droop, or vision loss (FAST criteria for stroke).
- First-ever seizure, or a cluster of seizures, or a seizure that lasts more than 5 minutes.
- Rapidly ascending weakness or numbness from the feet upward, or new bladder/bowel incontinence (possible transverse myelitis or GBS).
- Fever with confusion, stiff neck, or photophobia — meningitis until proven otherwise.
- New psychosis or suicidal thinking with a plan.
- Rapid cognitive decline over days to weeks (not months).
When you go, bring a current medication list, your rheumatologist's name, your most recent labs, and — importantly — the aPL result if you know it. That one data point changes the ER's approach to stroke and headache.
Prognosis and Long-Term Outlook
The prognosis of NPSLE depends enormously on which syndrome you have. Cognitive dysfunction, mood disorder, anxiety, and mild headache are chronic companions rather than progressive threats — they wax and wane but do not shorten life. Seizures are usually controllable and often resolve with lupus control. Peripheral neuropathies often stabilize and may partially recover.
Stroke, myelitis, severe cognitive decline, and psychosis carry more weight. NPSLE overall is associated with higher all-cause mortality in lupus cohorts, driven mostly by the cardiovascular and thrombotic burden. Aggressive control of lupus activity, hydroxychloroquine adherence, cardiovascular risk management, and — when indicated — anticoagulation measurably improve outcomes.
There is also genuine reason for optimism. Biologics (belimumab, anifrolumab, rituximab) have expanded the toolkit. Imaging is better. Attribution frameworks are sharper. Rehabilitation and mental-health integration are increasingly recognized as part of rheumatologic care rather than afterthoughts. Many NPSLE patients lead full lives, work, raise children, and hold down careers — often with accommodations, often with setbacks, rarely in isolation.
Key Research Papers
- ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999.
- Bertsias GK, et al. EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations. Ann Rheum Dis. 2010.
- Bortoluzzi A, et al. Development and validation of a new algorithm for attribution of neuropsychiatric events in systemic lupus erythematosus. Rheumatology (Oxford). 2015.
- Bonfa E, et al. Association between lupus psychosis and anti-ribosomal P protein antibodies. N Engl J Med. 1987.
- Hanly JG. Diagnosis and management of neuropsychiatric SLE. Nat Rev Rheumatol. 2014.
- Schreiber K, et al. Antiphospholipid syndrome. Lancet Neurol. 2018.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on NPSLE biology, attribution, and management:
- Neuropsychiatric lupus and the ACR 1999 nomenclature
- NPSLE attribution models and the Bortoluzzi algorithm
- Lupus cognitive dysfunction and neuropsychological testing
- Antiphospholipid syndrome, stroke, and lupus
- Anti-ribosomal P antibodies and lupus psychosis
- Lupus myelopathy and transverse myelitis treatment
- Lupus seizures, epilepsy, and long-term prognosis
- NPSLE imaging, CSF, and diagnostic workup
Connections
- Lupus Overview
- Stroke
- Myasthenia Gravis
- Biologics: Belimumab, Anifrolumab and Rituximab
- Hydroxychloroquine and Antimalarials
- ACR-EULAR 2019 Classification Criteria
- Lupus and Pregnancy
- Cutaneous Lupus and Photoprotection
- Lupus-Sjogren's Overlap
- ANA, dsDNA and Lupus Autoantibodies
- Lupus Nephritis and Kidney Involvement
- Sjogren's Syndrome
- Depression
- Anxiety
- Epilepsy
- Full Body MRI