Lupus and Sjögren's Overlap — Secondary Sjögren's Syndrome
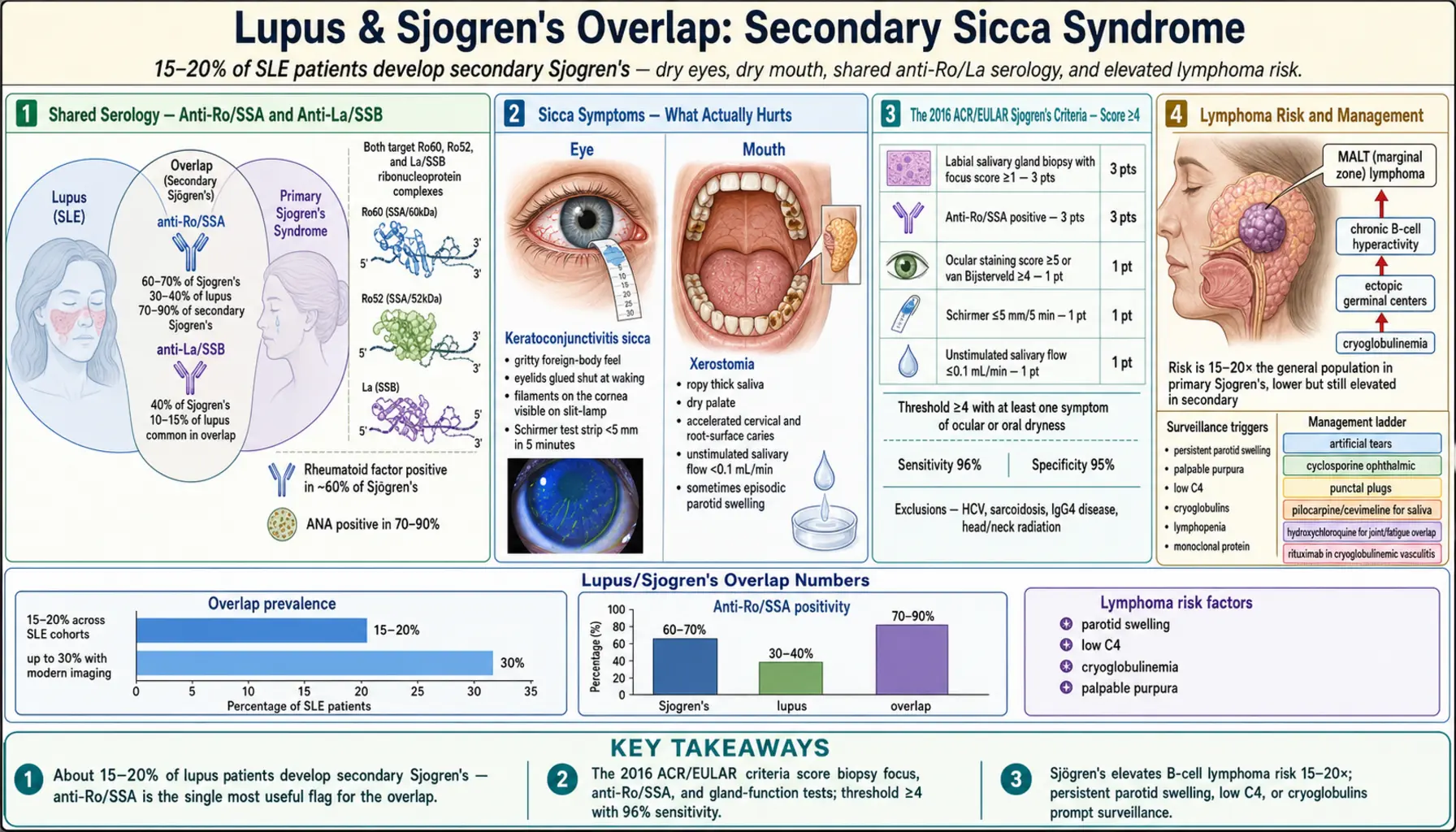
Table of Contents
- What Secondary Sjögren's Is
- How Often It Happens in Lupus
- Primary vs Secondary Sjögren's
- Shared Serology: Anti-Ro/SSA and Anti-La/SSB
- Sicca Symptoms — What You Feel
- The Diagnostic Workup Step by Step
- ACR/EULAR 2016 Classification Criteria
- Extraglandular Manifestations
- Lymphoma Risk and MALT
- Is It Sjögren's or a Drug Side Effect?
- Management — From Eye Drops to Rituximab
- Dental Decay Prevention
- Daily Life and Practical Tips
- Key Research Papers
- Connections
- Featured Videos
What Secondary Sjögren's Is
Sjögren's syndrome is a chronic autoimmune disease in which the immune system attacks the glands that make tears and saliva. The result is dry eyes and dry mouth — the "sicca" symptoms — along with a wider set of systemic problems ranging from joint pain to lung and kidney involvement. When Sjögren's appears on its own, it is called primary Sjögren's. When it appears in someone who already carries a diagnosis of another connective tissue disease — most commonly lupus (SLE), rheumatoid arthritis, or systemic sclerosis — it is called secondary Sjögren's.
The "secondary" label is not a judgment about severity. Secondary Sjögren's can be just as symptomatic, just as tissue-destructive, and just as exhausting as the primary form. It simply means your rheumatologist recognized lupus first and Sjögren's joined the picture afterward — or that the two were diagnosed close together, with lupus as the dominant disease driving your care.
For lupus patients, the overlap matters because it changes day-to-day quality of life, shifts a few pieces of the diagnostic puzzle, raises the long-term risk of B-cell lymphoma, and opens specific treatment options (like pilocarpine or punctal plugs) that plain lupus management does not usually address. See the Sjögren's Syndrome overview for the disease in isolation.
How Often It Happens in Lupus
Across published cohorts, roughly 15–20% of people with systemic lupus erythematosus develop secondary Sjögren's syndrome. Some single-center studies put the figure as high as 30% when modern salivary gland imaging is used liberally, and some as low as 9% when strict classification criteria are applied. The most widely cited meta-analyses land in the 14–18% range.
A few patterns stand out:
- Secondary Sjögren's tends to appear later in the lupus course — median onset about 7–10 years after the SLE diagnosis, though some patients carry both from the start.
- It is more common in older-onset lupus (women diagnosed after age 50) than in classic early-adult SLE.
- Women are affected about 9–20 times more often than men, mirroring the general female predominance of both diseases.
- Patients with secondary Sjögren's are more likely to carry anti-Ro/SSA antibodies, less likely to have severe renal disease, and more likely to have joint pain and Raynaud's than lupus patients without the overlap.
Primary vs Secondary Sjögren's
The distinction is clinical, not biochemical — the two forms share most of the same autoantibodies. But the differences matter for how rheumatologists frame treatment.
Primary Sjögren's patients tend to have more prominent glandular disease (severe xerostomia, parotid gland swelling), a higher frequency of anti-La/SSB antibodies, and a markedly elevated lymphoma risk (5–10% lifetime). Their therapy is organized around glandular symptoms and surveillance.
Secondary Sjögren's in lupus patients often has milder glandular symptoms but more active systemic inflammation driven by the underlying SLE. Anti-La/SSB is less common. The lymphoma risk is still elevated above the general population but appears lower than in primary Sjögren's. Therapy is organized around the dominant disease (lupus) with added attention to sicca symptoms.
One practical consequence: if you have lupus and develop new dry eyes and dry mouth, your rheumatologist may not immediately apply the full ACR/EULAR 2016 Sjögren's criteria — the label does not change whether you need artificial tears, pilocarpine, or intensified hydroxychloroquine. But a formal workup is worth doing once, because a confirmed diagnosis guides lymphoma surveillance and unlocks specific insurance coverage for cyclosporine ophthalmic drops and similar agents.
Shared Serology: Anti-Ro/SSA and Anti-La/SSB
Lupus and Sjögren's share an unusually tight serologic overlap. Two antibodies dominate the picture:
- Anti-Ro/SSA — present in roughly 60–70% of Sjögren's patients and 30–40% of lupus patients. In lupus patients with secondary Sjögren's, anti-Ro/SSA is present in 70–90%. It is the single most useful antibody for flagging the overlap.
- Anti-La/SSB — present in about 40% of primary Sjögren's but only 10–15% of lupus patients. When anti-La/SSB is present in an SLE patient, secondary Sjögren's is very likely.
Both antibodies target small nuclear ribonucleoprotein complexes — Ro60 and Ro52 for anti-SSA, and La/SSB for anti-La. They cross the placenta in pregnancy and are responsible for neonatal lupus and, in a small percentage, congenital heart block. If you are anti-Ro/SSA positive and planning pregnancy, your obstetrician needs to know — see the Lupus and Pregnancy page for monitoring protocols.
Rheumatoid factor is also frequently positive in Sjögren's (about 60%), and hypergammaglobulinemia (high total IgG) is common. A polyclonal elevation in IgG on an SPEP is a soft clue that Sjögren's may be active.
Sicca Symptoms — What You Feel
Dry eyes (keratoconjunctivitis sicca). Not simply "my eyes feel tired at the end of the day." Sjögren's dryness feels gritty, like sand under the eyelids. You may wake up with eyelids glued shut. Contact lenses become intolerable. Reading or screen work causes blurred vision that improves when you blink or use drops. In severe cases the cornea develops filaments — strands of mucus that stick to it — which an ophthalmologist can see on slit-lamp exam.
Dry mouth (xerostomia). Again, not simply "I get thirsty." Patients describe needing to sip water to swallow dry food, carrying a water bottle everywhere, waking at night to drink, and a thick ropy saliva that feels glue-like. Food sticks to the palate. Taste dulls. Speaking for long periods becomes effortful. Dental checkups start turning up new cavities in places you never had them before — particularly along the gumline and on the roots of teeth.
Other dry tissues. Sjögren's can affect every exocrine gland, not just eyes and mouth. Vaginal dryness is common and often under-reported. Dry skin, dry nasal passages (with nosebleeds), dry throat, and dry bronchi (chronic non-productive cough) are all part of the picture. Reflux worsens because saliva normally neutralizes esophageal acid.
Parotid and submandibular swelling. Episodic swelling of the large salivary glands in front of the ears or under the jaw. It can be painful, mimic mumps, and sometimes signals a secondary bacterial infection or, rarely, early lymphoma.
The Diagnostic Workup Step by Step
A complete Sjögren's workup layers objective tests on top of your symptom report. No single test is diagnostic; the picture is pieced together.
Schirmer test. A small strip of filter paper is tucked under the lower eyelid for five minutes. Less than 5 mm of wetting is abnormal and supports keratoconjunctivitis sicca. It is simple, cheap, and done in any ophthalmology office.
Ocular staining score. The ophthalmologist drops fluorescein and lissamine green onto the eye and grades areas of dead or damaged surface cells on a 0–12 scale per eye. A score of ≥5 in at least one eye is a positive ACR/EULAR criterion. This test picks up surface damage that Schirmer alone can miss.
Unstimulated whole-salivary flow (sialometry). You sit quietly and spit into a cup for five minutes. A flow of ≤0.1 mL/minute is abnormal. Simple, free, and surprisingly reproducible when done carefully.
Labial salivary gland biopsy. The gold standard. An oral surgeon or rheumatologist removes four to six tiny minor salivary glands from the inside of the lower lip under local anesthesia. A pathologist looks for focal lymphocytic sialadenitis and calculates the focus score — the number of focal lymphocytic aggregates (each containing ≥50 lymphocytes) per 4 mm² of tissue. A focus score of ≥1 is positive. The biopsy leaves a small internal stitch and usually heals in a week. It is the one piece of the workup that definitively confirms glandular autoimmunity when serology is ambiguous.
Salivary gland imaging. Ultrasound of the parotid and submandibular glands is increasingly used as a non-invasive first step; it shows characteristic hypoechoic foci that correlate well with biopsy. MRI and sialography are alternatives but less common in routine practice.
Blood work. ANA, anti-Ro/SSA, anti-La/SSB, rheumatoid factor, complete blood count (to look for cytopenias), SPEP and quantitative immunoglobulins, and a complement panel (C3, C4) if not already done as part of lupus monitoring. See the autoantibody article for how these fit into the broader lupus serology.
ACR/EULAR 2016 Classification Criteria
The 2016 American College of Rheumatology / European League Against Rheumatism criteria are the standard reference for classifying a patient as having Sjögren's syndrome in research and most clinical settings. You need a total score of ≥4 from the following items, in a patient who has at least one sicca symptom or a suggestive systemic feature:
- Labial salivary gland biopsy with focus score ≥1 — 3 points
- Anti-Ro/SSA positive — 3 points
- Ocular staining score ≥5 in at least one eye — 1 point
- Schirmer ≤5 mm/5 min in at least one eye — 1 point
- Unstimulated salivary flow ≤0.1 mL/min — 1 point
Exclusions include head and neck radiation, active hepatitis C, HIV, sarcoidosis, amyloidosis, graft-versus-host disease, and IgG4-related disease — each of which can mimic Sjögren's and must be ruled out first.
In a lupus patient, reaching a score of 4 is straightforward if you are anti-Ro/SSA positive (3 points) and have a positive Schirmer or ocular staining or salivary flow test (1 point). That is why serology plus a simple office test is usually enough — the biopsy is reserved for ambiguous cases.
Extraglandular Manifestations
Sjögren's is not just a dry mouth and dry eye disease. A meaningful minority of patients develop problems far from the salivary glands, and when these show up in a lupus patient, it can be hard to tell which disease is driving them.
- Cutaneous vasculitis. Palpable purpura on the legs, often associated with cryoglobulinemia. In a lupus patient, this overlaps with lupus vasculitis but the cryoglobulin pattern and tissue biopsy help sort it out.
- Peripheral neuropathy. Sensory neuropathy (burning feet, numbness, small-fiber loss) is the most common pattern. Sjögren's is one of the top autoimmune causes of small-fiber neuropathy, diagnosed by skin punch biopsy with intraepidermal nerve fiber density staining.
- Interstitial lung disease. Nonspecific interstitial pneumonia (NSIP) and lymphocytic interstitial pneumonia (LIP) are characteristic. Chronic dry cough plus a crackly exam plus a high-resolution chest CT is the usual path to diagnosis.
- Renal tubular acidosis. Distinct from lupus nephritis — Sjögren's classically causes type 1 (distal) renal tubular acidosis with hypokalemia, nephrocalcinosis, and kidney stones. Lupus nephritis is glomerular; Sjögren's kidney disease is tubulointerstitial. Both can coexist.
- Autonomic dysfunction. Some patients develop orthostatic intolerance, slow gastric emptying, or POTS-like features.
- Arthritis. Non-erosive polyarthritis very similar to lupus joint disease — see the Arthritis page.
- Raynaud's phenomenon. Extremely common in secondary Sjögren's, reported in 30–50% of patients. See Raynaud's Disease.
Lymphoma Risk and MALT
The most serious long-term complication of Sjögren's is non-Hodgkin B-cell lymphoma, most commonly mucosa-associated lymphoid tissue (MALT) lymphoma arising in the parotid gland. Primary Sjögren's patients have roughly a 5–10% lifetime risk, about 15–20 times the general population rate. In secondary Sjögren's overlapping with lupus, the risk appears lower but is still elevated — estimates range from 2–5% lifetime.
Known risk factors for lymphoma in Sjögren's:
- Persistent parotid gland swelling (especially unilateral)
- Palpable purpura or cryoglobulinemia
- Low C4 complement
- Lymphopenia or CD4+ T-cell lymphopenia
- Monoclonal gammopathy on SPEP
- High EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI) score
If you have any of these, your rheumatologist will watch you more closely — typically with an annual physical exam of the lymph nodes and salivary glands, and imaging (ultrasound or MRI) if a gland becomes persistently enlarged. A dominant salivary gland mass that does not resolve needs a biopsy, not reassurance. MALT lymphoma, when caught early and still confined to the gland, is highly treatable.
Is It Sjögren's or a Drug Side Effect?
Many medications cause dry mouth and dry eyes, and lupus patients are often on several of them at once. Before accepting a secondary Sjögren's label, it is worth reviewing the medication list. Common culprits:
- Antihistamines (diphenhydramine, cetirizine) — strong anticholinergic drying.
- Tricyclic antidepressants (amitriptyline, nortriptyline) — frequent cause of xerostomia.
- SSRIs and SNRIs (sertraline, venlafaxine) — milder but real.
- Diuretics (hydrochlorothiazide, furosemide) — dehydration-related dryness.
- Opioids — classic dry mouth.
- Anticholinergics for overactive bladder (oxybutynin, tolterodine).
- Beta blockers — decreased tear film in some patients.
- Isotretinoin — profoundly drying to all mucous membranes.
Drug-induced sicca is usually reversible within weeks of stopping the offending agent. Sjögren's is not. And importantly, drug-induced sicca does not produce a positive anti-Ro/SSA, a positive Schirmer with objective ocular surface damage on staining, or a focal lymphocytic biopsy. The distinction is clean when you do the objective tests.
Management — From Eye Drops to Rituximab
Treatment is built up in layers, matching intensity to symptoms and organ involvement.
Layer 1: environmental and over-the-counter measures. Preservative-free artificial tears four to six times daily (Refresh Optive, Systane, TheraTears). Nighttime gel or ointment (Refresh Lacri-Lube, GenTeal Gel). A humidifier by the bed. Wraparound sunglasses outdoors. Frequent sips of water through the day. Sugar-free xylitol gum or lozenges to stimulate residual saliva.
Layer 2: prescription eye drops.
- Cyclosporine 0.05% ophthalmic (Restasis) or 0.09% (Cequa) — suppresses local T-cell inflammation on the ocular surface. Takes 3–6 months to reach full effect. Burns on instillation for the first few weeks.
- Lifitegrast 5% (Xiidra) — blocks a different inflammatory pathway (LFA-1/ICAM-1). Faster onset than cyclosporine.
- Punctal plugs. Tiny silicone or collagen plugs inserted into the tear drainage ducts by an ophthalmologist. Keeps your own tears (and any drops) on the eye surface longer. Collagen plugs dissolve in weeks; silicone plugs are semi-permanent.
Layer 3: secretagogues for dry mouth.
- Pilocarpine (Salagen), 5 mg four times daily. A muscarinic agonist that stimulates residual salivary tissue. Side effects: sweating, flushing, frequent urination, sometimes GI cramping. Start with 2.5 mg to test tolerance.
- Cevimeline (Evoxac), 30 mg three times daily. More selective for M3 receptors on salivary glands with somewhat less systemic cholinergic effect. Often better tolerated than pilocarpine.
Layer 4: systemic disease-modifying therapy.
- Hydroxychloroquine (Plaquenil) — most lupus patients with secondary Sjögren's are already on it. Modest benefit for sicca symptoms and clear benefit for joint pain and fatigue. See the HCQ article.
- Methotrexate, azathioprine, mycophenolate — used when systemic or extraglandular features (arthritis, ILD, vasculitis) dominate. Chosen by the SLE picture more than the Sjögren's picture.
- Rituximab — anti-CD20 B-cell depletion. Reserved for refractory extraglandular disease: severe cryoglobulinemic vasculitis, progressive ILD, significant neuropathy, or MALT lymphoma. Trials in unselected Sjögren's (TEARS, TRACTISS) showed mixed results for glandular symptoms but clearer benefit in subgroups with active systemic disease. See the biologics article.
- Belimumab — primarily used for lupus activity; emerging data in Sjögren's, especially in combination with rituximab.
NSAIDs and short corticosteroid courses are used for joint flares as in lupus. Chronic high-dose steroids are avoided — they do not help sicca and carry the usual bone, skin, and infection risks.
Dental Decay Prevention
Saliva is the mouth's natural defense against cavities. Without it, tooth decay accelerates dramatically — patients can go from no cavities to multiple root caries within a year or two. Aggressive prevention matters more than any medication.
- See your dentist every 3–4 months, not the usual 6. Ask them to note "Sjögren's / xerostomia" in your chart so they know the stakes.
- High-fluoride prescription toothpaste — 1.1% sodium fluoride (5000 ppm) such as Prevident or Clinpro 5000. Use nightly after brushing; spit but do not rinse.
- Daily fluoride rinse or custom fluoride trays for 5-minute nightly applications in high-risk patients.
- Xylitol — gum, mints, or lozenges 5–6 times daily. Xylitol is a sugar alcohol that cavity-causing bacteria cannot metabolize; regular exposure lowers bacterial counts.
- Avoid constant sipping of acidic drinks — sparkling water, lemon water, diet sodas. They strip enamel in a dry mouth. Stick to plain water or drink acidic beverages through a straw and rinse with water afterward.
- Saliva substitutes and sprays (Biotène, Xylimelts) overnight for comfort and buffering.
- Monitor for oral candidiasis — a red, sore tongue with cracked corners of the mouth. Treat promptly with nystatin or fluconazole; it will not clear on its own in a dry mouth.
Daily Life and Practical Tips
- Hydrate strategically. Sipping water constantly actually washes out the small amount of saliva and mucin you have. Sip enough to stay comfortable, but rely on secretagogues and xylitol to keep the mouth moist rather than volume of water.
- Humidify the bedroom. Running a cool-mist humidifier overnight dramatically improves morning eye and mouth symptoms. Clean weekly to prevent mold.
- Protect the eyes outdoors. Wraparound sunglasses cut tear evaporation from wind. In very dry climates or on airplanes, moisture chamber goggles (7eye, Ziena) help.
- Lubricate before screens. Drop artificial tears before starting computer work, not after your eyes already sting. Set a timer to blink fully every 20 minutes.
- Plan around flares. Long flights, dry air-conditioned offices, and winter heating all worsen sicca. Bring your drops everywhere; they are never "optional."
- Vaginal dryness is treatable. Local vaginal moisturizers (Replens, Hyalo Gyn) and, when appropriate, low-dose vaginal estrogen are safe and effective. Bring it up with your rheumatologist or gynecologist — most patients never volunteer the symptom.
- Track new symptoms. Persistent unilateral salivary gland swelling, unexplained weight loss, drenching night sweats, or new enlarged lymph nodes are lymphoma warning signs. Do not sit on them.
Key Research Papers
- Shiboski CH, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren's Syndrome. Arthritis Rheumatol. 2017.
- Ramos-Casals M, et al. EULAR recommendations for the management of Sjögren's syndrome with topical and systemic therapies. Ann Rheum Dis. 2020.
- Brito-Zerón P, et al. Sjögren syndrome. Nat Rev Dis Primers. 2016.
- Baer AN, et al. The SSB-positive/SSA-negative antibody profile is not a reliable marker for primary Sjögren's syndrome. Ann Rheum Dis. 2015.
- Nocturne G, Mariette X. Sjögren syndrome-associated lymphomas: an update on pathogenesis and management. Br J Haematol. 2015.
- Devauchelle-Pensec V, et al. Treatment of primary Sjögren syndrome with rituximab: the TEARS randomized trial. Ann Intern Med. 2014.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on lupus-Sjögren's overlap, diagnosis, and management:
- Secondary Sjögren's in systemic lupus erythematosus
- Anti-Ro/SSA and anti-La/SSB in lupus and Sjögren's
- Labial salivary gland biopsy and focus score
- ACR/EULAR 2016 Sjögren's classification criteria
- Sjögren's and MALT lymphoma risk
- Pilocarpine and cevimeline for xerostomia
- Rituximab in Sjögren's syndrome trials
- Renal tubular acidosis in Sjögren's
- Interstitial lung disease in Sjögren's
- Xerostomia and dental caries prevention
Connections
- Lupus Overview
- Sjogren's Syndrome
- Arthritis
- Raynaud's Disease
- Biologics: Belimumab, Anifrolumab and Rituximab
- ANA, dsDNA and Lupus Autoantibodies
- Hydroxychloroquine and Antimalarials
- Lupus and Pregnancy
- Neuropsychiatric Lupus
- ACR-EULAR 2019 Classification Criteria
- Cutaneous Lupus and Photoprotection
- Lupus Nephritis and Kidney Involvement
- Lymphoma
- Kidney Disease
- Interstitial Lung Disease