NSAID Strategy for Ankylosing Spondylitis
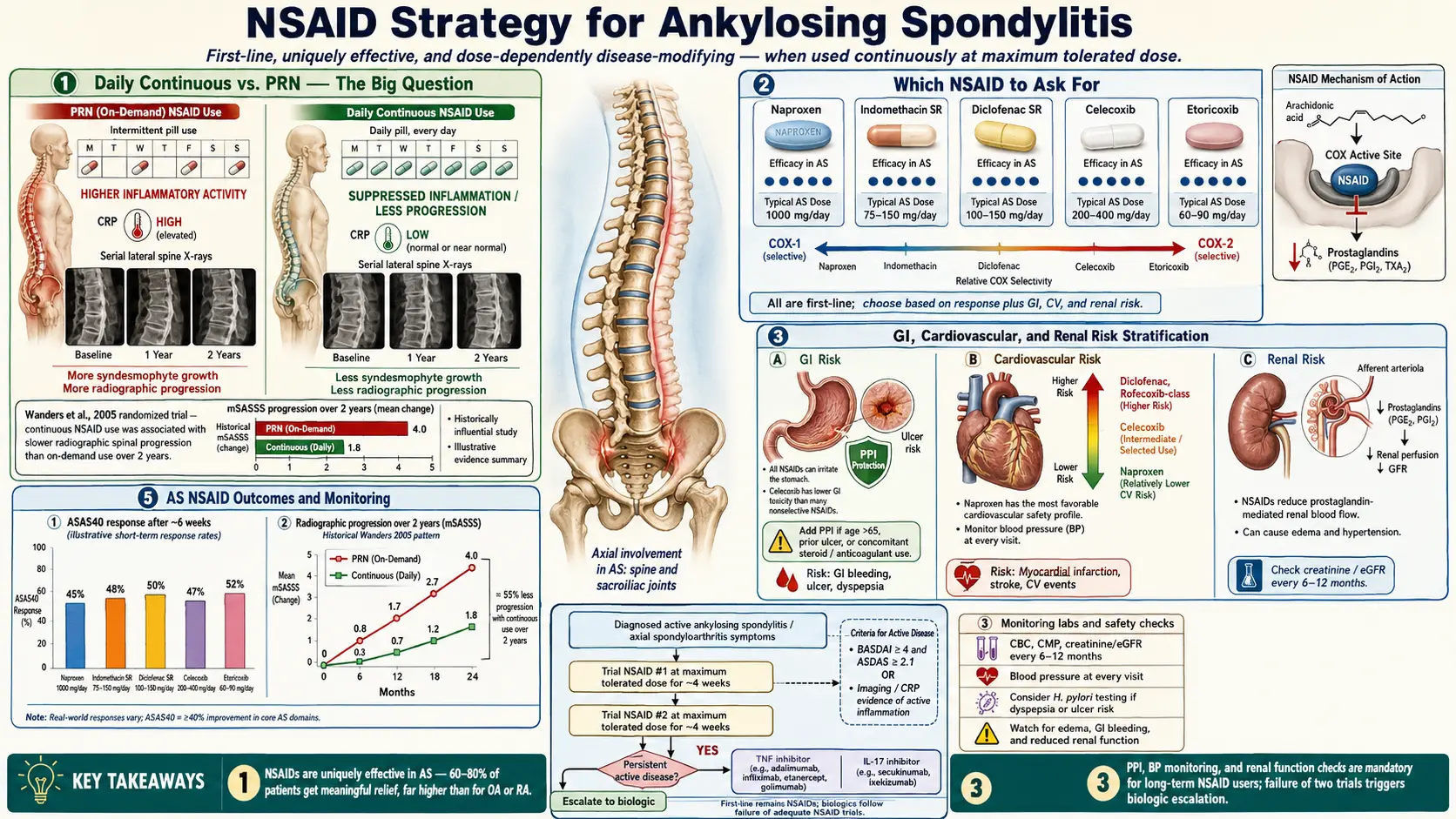
Table of Contents
- NSAIDs Are First-Line for AS — And More Effective Than for Other Arthritides
- Daily Continuous vs. PRN — The Big Question
- Which NSAID to Ask For — Drug-by-Drug
- Trial-and-Error Reality
- Dosing for AS Specifically
- GI Protection — Critical for Long-Term NSAID Users
- Cardiovascular Risk
- Renal Risk
- Other Side Effects
- NSAID Failure — When to Escalate to Biologics
- NSAIDs + Biologics
- Topical NSAIDs — Adjunct Option
- Acetaminophen + NSAIDs
- Alternative Anti-Inflammatories
- Monitoring Schedule
- NSAIDs in Pregnancy
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. NSAIDs Are First-Line for AS — And More Effective Than for Other Arthritides
One of the diagnostic clues for ankylosing spondylitis is that the inflammatory back pain responds unusually well to NSAIDs — more reliably, and more dramatically, than back pain from mechanical causes or even most other inflammatory arthritides. Most AS patients see greater than 50% pain reduction within 48 hours of starting a therapeutic dose.
The corollary matters clinically: if you have suspected AS and you don’t respond meaningfully to a full-dose NSAID after two weeks of an adequate dose, the diagnosis should be reconsidered before assuming you’re an NSAID non-responder. Seronegative fibromyalgia, mechanical back pain, and non-radiographic axial SpA in its earliest stages can mimic AS but don’t share the same robust NSAID response.
This is why every major guideline — ACR/SAA/SPARTAN 2019, ASAS-EULAR 2022 — lists NSAIDs as the first-line pharmacologic therapy for active AS. Before biologics, before DMARDs, before anything injectable, you try NSAIDs properly first.
2. Daily Continuous vs. PRN — The Big Question
Every AS patient eventually asks this: should I take my NSAID every day no matter what, or only when I’m hurting? For most of the 2000s and early 2010s, the answer was “every day, forever, to slow the fusion.” That answer has quietly shifted.
- Wanders 2005 trial (N=215) compared continuous daily celecoxib vs. on-demand use over 2 years and found less radiographic progression in the continuous group. This single trial defined the “take it every day” dogma for over a decade.
- ENRADAS trial (Sieper 2016), a larger and better-controlled RCT using diclofenac, did not replicate the Wanders finding. Continuous dosing showed no radiographic advantage over PRN.
- Current guidelines (ACR/SAA 2019, ASAS-EULAR 2022) recommend NSAIDs as needed for symptom control. Continuous dosing is not required solely to slow progression in the absence of active symptoms.
Practical stance: take NSAIDs daily if you have daily symptoms. Use PRN dosing if your symptoms are intermittent. Do not force daily NSAIDs on an asymptomatic patient just in case. The GI, cardiovascular, and renal risks of chronic dosing outweigh the uncertain radiographic benefit in quiescent disease.
3. Which NSAID to Ask For — Drug-by-Drug
Meloxicam (Mobic)
Dose: 7.5–15 mg daily. Once-daily dosing with the longest half-life among common NSAIDs (15–20 hours), which gives consistent 24-hour coverage from a single pill. Moderate COX-2 selectivity puts GI risk between ibuprofen and celecoxib. A very common starting choice in AS because of the convenient dosing and balanced profile.
Naproxen (Aleve, Naprosyn)
Dose: 500 mg twice daily. Cheap, OTC at lower strengths, long half-life. Critically, naproxen has the best cardiovascular safety profile of any NSAID — the lowest MI and stroke risk in large meta-analyses. First choice for AS patients with known cardiovascular disease or elevated CV risk.
Celecoxib (Celebrex)
Dose: 200 mg daily or twice daily. A selective COX-2 inhibitor, which means the lowest GI ulcer and bleeding risk among NSAIDs. Preferred in patients with prior ulcer disease or concurrent inflammatory bowel disease (see AS and IBD Overlap) — unlike traditional NSAIDs, celecoxib does not appear to flare IBD. Cardiovascular risk is slightly higher than naproxen but comparable to ibuprofen at approved doses.
Indomethacin (Indocin)
Dose: 25–50 mg three to four times daily. Historically considered the most potent NSAID for AS specifically, and still the one many older rheumatologists reach for when others fail. The downside is a higher rate of GI toxicity and CNS side effects — headache, dizziness, and a “spaced-out” feeling are common. Often tried as a third-line NSAID after meloxicam and naproxen.
Diclofenac (Voltaren)
Dose: 75 mg twice daily (or 50 mg TID). Effective but carries the highest cardiovascular risk of the common NSAIDs — comparable in some analyses to the withdrawn rofecoxib. Oral diclofenac is not a first choice for AS in 2026. The topical gel, however, is genuinely useful for enthesitis (see section 12).
Ibuprofen (Advil, Motrin)
Dose: 400–800 mg three to four times daily. OTC, cheap, familiar. Reasonable as a first trial but the TID–QID dosing is inconvenient and GI risk at the doses needed for AS is higher than meloxicam or celecoxib. Most patients end up switching.
Etoricoxib (Arcoxia)
Dose: 60–90 mg daily. Highly COX-2 selective, strong evidence in AS specifically, widely used in Europe, UK, and Canada. Not FDA-approved in the US — if you’re in the States and you read about this drug in a European paper, your rheumatologist cannot prescribe it.
Piroxicam (Feldene)
Dose: 20 mg daily. Very long half-life allows once-daily dosing, but elevated GI and cardiovascular risk relative to alternatives. Rarely a first choice now.
4. Trial-and-Error Reality
Here is the part no trial result captures well: different AS patients respond best to different NSAIDs in a way that is largely idiosyncratic. Two patients with identical imaging and identical CRP can have dramatically different responses to, say, meloxicam vs. indomethacin. The genetic and pharmacokinetic reasons are still not fully understood.
The standard approach is therefore empirical:
- Try one NSAID for 2–4 weeks at the maximum tolerated dose.
- If response is inadequate, switch to a structurally different NSAID — don’t just substitute one propionic acid derivative for another.
- Most rheumatologists recommend trialing 2–3 different NSAIDs before declaring true NSAID failure and escalating to biologics.
Keep a simple symptom log during each trial: morning stiffness duration, nighttime awakenings, BASDAI-style global score. Without data, the “did this actually help?” question gets very fuzzy by week three.
5. Dosing for AS Specifically
AS doses often run higher than the doses used for rheumatoid arthritis or osteoarthritis:
- Meloxicam: max 15 mg daily (vs RA typical dose 7.5 mg)
- Naproxen: 500 mg BID continuous
- Celecoxib: 200 mg BID for active disease (not just 200 mg QD)
- Indomethacin: 150–200 mg/day divided
- Ibuprofen: 2400–3200 mg/day divided
Evening dosing is the underused trick. The classic AS inflammatory pattern is pain and stiffness worst in the second half of the night — the 3 AM wakeup. A bedtime NSAID dose (or the largest dose of the day shifted to bedtime) covers that window and dramatically reduces morning stiffness. See Morning Stiffness Management.
6. GI Protection — Critical for Long-Term NSAID Users
Chronic NSAID use causes gastric and duodenal ulcers. The annual ulcer complication rate (bleeding, perforation, obstruction) on traditional NSAIDs is roughly 1–2%, with cumulative risk rising each year. If you’re on NSAIDs for AS, you need a plan.
- Proton pump inhibitors (PPIs) are the cornerstone: omeprazole 20–40 mg, pantoprazole 40 mg, or esomeprazole 20–40 mg once daily. PPIs reduce NSAID-induced ulcers by 80–90%.
- Misoprostol (Cytotec) works mechanistically but is rarely used now — diarrhea and cramping limit tolerability.
- Celecoxib’s COX-2 selectivity gives it roughly half the ulcer rate of traditional NSAIDs, and many patients on celecoxib monotherapy without high GI risk factors can skip the PPI.
- H. pylori eradication before chronic NSAIDs: test and treat if positive. H. pylori + NSAIDs is a synergistic ulcer machine.
The PPI caveat. Long-term PPIs are not free. Documented issues include vitamin B12 deficiency, reduced calcium absorption and fracture risk, hypomagnesemia, increased enteric infection rates, and small intestinal bacterial overgrowth — see SIBO. Periodic “PPI holidays” after 6–12 months of trouble-free NSAID use are reasonable in patients without a prior ulcer history.
7. Cardiovascular Risk
All NSAIDs except aspirin raise the risk of myocardial infarction, stroke, and heart failure to varying degrees.
- Lowest risk: naproxen
- Moderate risk: ibuprofen, celecoxib at FDA-approved doses
- Highest risk: diclofenac, rofecoxib (withdrawn 2004)
Absolute risk increase: roughly 0.5–1% additional cardiovascular event per year in average-risk patients, and considerably higher in those with established cardiovascular disease. For a 30-year-old with no CV risk factors, this is small. For a 65-year-old post-MI patient, it is not.
If you have cardiovascular disease and you need an NSAID for AS, naproxen or celecoxib 200 mg/day at the lowest effective dose is the usual compromise. Have the conversation with your cardiologist, not just your rheumatologist.
8. Renal Risk
NSAIDs reduce renal blood flow by inhibiting prostaglandin-mediated afferent arteriolar vasodilation. In healthy kidneys this is usually tolerated; in borderline kidneys it precipitates injury.
- Baseline creatinine and eGFR before starting chronic NSAID therapy.
- Annual creatinine + eGFR during chronic use — more often in older patients or those on diuretics or ACE inhibitors.
- Stop the NSAID if: eGFR drops more than 30%, acute kidney injury develops, or new proteinuria appears.
- Contraindicated: CKD stage 4–5, cirrhosis with ascites, heart failure stage C–D.
- Hydrate. Adequate water intake is protective; dehydration plus NSAID plus diuretic is the classic AKI setup.
9. Other Side Effects
- Hypertension: all NSAIDs raise blood pressure by an average of 2–5 mmHg. Monitor if borderline or treated hypertension.
- NSAID-exacerbated respiratory disease: about 10% of asthmatics get bronchospasm from aspirin/NSAIDs. Celecoxib is usually tolerated even in these patients.
- Bleeding risk: additive with anticoagulants, antiplatelets, SSRIs. Re-check the med list.
- Tinnitus: dose-related; classic with high-dose salicylates but possible with any NSAID.
- Rash: occasional. Celecoxib carries a boxed warning about sulfa cross-reactivity, but actual cross-reactivity in sulfa-allergic patients is minimal in practice.
10. NSAID Failure — When to Escalate to Biologics
The criteria for moving from NSAIDs to biologics (TNF inhibitors, IL-17 inhibitors, JAK inhibitors) are well defined:
- Inadequate response after 2 different NSAIDs at maximum tolerated dose for 2–4 weeks each, OR
- Active disease markers — elevated CRP, BASDAI > 4 — despite NSAIDs, OR
- Intolerable side effects preventing adequate dosing, OR
- Peripheral arthritis, enthesitis, or dactylitis inadequately controlled by NSAIDs.
Realistic time from starting NSAIDs to starting a biologic in a patient who ultimately needs one: 2–6 months. Don’t spend two years cycling NSAIDs while radiographic damage progresses. See Biologics Guide.
11. NSAIDs + Biologics
Starting a biologic does not mean stopping NSAIDs. Combined treatment is standard, especially in the first 12–16 weeks while the biologic takes full effect. Many patients can later reduce the NSAID dose — or drop it to PRN — once the biologic brings BASDAI and CRP down. Others stay on both indefinitely for symptom control.
12. Topical NSAIDs — Adjunct Option
- Diclofenac gel 1% (Voltaren) — now OTC; useful for localized enthesitis (heel, Achilles, lateral epicondyle, knee).
- Diclofenac patches (Flector) 1.3% — prescription; convenient for a single painful joint.
Topicals deliver local drug concentrations with a small fraction of systemic exposure, sparing you most of the GI, CV, and renal risk. The limitation is that topicals don’t reach the axial spine or sacroiliac joints adequately — they’re a good add-on for peripheral symptoms, not a replacement for oral NSAIDs in axial disease.
13. Acetaminophen + NSAIDs
Acetaminophen (paracetamol) alone is inadequate for AS. AS is an inflammatory disease, and acetaminophen has essentially no anti-inflammatory action — it doesn’t meaningfully reduce swelling, stiffness, or radiographic progression.
It is, however, a reasonable add-on for breakthrough pain: 500–1000 mg PRN, max 3 g/day (the old 4 g ceiling has been revised downward by most hepatology guidance). Think of it as a bridge for bad days, not as disease-modifying.
14. Alternative Anti-Inflammatories
- Turmeric / curcumin standardized to 95% curcuminoids, 500 mg BID–TID. Modest anti-inflammatory effect in trials — gentler than prescription NSAIDs, nowhere near as potent. See Turmeric.
- Boswellia serrata standardized to boswellic acids. Similar story — real but modest effect. See Boswellia.
- Omega-3 fatty acids 2–4 g EPA+DHA daily — modest anti-inflammatory, also cardioprotective, which pairs well with the CV considerations above.
These are adjuncts, not substitutes. In active AS with high CRP, they will not control the disease on their own. They may let you run at a slightly lower NSAID dose.
15. Monitoring Schedule
- Before starting: CBC, CMP, eGFR, LFTs, blood pressure.
- 1 month in: CBC and creatinine to catch early problems.
- Every 6 months: CBC, CMP, eGFR, LFTs.
- Annually: H. pylori testing if chronic NSAIDs without PPI; blood pressure check.
- Symptom red flags — stop NSAID and seek urgent evaluation: black or tarry stool, coffee-ground emesis, new iron-deficiency anemia, severe abdominal pain, marked ankle swelling, sharp drop in urine output.
16. NSAIDs in Pregnancy
NSAIDs are contraindicated in the third trimester because they can cause premature closure of the fetal ductus arteriosus, oligohydramnios, and neonatal renal dysfunction. First and second trimester use is usually avoided if possible and kept to short courses when necessary. Acetaminophen is the safer analgesic during pregnancy. See Pregnancy and AS for the full pregnancy-specific medication strategy.
17. Key Research Papers
- Wanders A, et al. Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis & Rheumatism. 2005;52(6):1756-1765.
- Sieper J, et al. Effect of continuous versus on-demand treatment of ankylosing spondylitis with diclofenac over 2 years on radiographic progression of the spine (ENRADAS). Annals of the Rheumatic Diseases. 2016;75(8):1438-1443.
- Ward MM, et al. 2019 Update of the ACR/SAA/SPARTAN Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. 2019.
- Ramiro S, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Annals of the Rheumatic Diseases. 2023.
18. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: NSAID in ankylosing spondylitis
- PubMed: Celecoxib in axial spondyloarthritis
- PubMed: NSAIDs and radiographic progression in spondyloarthritis
- PubMed: Indomethacin in ankylosing spondylitis
- PubMed: NSAID gastrointestinal protection
- PubMed: COX-2 selective inhibitors and cardiovascular risk
- PubMed: Naproxen cardiovascular safety
- PubMed: Meloxicam in spondyloarthritis
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- Exercise and PT Protocol
- Morning Stiffness Management
- Starch-Free Diet and Ebringer
- Pregnancy and AS
- Uveitis and Eye Involvement
- Arthritis
- Peptic Ulcer Disease
- SIBO
- Cardiovascular Disease
- eGFR Kidney Function
- Inflammatory Markers
- Turmeric