Pregnancy and Ankylosing Spondylitis
Pregnancy with AS is different from pregnancy with rheumatoid arthritis — and if you have been told it would all get better once you conceived, only to find your back pain worsening at 22 weeks, you are not imagining it and you are not failing. The old obstetric reassurance — "autoimmune disease improves in pregnancy" — was built on RA data. It does not reliably apply to spondyloarthritis. This article walks through what to actually expect, which medications stay and which go, how to plan delivery, and how to survive the postpartum period without a catastrophic flare.
Table of Contents
- Why AS Pregnancy Is Different From RA Pregnancy
- Pre-Conception Planning
- NSAIDs in Pregnancy
- Biologics in Pregnancy
- The 2020 EULAR Points to Consider
- Managing Flares When Most Drugs Are Off the Table
- Hip, Pelvis, and Spine Mechanics
- Sleep Positioning
- Delivery Planning
- Postpartum Flare Risk
- Breastfeeding and Medications
- Fertility — Yours and His
- Genetic Counseling and Your Baby’s Risk
- Mental Health, Sleep Loss, and PPD
- Key Research Papers
- Connections
- Featured Videos
Why AS Pregnancy Is Different From RA Pregnancy
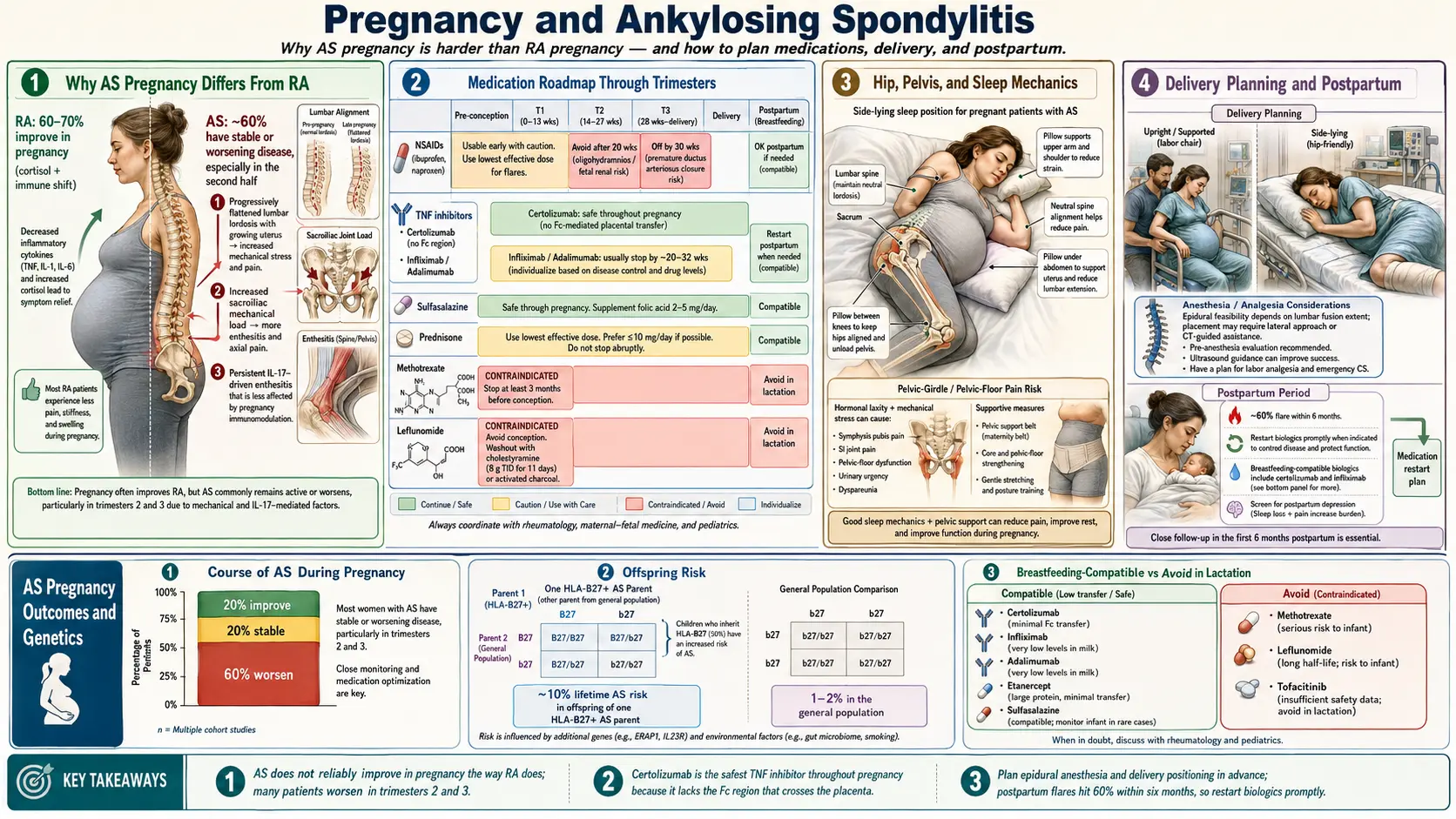
For decades, rheumatology textbooks taught a simple rule: autoimmune disease improves in pregnancy because the maternal immune system shifts from a Th1 to a Th2 pattern to tolerate the fetus. That rule was built almost entirely on rheumatoid arthritis, where about 60% of patients do improve, often dramatically, by the second trimester.
Ankylosing spondylitis does not follow the same pattern. In the best prospective data we have, roughly 60% of AS patients report unchanged or worsening disease activity during pregnancy, about 20% improve, and the rest fluctuate. The classic worsening window is the 20–28 week range, when mechanical load on the pelvis peaks, inflammatory back pain is magnified by a loosened symphysis and sacroiliac joints, and many patients have already stopped NSAIDs.
Why the difference? Two likely reasons. First, AS is driven largely by the IL-23/IL-17 axis, which is not as strongly suppressed by pregnancy hormones as the Th1/TNF pathways that dominate RA. Second, much of AS pain is mechanical on top of inflammatory — the sacroiliac joints and lumbar spine take far more direct strain from a growing uterus than the small joints of the hands.
If you were counseled that pregnancy would be a "break" from your AS and it has not been, your disease is behaving normally. The mismatch is in the counseling, not in you.
Pre-Conception Planning
Ideally, planning begins three to six months before conception. Active, uncontrolled AS at the time of conception correlates with more difficult pregnancies and higher rates of preterm birth and low birth weight. The goal is low disease activity (ASDAS < 2.1 or BASDAI < 4) for at least three months, preferably six, before trying.
A practical pre-conception checklist:
- Medication review with your rheumatologist. Methotrexate must be stopped at least three months before conception (teratogenic). Leflunomide requires cholestyramine washout. Sulfasalazine, hydroxychloroquine, azathioprine, and most TNF inhibitors can continue. JAK inhibitors (tofacitinib, upadacitinib) must be stopped.
- Switch to a pregnancy-compatible biologic in advance if you are on something less well-studied. Moving to certolizumab pegol three months before trying gives you time to confirm it is controlling your disease.
- Folate — at least 400 mcg daily, 800 mcg if you have been on sulfasalazine (which interferes with folate metabolism). Start three months before conception.
- Vitamin D — check a 25-OH vitamin D level and replete to at least 30 ng/mL. AS patients are frequently low.
- DXA scan if you have had long-term NSAID use, prior prednisone, or baseline low body weight. Pregnancy and lactation both transiently reduce bone density, and AS patients are already at higher fracture risk.
- Book a maternal-fetal medicine (MFM) consultation and line up a rheumatologist who is comfortable managing biologics in pregnancy. Co-management is the standard of care; neither specialty should be making these calls alone.
NSAIDs in Pregnancy
NSAIDs — the backbone of day-to-day AS management — become the single biggest medication question of pregnancy.
First trimester and early second trimester (up to roughly 20 weeks). Short-course, lowest-effective-dose NSAIDs (ibuprofen, naproxen, diclofenac) are generally considered acceptable if truly needed, though some guidelines now recommend minimizing use even in early pregnancy. There is a small, debated signal for first-trimester miscarriage risk with sustained use. Intermittent, symptom-driven dosing is safer than daily scheduled therapy.
After 20 weeks. Avoid. In October 2020, the FDA issued a Drug Safety Communication recommending against NSAID use after 20 weeks of gestation due to the risk of fetal renal dysfunction leading to oligohydramnios (low amniotic fluid). This can develop within days of initiating NSAID therapy and may be reversible if the drug is stopped promptly, but it is not worth gambling on. The prior cutoff was 30 weeks; the FDA moved it ten weeks earlier after accumulating case reports.
After 30 weeks. Absolutely avoid. NSAIDs cause premature closure of the ductus arteriosus, a critical fetal vessel. Closure in utero can cause fetal heart failure and pulmonary hypertension in the newborn.
Low-dose aspirin (81 mg) is a separate category — it is actually used in pregnancy for preeclampsia prevention and has a different safety profile than therapeutic NSAIDs. Do not confuse the two.
The practical upshot: plan for a 20-week NSAID cliff and make sure your non-NSAID strategy is in place well before you reach it.
Biologics in Pregnancy
This is where the last decade of research has changed the game. Several TNF inhibitors now have enough human pregnancy data to be considered compatible throughout pregnancy, and one — certolizumab pegol — has a structural advantage that makes it the de facto first choice when a woman with AS is planning or already pregnant.
TNF Inhibitors
- Certolizumab pegol (Cimzia) — preferred throughout pregnancy. Certolizumab is a Fab′ fragment attached to polyethylene glycol; it lacks the Fc portion of a normal IgG antibody. Placental transfer of IgG uses the neonatal Fc receptor (FcRn), so no Fc means almost no active transport to the fetus. The prospective CRIB study (Forger et al, 2018) measured certolizumab in 16 mother-infant pairs and found minimal to no drug in cord blood and infant serum at birth. Continuing certolizumab to delivery is reasonable.
- Etanercept (Enbrel) — compatible; lower placental transfer than adalimumab or infliximab because of structural differences, though it still crosses via FcRn in the third trimester. Often continued through the second trimester and sometimes to delivery.
- Adalimumab (Humira) and infliximab (Remicade) — compatible through conception and most of pregnancy. They are complete IgG1 antibodies and are actively transported across the placenta in the third trimester, so infant drug levels at birth can exceed maternal levels. Many rheumatologists stop adalimumab around 28–32 weeks and infliximab around 20–24 weeks to minimize neonatal exposure, but continuing if disease activity demands it is acceptable. The main implication is the infant vaccination schedule: avoid live vaccines (rotavirus, BCG) for the first 6 months of life when the mother was on a full-transfer TNF inhibitor in the third trimester.
- Golimumab (Simponi) — limited data, generally avoided when alternatives exist.
IL-17 Inhibitors
Secukinumab (Cosentyx) and ixekizumab (Taltz) — limited human pregnancy data. Current EULAR guidance recommends stopping before conception or as soon as pregnancy is confirmed unless the benefit clearly outweighs the uncertainty. If your AS is controlled only by an IL-17 inhibitor, have a serious pre-conception conversation about switching to certolizumab for the pregnancy and resuming the IL-17 drug postpartum.
JAK Inhibitors
Tofacitinib, upadacitinib, baricitinib — contraindicated in pregnancy. Small molecules cross the placenta freely, and animal studies show teratogenicity. Stop at least one washout cycle (typically one week) before attempting conception.
Older DMARDs
Sulfasalazine is compatible with pregnancy (add folate). Methotrexate and leflunomide are absolute contraindications.
The 2020 EULAR Points to Consider
In 2017 (published) and updated in guidance documents through 2020, the European Alliance of Associations for Rheumatology (EULAR) Points to Consider for the Use of Antirheumatic Drugs Before Pregnancy, and During Pregnancy and Lactation (Andreoli et al) became the standard reference. The patient-facing summary:
- Active disease at conception predicts worse pregnancy outcomes than continued biologic therapy does. Controlled disease matters more than drug avoidance.
- Certolizumab, etanercept, adalimumab, and infliximab are compatible at conception and through at least the first two trimesters. Third-trimester continuation is a case-by-case call.
- Hydroxychloroquine, sulfasalazine, and azathioprine are compatible throughout pregnancy.
- Low-dose prednisone (ideally < 7.5 mg/day) is compatible for flare management.
- Methotrexate, leflunomide, mycophenolate, cyclophosphamide, and JAK inhibitors are contraindicated.
- Live vaccines should be deferred in infants whose mothers received full-transfer biologics in the third trimester.
If your rheumatologist seems uncertain, ask directly whether they are using the EULAR 2020 framework. A good answer names the framework. A vague "let’s just stop everything" answer means you need a second opinion.
Managing Flares When Most Drugs Are Off the Table
The worst stretch is often weeks 22–32: NSAIDs are gone, the third-trimester biologic dose may have been held, and mechanical load on the pelvis is peaking. What actually helps:
- Aquatic therapy. Warm-water (88–92°F) pool exercise unloads the SI joints, reduces stiffness, and is safe throughout pregnancy. Many PT clinics and YMCAs run prenatal water classes.
- Prenatal physical therapy. A PT experienced in spondyloarthritis can teach extension-based and pelvic-stabilization exercises that target AS specifically, not just generic prenatal posture. See the exercise and PT protocol.
- Heat. Heating pads and warm showers are safe on the back and hips. Avoid abdominal heat and hot tubs (core temperature concern).
- Acetaminophen (paracetamol). Safe throughout pregnancy at the standard 1 g up to four times daily. Not a strong anti-inflammatory but genuinely helpful for mechanical flare pain and mild-to-moderate stiffness.
- Short prednisone bursts. For a severe flare, a 5–7 day course of 10–20 mg prednisone is acceptable. Long-term prednisone raises gestational diabetes, hypertension, and preterm birth risk — but a short rescue course is reasonable when nothing else is working. Co-manage with your OB/MFM.
- Local corticosteroid injections. SI joint or trochanteric bursa injections with a low-dose steroid (triamcinolone) are considered acceptable when the benefit is significant.
- TENS units. Non-pharmacologic, safe, and useful for nighttime lumbar pain.
Hip, Pelvis, and Spine Mechanics
Pregnancy drops a near-perfect mechanical storm on an AS-affected spine. Relaxin loosens the symphysis and SI joints. The uterus shifts the center of gravity forward, tilting the pelvis and deepening the lumbar curve. Gait widens. Stair-climbing recruits the gluteus medius harder. In a person without AS, this is manageable; in a person with chronic SI joint inflammation, it is often the trigger for the 20-week flare.
Interventions that actually reduce mechanical load:
- Pelvic support belt (brands: Serola, Gabrialla, Baby Belly Belt). Worn low across the sacrum and pubic symphysis, these stabilize the SI joints during walking and standing. Most patients feel the difference within an hour of wearing one.
- Supportive footwear. No flats, no high heels. Structured walking shoes with arch support reduce pelvic tilt.
- Chair and car ergonomics. Lumbar roll, knees slightly lower than hips, avoid prolonged sitting over 30 minutes without standing up.
- Daily prenatal PT. Ten minutes of pelvic tilts, bird-dogs, and wall-supported standing hip extensions preserves the spinal mobility you still have.
- Avoid asymmetric loading. No carrying a toddler on one hip, no bags slung on one shoulder.
Sleep Positioning
Sleep gets harder in AS pregnancy than in almost any other situation — inflammatory stiffness and mechanical back pain stack on top of the normal third-trimester discomfort. A setup that works for many:
- Firm mattress. Soft mattresses let the pelvis sag, torquing the SI joints. If your mattress is old and soft, a firm topper helps.
- Body pillow or long wedge. Side-lying with a pillow supporting the belly keeps the lumbar spine neutral rather than rotated.
- Pillow between the knees. Keeps the pelvis level and reduces SI joint shear.
- Small rolled towel under the waist. For patients whose natural side-lying posture collapses the lumbar curve, a thin roll at the waist preserves alignment.
- Left side preferred after 20 weeks for blood flow to the placenta, though short stretches on the right are fine if SI pain forces a switch.
- Log-roll out of bed. Bend knees, roll to side, push up with arms. Never sit straight up from supine — the core crunch aggravates SI joints.
Delivery Planning
AS alone is not an indication for C-section. Vaginal delivery is the default and is generally well-tolerated even in women with fused spines, provided anesthesia planning happens in advance.
Three pieces need to be in place before labor:
- Anesthesia consultation at 28–34 weeks. Any patient with AS should meet the anesthesia team before labor, not during it. If you have spinal fusion, prior spine surgery, or significant lumbar rigidity, epidural placement may be technically difficult or impossible at the usual L3–L4 or L4–L5 interspace. Options include an epidural at a higher level, a combined spinal-epidural, ultrasound-guided placement, or — if neuraxial anesthesia is not feasible — IV or inhaled analgesia, pudendal block, or general anesthesia for C-section.
- Cervical spine mobility assessment. If you ever need general anesthesia, the anesthesiologist must intubate you. A fused or rigid cervical spine complicates intubation and may require a fiberoptic approach. Flag this explicitly.
- Labor positioning plan. Hands-and-knees, side-lying, and birth ball positions are often more tolerable than flat-on-back for AS patients. Discuss with your L&D team in advance.
If C-section is chosen for obstetric reasons, spinal anesthesia has the same technical challenges as epidural and needs the same advance planning. A good anesthesia team will have a written plan in your chart by 36 weeks.
Postpartum Flare Risk
The postpartum period is the single riskiest interval of the whole reproductive cycle for an AS patient. About 60% of women flare in the first six months after delivery, often severely. The drivers stack: pregnancy immune tolerance ends abruptly, estrogen and progesterone crash, sleep is shattered, breastfeeding adds physical load, and any biologic that was held for the third trimester has not yet been restarted.
A practical postpartum plan:
- Resume your biologic early. Certolizumab, etanercept, and adalimumab can all be restarted within days of delivery (and in many cases were never stopped). Do not wait for a flare to begin — prevent it.
- Restart daily PT/exercise as soon as cleared by your OB (typically 2–6 weeks depending on delivery). Aquatic therapy is again the easiest re-entry.
- Have a short prednisone prescription on hand for rescue use.
- Build sleep backup into the first 12 weeks. Partner night feeds, family help, pumped milk so a partner can take the 2 AM feed — sleep deprivation is both a flare trigger and a postpartum depression trigger, and the two amplify each other.
- Schedule a rheumatology visit at 4–6 weeks postpartum, not at 3 months. Catch flare-in-progress early.
Breastfeeding and Medications
Breastfeeding with AS is generally compatible with the medications that matter most:
- Certolizumab pegol — the CRADLE study measured certolizumab in breast milk across 17 mothers and found levels below the limit of quantification or at minimally detectable levels. Oral bioavailability of monoclonal antibody fragments is essentially zero (infant gut digests them). Fully compatible with breastfeeding.
- Etanercept, adalimumab, infliximab, golimumab — all transfer to milk at very low levels and are degraded in the infant gut. Compatible.
- Secukinumab, ixekizumab — limited data but expected to behave similarly. Usually considered compatible.
- Ibuprofen — very low milk transfer, short half-life. Preferred NSAID in breastfeeding. Naproxen is acceptable but has a longer half-life. Avoid aspirin (Reye syndrome risk in infant).
- Prednisone — compatible. At doses above 20 mg, some clinicians suggest waiting 4 hours after a dose before nursing, though the clinical relevance is marginal.
- Sulfasalazine — compatible in full-term healthy infants; caution in preterm or G6PD-deficient infants.
- Methotrexate, leflunomide, JAK inhibitors — not compatible with breastfeeding.
The LactMed database (free from the NIH) has evidence-based summaries for every one of these drugs and is the single best reference for any specific question.
Fertility — Yours and His
AS itself does not reduce female fertility. Time-to-pregnancy in women with controlled AS is similar to the general population. Active, uncontrolled inflammation may modestly reduce fertility and increase miscarriage risk, which is another reason to get disease activity low before trying.
For male AS patients planning a pregnancy with their partner, two drug notes:
- Sulfasalazine reduces sperm count and motility in about 60% of men who take it. The effect is fully reversible within 2–3 months of stopping. If you are a man on sulfasalazine and you and your partner are trying to conceive, discuss switching temporarily with your rheumatologist.
- Methotrexate and TNF inhibitors do not meaningfully impair male fertility based on current evidence, and men do not need to stop them before conception.
Genetic Counseling and Your Baby’s Risk
The question every AS parent asks: what is my child’s risk?
- HLA-B27 inheritance. If one parent is HLA-B27 positive (heterozygous, the usual case), each child has a 50% chance of inheriting HLA-B27. If the parent is homozygous for B27 (rare), every child inherits it.
- AS risk in the child. Inheriting HLA-B27 is not the same as developing AS. A child of an AS parent has roughly a 5–10% lifetime risk of developing AS — meaningful, but still an 85–95% chance of not developing it.
- If both parents have AS (uncommon but it happens), risk rises further — but there is no proven genetic counseling reason to avoid pregnancy on this basis alone.
- Testing children. Routine HLA-B27 testing of children of AS parents is not recommended. A positive result in an asymptomatic child changes nothing about care. Test when and if symptoms of inflammatory back pain appear.
Formal genetic counseling is reasonable if you have family history of severe AS, other HLA-B27 diseases, or if both partners carry the gene. See the HLA-B27 explained article for the full genetics.
Mental Health, Sleep Loss, and PPD
The combination of an unpredictable flare, a newborn, and shredded sleep puts AS mothers at substantially elevated risk for postpartum depression and anxiety. This is not weakness and it is not surprising — it is a predictable physiological consequence of a stressor stack, and it is treatable.
- Screen early and screen often. Ask your OB or primary care physician to do an Edinburgh Postnatal Depression Scale (EPDS) at 2, 6, and 12 weeks postpartum, not just once.
- Name the flare separately from the depression. Untreated AS pain masquerades as depression, and untreated depression worsens pain perception. Treat both.
- SSRIs are compatible with breastfeeding. Sertraline and paroxetine have the most data; both are reasonable first choices. Do not let breastfeeding be a reason to suffer untreated.
- Accept help. Meal trains, overnight doulas, partner-led feeds, grandparent shifts — any hour of uninterrupted sleep you can negotiate is a therapeutic intervention.
- Peer support. Spondylitis Association of America (SAA) and online AS pregnancy groups are full of women who have done this. You are not the first and the isolation is not mandatory.
If you are having intrusive thoughts, thoughts of self-harm, or are unable to care for your baby, call your OB, rheumatologist, or the national Maternal Mental Health Hotline (1-833-TLC-MAMA in the U.S.) immediately. This is medical, not moral.
Key Research Papers
- Andreoli L, et al. EULAR recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum Dis. 2017. (The 2020 EULAR reproductive points to consider framework.)
- Mariette X, Forger F, et al. Lack of placental transfer of certolizumab pegol during pregnancy: results from CRIB, a prospective, postmarketing, pharmacokinetic study. Ann Rheum Dis. 2018.
- Ostensen M, Husby G. Ankylosing spondylitis and pregnancy. Rheum Dis Clin North Am. 1989;15(2):241–54. (Foundational work on AS disease activity through pregnancy and postpartum.)
- FDA Drug Safety Communication, October 2020. FDA warns that use of a type of pain and fever medication in the second half of pregnancy could lead to complications. (NSAIDs and oligohydramnios; FDA.gov DSC reference.)
Live PubMed Searches
Further reading on AS, spondyloarthritis, and pregnancy. These PubMed topic searches return current peer-reviewed work:
- Ankylosing spondylitis and pregnancy
- Spondyloarthritis pregnancy outcomes
- Certolizumab pegol placental transfer
- Biologics and breastfeeding in rheumatic disease
- NSAIDs, oligohydramnios, and ductus arteriosus in pregnancy
- Postpartum flare in spondyloarthritis
- EULAR reproductive recommendations in rheumatic disease
- Epidural anesthesia in ankylosing spondylitis and spinal fusion
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- Exercise and PT Protocol
- NSAID Strategy
- Morning Stiffness Management
- Starch-Free Diet and Ebringer
- Uveitis and Eye Involvement
- Arthritis
- Lupus
- Infertility
- Preeclampsia
- Gestational Diabetes
- Depression