Morning Stiffness Management for Ankylosing Spondylitis
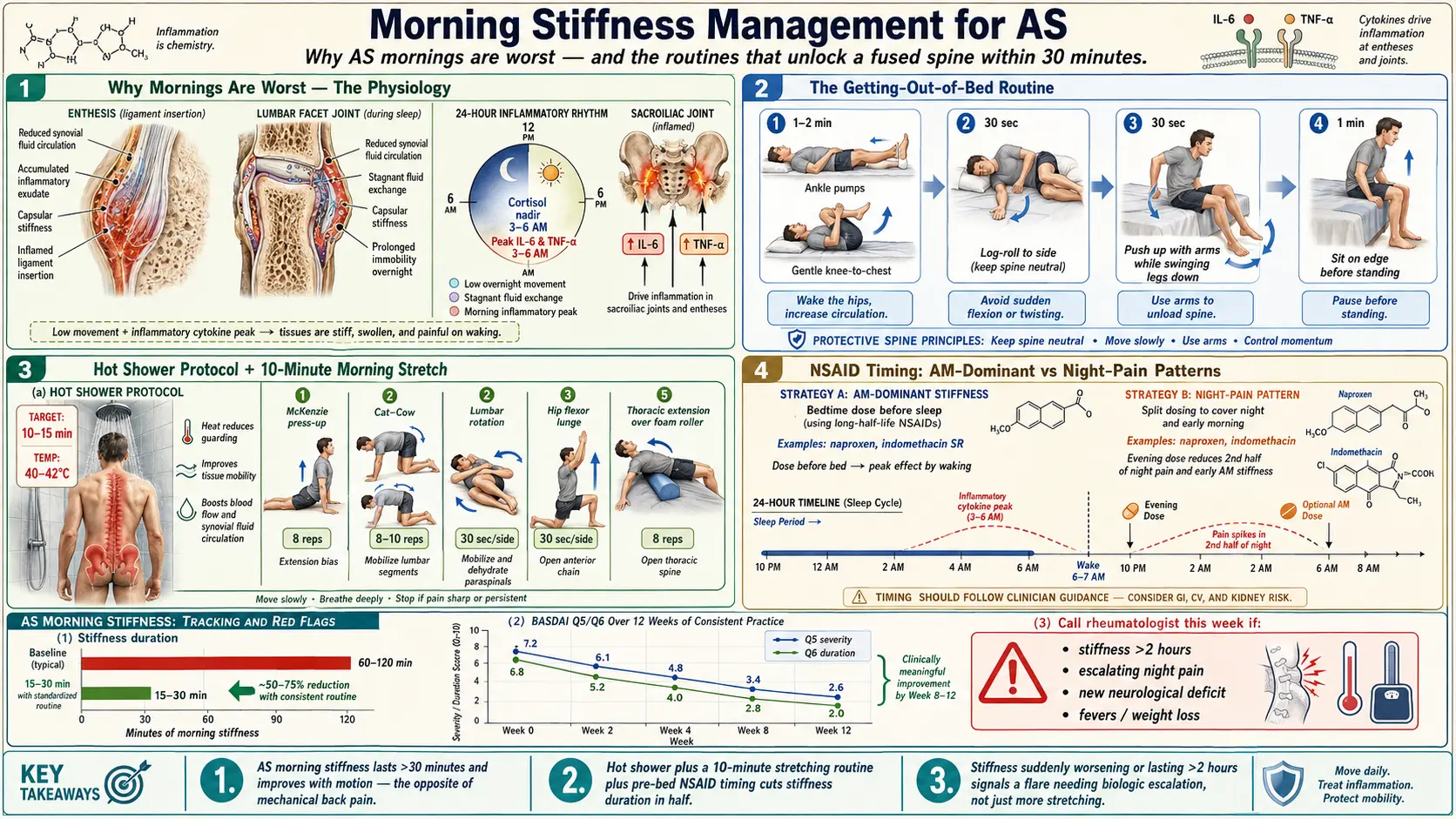
Table of Contents
- Why AS Morning Stiffness Is Different
- The Physiology — Why Mornings Are Worst
- The Getting-Out-of-Bed Routine
- The Hot Shower Protocol
- The 10-Minute Morning Stretching Sequence
- Pre-Bed Prep to Reduce AM Stiffness
- NSAID Timing — AM-Dominant vs Night-Pain Patterns
- Heat Tools That Actually Work
- Workplace Tactics
- When Stiffness Worsens — The Flare Signal
- Track Your Stiffness
- Red Flags — When to Call Someone
- Key Research Papers
- Connections
- Featured Videos
Why AS Morning Stiffness Is Different
If you have ever woken up feeling like a plank of wood — spine locked, hips jammed, ribs tight enough that a deep breath feels like work — you are not imagining it. Morning stiffness is the single most characteristic symptom of ankylosing spondylitis, and the ASAS (Assessment of SpondyloArthritis international Society) criteria use it to separate inflammatory back pain from ordinary mechanical back pain.
Four features distinguish the AS pattern:
- Duration longer than 30 minutes — typically 45 minutes to two hours on bad days. Mechanical back pain loosens within 5–15 minutes of getting up.
- Worse at rest, better with movement. Walking, stretching, and a hot shower help. This is the opposite of a disc injury.
- Second-half-of-the-night awakening. Many AS patients wake at 3–5 a.m. with pain that forces them up to move before they can fall back asleep.
- Alternating buttock pain. Deep, dull pain that switches sides from week to week — a signature of sacroiliitis.
If three or more describe your mornings and you are under 45, you are looking at inflammatory back pain until proven otherwise. Name each one to your rheumatologist. They are diagnostic gold.
The Physiology — Why Mornings Are Worst
Morning stiffness in AS is not a stretching problem. It is an inflammation problem that follows a clock. The cytokines most implicated in AS — TNF-alpha, IL-6, and IL-17 — peak between roughly 2 a.m. and 7 a.m.
While you sleep, several things stack up at once:
- Cytokine surge. TNF and IL-6 plasma levels climb overnight and peak near dawn, driving fresh inflammation in the sacroiliac joints, spinal entheses, and facet joints.
- Cortisol trough. Your own anti-inflammatory cortisol bottoms out around midnight. For a few hours you have maximum inflammation with minimum suppression.
- Immobility. Joint fluid thickens and inflammatory exudate pools when joints are still. The spine and SI joints are especially vulnerable — large, poorly vascularized, and motionless.
- Cooling. Core temperature drops during sleep, slowing synovial fluid turnover and thickening periarticular tissue.
By 6 a.m. your spine has been quietly inflamed and immobilized for hours. Every successful morning strategy does the same three things: raises tissue temperature, restores circulation, and blunts the pre-dawn cytokine peak with properly timed medication.
The Getting-Out-of-Bed Routine
The first 60 seconds out of bed matter. A bad move can set a flare in motion for the day.
Do not jackknife up from your back. Lifting your torso flat-to-upright with your abs loads the lumbar spine and SI joints at their stiffest moment — the single most common trigger for an AM pain spike.
Do the log roll instead:
- Bend both knees so feet are flat on the mattress.
- Keep shoulders and hips square — imagine you are a log.
- Slowly roll the whole log onto one side, shoulders and hips rotating together.
- Let your feet drop over the edge while pushing your torso up with your top arm.
- Arrive seated without having twisted through the spine.
Sit on the edge 30–60 seconds. Circle your ankles, shrug your shoulders, let blood return to your legs. Then stand straight up — do not hinge forward off your knees.
The pre-bed NSAID question. If you are on an NSAID and mornings are your worst time, the timing of the last dose is high-leverage. Long-acting agents (modified-release indomethacin, extended-release diclofenac, meloxicam) at dinner or bedtime can blunt the 3–6 a.m. cytokine peak. Details in the NSAID Strategy article.
The Hot Shower Protocol
A hot shower is not a luxury. It is treatment. Ten to fifteen minutes can collapse a two-hour stiffness window to 20 minutes — heat raises tissue temperature, lowers synovial fluid viscosity, dilates vessels feeding the SI joints, and damps pain signaling via gate-control effects.
- Water 40–42°C (104–108°F). Hot but not scalding.
- Ten to fifteen minutes. Under 8 minutes will not warm deep tissue; over 20 adds nothing.
- Sacroiliac joints first. The dimples above and lateral to the tailbone — where most AS starts. Turn your back to the stream for 4–5 minutes.
- Then lumbar, thoracic, and ribs. 2–3 minutes per region, tailbone to neck. Take slow deep breaths while water runs down the sides of your chest.
- Move under the water. Pelvic tilts, shoulder rolls, gentle spinal rotations. Heat plus motion beats either alone.
- Optional contrast finish. 30–60 seconds cool (not cold) at the end. Some patients find the vascular pumping leaves them less stiff two hours later; skip if you hate it.
A handheld shower head ($30) lets you aim pressure directly at the SI joints and ribs.
The 10-Minute Morning Stretching Sequence
Do this after your shower, while tissues are warm. Movements are slow and pain-guided. Repeat each 5–10 times unless noted.
- Cat-cow on hands and knees (2 min). Drop belly, lift chest and tailbone (cow); round spine, tuck chin and pelvis (cat). Mobilizes every segment through its full sagittal range.
- Supine pelvic tilts (1 min). On your back, knees bent. Flatten lower back to the floor, hold 3 seconds, release. Reactivates abdominal-pelvic coordination.
- Knee-to-chest, single then double (1 min). Hold 10 seconds each. Opens the lumbar spine and SI joints.
- Thoracic rotations (2 min). Seated with hands behind head, rotate trunk left and right, 3 seconds at end range. Or side-lying "book opener" — top arm swept across to the floor behind you. AS freezes thoracic rotation first; reclaim it daily.
- Standing hamstring stretch (1 min). Heel on a low step, hinge forward with a flat back. Tight hamstrings pull the pelvis into posterior tilt — a classic AS postural collapse.
- Wall chest stretch (1 min). Forearm on a doorframe at shoulder height, step through. Counters forward-rounded posture.
- Prone press-up (1 min). Face-down, press onto forearms (or hands), look up slightly. Holds spinal extension — the range AS attacks first.
- Diaphragmatic breathing (1 min). Hands on lower ribs. In for 4, out for 6, pushing ribs sideways into your hands. Chest expansion is lost early in AS; daily drills preserve it.
If you skip everything else in this article, do these eight movements every morning. The full exercise and PT protocol builds strength and cardio on top.
Pre-Bed Prep to Reduce AM Stiffness
Half of morning stiffness is set the night before.
- Medium-firm mattress. Too-soft sags the spine all night; too-hard creates pressure points that keep you shifting. Firmer-grade memory foam is acceptable.
- Thin pillow — or none. AS flexes the upper thoracic spine forward; a thick pillow locks that in and accelerates the "question-mark" posture. Use the thinnest pillow that keeps your head neutral.
- Side-sleep with a knee pillow. Keeps the pelvis level and takes rotational strain off the SI joints. Back sleeping is fine. Stomach sleeping is the worst — forces cervical extension and rotation all night.
- Warm shower or bath before bed. Raising core temperature 60–90 minutes before sleep helps you fall asleep faster and keeps joints warmer longer.
- Light bedding. Heavy blankets pin joints in one position.
- No alcohol after 7 p.m. Suppresses deep sleep, worsens pain perception, and irritates the stomach with NSAIDs.
- Hydrate, but not late. Dehydration thickens synovial fluid; a 2 a.m. bathroom trip interrupts the pre-dawn sleep you need most.
NSAID Timing — AM-Dominant vs Night-Pain Patterns
NSAIDs remain first-line for AS and often work dramatically. When you take them may matter as much as which one.
Morning-stiffness-dominant. You sleep reasonably well, but wake at 6–7 a.m. locked for 60–90 minutes. An evening or bedtime dose of a long-acting NSAID — modified-release indomethacin at dinner, or extended-release diclofenac at bedtime — delivers peak drug levels into the pre-dawn cytokine surge.
Night-pain-dominant. You wake at 2–4 a.m. in active pain. A split dose may be better: half with dinner, half with a protein snack at bedtime. Long-half-life agents like naproxen or meloxicam give smoother 24-hour coverage.
Sieper and colleagues showed that modified-release indomethacin at bedtime gave better morning stiffness control than standard dosing at comparable total doses. ASAS/EULAR guidelines note NSAID timing should match the patient's dominant symptom pattern.
Do not change dosing on your own. Bring a two-week pain diary and ask: "Should we move or split my NSAID to cover that window?" See the NSAID Strategy article for dose ranges, GI protection, and switching protocols.
Heat Tools That Actually Work
Heat is the cheapest and most reliably effective non-drug treatment in AS.
- Electric heating pad. The workhorse. Moist-heat option and auto-off timer. 15–20 minutes on the SI joints or lumbar spine. Moist penetrates deeper than dry.
- Heated vest or back wrap. USB-powered ($50–$120) for cold commutes, outdoor work, or chilly offices — cold stiffens AS tissue disproportionately.
- Infrared sauna. Far-infrared warms deep tissue without the suffocating air. 20–30 minutes at 45–55°C, 2–4 times weekly, reduces morning stiffness in small AS studies. Home units run $1,500–$4,000; many gyms now have them.
- Paraffin wax bath. For small hand joints, especially with psoriatic overlap. $40–$80.
- Hot water bottle. Still works. Three-quarters full, wrapped in a towel, under the lumbar spine 15 minutes.
- Adhesive heat patches (ThermaCare). 8-hour iron-oxidation patches for flights, drives, and workdays away from a heating pad.
Skip ice in the morning. Cold has a role in acute peripheral joint flares but worsens axial AS stiffness.
Workplace Tactics
Eight hours in an office chair undoes everything your shower accomplished. Prolonged static posture is the daytime equivalent of overnight immobility.
- Walk every 30 minutes. Timer. Stand, walk 60 seconds, pelvic tilts, sit back down. The single highest-impact workplace habit.
- Sit-stand desk. Alternate every 30–45 minutes. Electric desk $300–$600; countertop converter $150–$300.
- Lumbar roll or wedge cushion. Maintains the lordosis AS flattens; a wedge tilts the pelvis into neutral.
- Monitor at eye level. A laptop on a desk is a cervical-flexion trap. Top of screen at or just below eye line.
- Long flights. Aisle seat. Walk every 60 minutes. Adhesive heat patch on the SI joints. Compression socks.
- Long drives. Stop every 90 minutes. Walk 2 minutes, lean back against the car roof for a prone-press-up equivalent.
- Warm clothing. Fleece vest, under-desk space heater. Over-air-conditioned offices are an AS nightmare.
- ADA accommodations. AS is a recognized disability. You are entitled to a sit-stand desk, ergonomic seating, schedule flexibility for AM stiffness, and work-from-home on flare days. Talk to HR before you need to.
When Stiffness Worsens — The Flare Signal
Knowing your baseline lets you catch a flare early. A flare signal is one or more of these, sustained 3–5 days:
- Stiffness duration jumps from 30–60 minutes to 90–180.
- Night pain returns — waking at 2–4 a.m. multiple nights in a row.
- Peripheral joint involvement — swollen knee, inflamed Achilles, sausage finger or toe (dactylitis).
- Fatigue spikes out of proportion to workload.
- Chest expansion feels reduced; deep breaths hurt at the ribs.
- Eye symptoms — pain, redness, light sensitivity, blurred vision — same-day ophthalmology for possible uveitis.
When a flare is building:
- Do not stop stretching. Scale it back if needed — a flare is when you need movement most.
- Increase heat — second evening shower, heating pad before bed.
- Review NSAID timing and adherence. Missed doses are a common trigger.
- Prioritize sleep, hydration, anti-inflammatory eating for 1–2 weeks.
- If the flare lasts 2–3 weeks or a new peripheral joint is involved, message your rheumatologist. A flare that outlasts NSAID optimization signals escalation to a biologic may be warranted.
Track Your Stiffness
You cannot manage what you do not measure. The validated tool is the BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) — six questions scored 0–10. Question 5 covers duration of morning stiffness; Question 6 covers severity. A BASDAI of 4 or above is high disease activity and a reason to reassess treatment.
A simple daily log works:
- Wake time
- Minutes until stiffness eased
- Severity 0–10
- Night awakenings
- What you did (shower, stretches, NSAID timing, alcohol, prior-day exercise)
Two weeks of data reveals the pattern. It is the difference between "I feel stiff" and "I average 75 minutes of stiffness, waking twice a night, BASDAI 5.8." Apps: ArthritisPower, myRA, Bearable — a paper notebook is equally good.
Red Flags — When to Call Someone
Most morning stiffness is managed at home. These symptoms require the phone.
- New neurological symptoms below the waist — leg weakness, numbness, foot drop, loss of balance. A fused spine is vulnerable to cord compression from minor trauma. Urgent evaluation.
- Cauda equina warning signs — saddle anesthesia, new urinary or fecal incontinence. Emergency. Go to the ER.
- Fever plus worsening back pain. AS itself does not cause fever. Consider septic discitis, vertebral osteomyelitis, or (on biologics) opportunistic infection. Same-day call.
- Sudden severe neck pain after even minor trauma. Advanced AS creates a brittle, fused spine that can fracture from trivial impact. Image it.
- Sudden eye pain, redness, or vision change. Acute anterior uveitis can damage vision permanently in 24–48 hours. Same-day ophthalmology.
- Cardiac-feeling chest pain — crushing, radiating, with sweating or shortness of breath. AS raises cardiovascular risk. Do not assume rib inflammation.
Everything else — the plank-of-wood morning, the 90-minute unlock, the 3 a.m. shuffle — is the disease doing what it does. The routines above take the ceiling off the damage and the floor out of the misery. Do them every day. Track the results. Bring the data to your rheumatologist.
Key Research Papers
- van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017;76(6):978–991.
- Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379–1390. — Landmark review including inflammatory back pain criteria and morning stiffness definition.
- Sieper J, Lenaerts J, Wollenhaupt J, et al. Efficacy and safety of infliximab plus naproxen versus naproxen alone in patients with early, active axial spondyloarthritis. Ann Rheum Dis. 2014.
- Dougados M, Dijkmans B, Khan M, et al. Conventional treatments for ankylosing spondylitis and NSAID chronotherapy. Ann Rheum Dis. 2002;61 Suppl 3:iii40–50.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on AS morning stiffness, circadian inflammation, and management strategies:
- Ankylosing spondylitis and morning stiffness
- Inflammatory back pain criteria (ASAS)
- Modified-release NSAIDs in ankylosing spondylitis
- Circadian cytokines, TNF and IL-6 in rheumatic disease
- Exercise therapy for ankylosing spondylitis stiffness
- Hydrotherapy and heat therapy in spondyloarthritis
- BASDAI and ankylosing spondylitis disease activity
- Infrared sauna and inflammatory arthritis
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- Exercise and PT Protocol
- NSAID Strategy
- Starch-Free Diet and Ebringer
- Pregnancy and AS
- Uveitis and Eye Involvement
- Arthritis
- Crohn's Disease
- Ulcerative Colitis
- Inflammatory Bowel Disease
- Inflammatory Markers
- Vitamin D3