Uveitis & Eye Involvement in AS
Read this first if your eye is red and painful right now: do not wait. A sudden, painful, red, light-sensitive eye in someone with AS (or HLA-B27) is acute anterior uveitis until proven otherwise — and it is a true eye emergency. You need a slit-lamp exam by an ophthalmologist within 24 hours, not your primary care doctor, not an urgent care, not next week. If your regular eye clinic cannot see you today, go to an emergency department that has an on-call ophthalmologist. Every hour of delay increases the risk of permanent scarring, glaucoma, or vision loss.
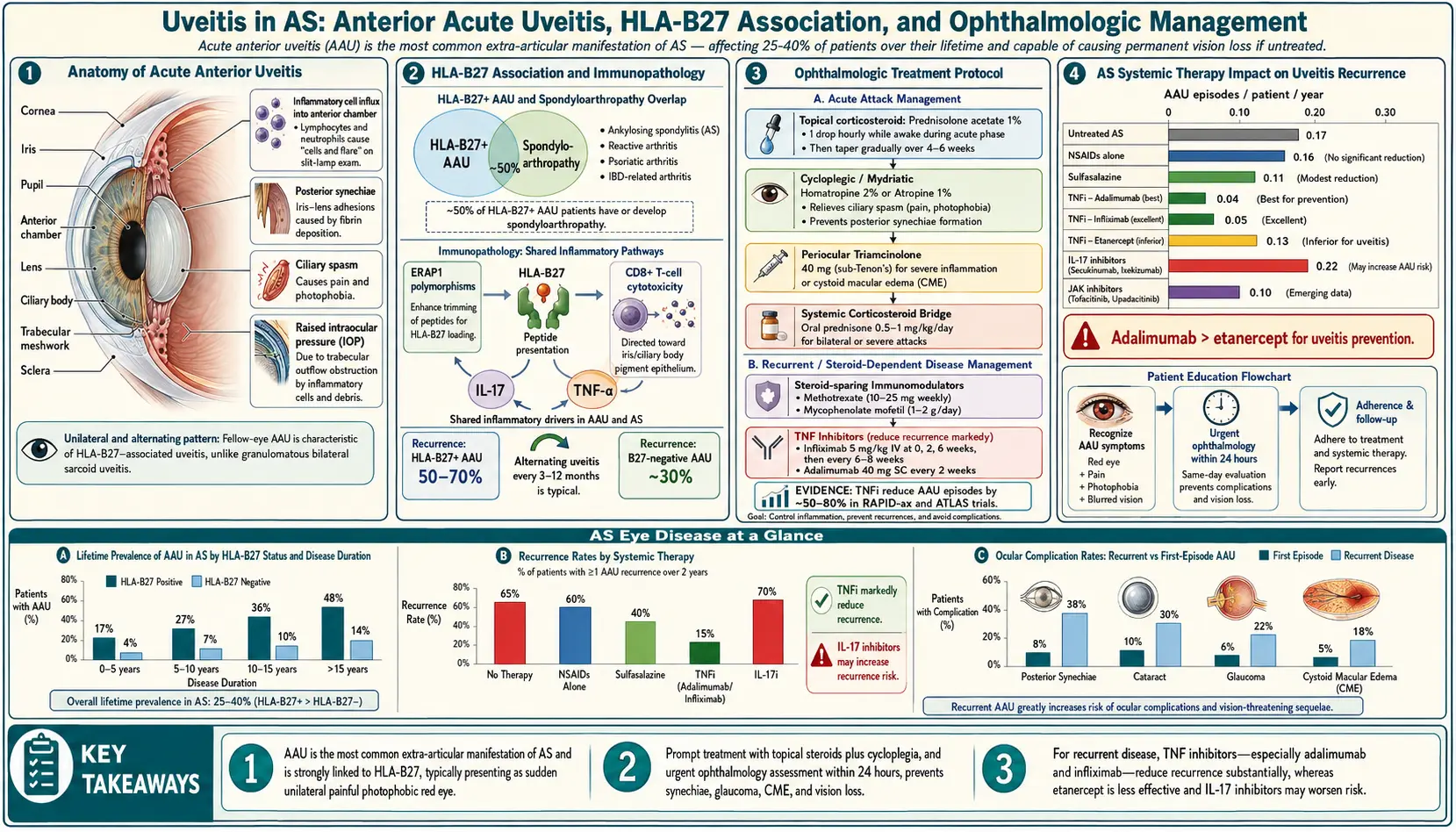
Now the background. Uveitis is the single most common non-spinal complication of ankylosing spondylitis. Roughly 25–40% of AS patients will have at least one episode in their lifetime, and for many, a uveitis flare is the first symptom — showing up years before the back pain that eventually gets the AS diagnosis. If you have a strong family history of AS or you have already tested HLA-B27 positive, understanding what uveitis looks like and what to do about it can literally save your sight.
Table of Contents
- What Uveitis Is and Which Kind AS Patients Get
- Symptoms — How to Recognize an Attack
- Why HLA-B27 Drives It
- Uveitis vs Conjunctivitis vs "Pink Eye"
- Diagnosis — The Slit-Lamp Exam
- Treatment — Drops, Dilators, and Systemic Therapy
- How AS Biologics Change Your Uveitis Risk
- Complications if Treatment Is Delayed
- Your Personal Emergency Action Plan
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
What Uveitis Is and Which Kind AS Patients Get
The uvea is the middle, pigmented layer of the eye. It has three parts: the iris (the colored ring you can see), the ciliary body (which makes the fluid inside the eye and controls the lens focusing muscle), and the choroid (a vascular layer behind the retina). "Uveitis" means inflammation of any portion of the uvea.
The type almost every AS patient gets is acute anterior uveitis (AAU) — also called iritis because the iris and the front of the ciliary body are where the inflammation concentrates. Key features:
- Acute: comes on over hours to a day or two, not weeks.
- Anterior: confined to the front chamber of the eye. The retina is usually spared, which is why prompt treatment almost always preserves vision.
- Unilateral: one eye at a time, though it often alternates between eyes across episodes. Simultaneous bilateral AAU is unusual in HLA-B27 disease and should prompt a look for other causes (sarcoidosis, Behçet, infection).
- Recurrent: once you have had one, the lifetime odds of another are high — most patients average roughly one flare every one to two years if untreated.
Posterior uveitis (inflammation of the choroid/retina) and panuveitis (whole-eye inflammation) are not typical of AS. If your ophthalmologist describes posterior or panuveitis, the workup should widen to sarcoid, tuberculosis, syphilis, Behçet's, and other causes.
Symptoms — How to Recognize an Attack
Learn these signs by heart. You may get them in any combination, and the first one often appears while you are still doing something ordinary — reading, driving into sunlight, sitting at a computer.
- Eye pain — a deep ache, not a surface scratchy feeling. Often worse when you look at something bright or when the eye tries to focus up close.
- Redness concentrated around the iris — called a ciliary flush. The redness forms a pink-to-purple ring hugging the colored part of the eye, as opposed to diffuse redness across the whole white of the eye.
- Photophobia — even normal room lighting feels painfully bright. Sunlight is unbearable. Many patients instinctively pull sunglasses on indoors.
- Blurred vision — from inflammatory cells floating in the fluid of the front chamber and from a constricted, spasming pupil.
- Floaters — specks or wisps drifting across your field of view, because white blood cells are literally suspended in the aqueous humor.
- A small, sluggish, or irregularly shaped pupil — the iris muscle is inflamed and may stick to the lens, pulling the pupil out of round.
- Tearing (without much discharge) — reflex tears from pain, not the thick goop of conjunctivitis.
If you have three or more of these in one eye, assume it is uveitis and get to an ophthalmologist the same day.
Why HLA-B27 Drives It
The link between HLA-B27 and acute anterior uveitis is as tight as the link to AS itself. Across multiple international cohorts, roughly 50–60% of people presenting with a first episode of acute anterior uveitis carry HLA-B27 — vastly higher than the 6–8% B27 prevalence in the general Caucasian population. Conversely, of people who are HLA-B27 positive, about 1% per year will have a uveitis flare, cumulative over a lifetime.
Clinically this matters because HLA-B27-associated uveitis has a signature that an experienced ophthalmologist can recognize: acute onset, unilateral, anterior only, alternating sides over years, strongly responsive to topical steroids, and often clustered in people who also have back stiffness, psoriasis, reactive arthritis, or inflammatory bowel disease. Any adult who shows up with a first episode of AAU should be asked about chronic back pain and, in most centers, offered HLA-B27 testing — because a positive result often uncovers undiagnosed spondyloarthritis. For the full genetics and mechanism, see the HLA-B27 article.
Uveitis is also more common in AS patients with concurrent inflammatory bowel disease (see AS & IBD overlap) and in those with longer disease duration.
Uveitis vs Conjunctivitis vs "Pink Eye"
Most red eyes are not uveitis. Knowing the differences lets you self-triage and lets you push back if a clinician waves you off with "looks like pink eye, use some drops."
- Viral or bacterial conjunctivitis ("pink eye") — usually bilateral (both eyes, or the second within a day or two), diffuse redness across the whole sclera, thick discharge that crusts lashes shut overnight, mild gritty irritation rather than deep pain, normal vision, normal pupil, no photophobia.
- Dry eye / corneal abrasion — scratchy surface feeling, watery, sometimes a foreign-body sensation. Pain improves dramatically with an anesthetic drop in the ER (a diagnostic clue). Pupil normal.
- Acute angle-closure glaucoma — severe pain, nausea, vomiting, hazy cornea, fixed mid-dilated pupil. Also an emergency. Distinguished by tonometry (very high eye pressure).
- Acute anterior uveitis — usually unilateral, deep aching pain, ciliary flush around the iris, photophobia, blurred vision, small or irregular pupil, minimal discharge (watery, not purulent).
The shortcut: bilateral, gooey, no real pain is almost always conjunctivitis. Unilateral, truly painful, light-sensitive, with vision changes is uveitis (or angle-closure) until an ophthalmologist says otherwise.
Diagnosis — The Slit-Lamp Exam
Uveitis is diagnosed in the clinic with a slit lamp — a microscope with a narrow beam of light that the ophthalmologist shines into the front chamber of your eye. You will be asked to rest your chin on a cushion and stare at a tiny target. The whole exam takes five to ten minutes. What they look for:
- Cells and flare. Individual inflammatory cells floating in the aqueous humor look like dust motes in a sunbeam. A hazy background ("flare") is protein leaking from inflamed blood vessels. Both are graded 0 to 4+.
- Keratic precipitates (KPs). Clumps of inflammatory cells that stick to the inner surface of the cornea. In HLA-B27 uveitis they are usually fine and scattered.
- Posterior synechiae. Adhesions where the iris has glued itself to the front of the lens. If present, the pupil will not dilate cleanly when drops are instilled — it will snag at the adhesion points and look scalloped or pulled-in.
- Hypopyon. In severe flares, a layer of white cells settles at the bottom of the front chamber, visible as a small white crescent. Uncommon but classic for HLA-B27 uveitis.
- Intraocular pressure. Measured with a tonometer. Can be low (inflamed ciliary body making less fluid) or elevated (cells clogging outflow, or steroid response later on).
- Dilated fundus exam. To confirm the back of the eye is not involved — an important step, because posterior involvement would change the diagnosis and workup.
Bloodwork and imaging are usually not needed for a first episode of classic unilateral acute anterior uveitis in someone already known to have AS. For recurrent, bilateral, posterior, or atypical uveitis, expect a broader workup: HLA-B27 if not done, chest X-ray (sarcoid, tuberculosis), syphilis serology (RPR/FTA), ACE level, QuantiFERON-TB, and occasionally brain imaging for Behçet's or multiple sclerosis.
Treatment — Drops, Dilators, and Systemic Therapy
The goals are three: stop the inflammation fast, keep the iris from sticking to the lens, and control pain. Most uncomplicated flares are handled topically.
Topical corticosteroid drops
The workhorse is prednisolone acetate 1% (brand names Pred Forte, Omnipred). A typical starting regimen for a moderate flare is one drop in the affected eye every 1 to 2 hours while awake for the first 2–3 days, then a slow taper over four to six weeks guided by repeat slit-lamp exams. Do not stop drops early just because the eye feels better — rebound inflammation is common if the taper is rushed. Alternatives include difluprednate 0.05% (stronger, BID–QID dosing) and dexamethasone 0.1%.
Warning: topical steroids can raise eye pressure and, over months, accelerate cataract. Both are manageable when the ophthalmologist is monitoring. Do not keep a leftover bottle of steroid drops in the medicine cabinet and self-treat a future flare without an exam — you can blind yourself by dosing steroids on top of a herpes simplex keratitis or a bacterial ulcer that looks like uveitis.
Cycloplegic / mydriatic drops
Drops that paralyze the iris muscle and dilate the pupil. They do three things: relieve the painful spasm of the ciliary body, pull the iris away from the lens so adhesions cannot form, and break any adhesions that have already started. Options:
- Cyclopentolate 1%, one drop 2–3 times daily — most common choice for moderate flares.
- Homatropine 5%, BID — longer-acting middle-ground.
- Atropine 1%, once daily — the strongest dilator, reserved for severe inflammation or when posterior synechiae are already forming.
Expect your vision to be blurry at near distance and your pupil to be enlarged for several days to a week after these drops. Wear sunglasses; bright light will be uncomfortable.
Stepping up — oral steroids and injections
If topical therapy is not controlling the flare after 48–72 hours, or if the inflammation is severe from the start (dense cells, hypopyon, macular involvement), the next steps are:
- Oral prednisone — typically 40–60 mg daily with a taper over weeks.
- Periocular steroid injection — triamcinolone delivered into the sub-Tenon's space or transseptally; gives weeks of high local drug levels without as much systemic exposure.
- Intravitreal steroid implants (dexamethasone, fluocinolone) — used mostly for chronic or posterior disease, rarely needed in classic HLA-B27 AAU.
Systemic immunomodulation
For patients with frequent, sight-threatening, or steroid-dependent uveitis, systemic therapy enters the picture. In AS patients this usually overlaps with the drugs already being considered for the spine — see the next section and the biologics guide.
How AS Biologics Change Your Uveitis Risk
This is one of the most important — and underappreciated — decisions in AS care: different biologics have different effects on uveitis. If you have a history of recurrent flares, your rheumatologist should choose a drug that protects your eyes, not one that ignores them or, in rare cases, provokes them.
Monoclonal anti-TNF antibodies — reduce flares
The monoclonal TNF inhibitors — infliximab (Remicade), adalimumab (Humira), certolizumab (Cimzia), golimumab (Simponi) — consistently reduce the rate of uveitis flares in spondyloarthritis, in some cohorts by more than half. Adalimumab is even FDA-approved for non-infectious uveitis on the strength of the VISUAL-1, VISUAL-2, and VISUAL-3 trials. If you have active AS and recurrent uveitis, a monoclonal anti-TNF is the default first-line biologic.
Etanercept — the notable exception
Etanercept (Enbrel), a soluble TNF receptor rather than a monoclonal antibody, does not reduce uveitis flares and in some cohorts is associated with a higher rate of uveitis episodes than other anti-TNFs. It is still effective for peripheral arthritis and for the spine itself, but if you have a significant uveitis history, it is not the biologic to choose. This distinction is so well established that "monoclonal anti-TNF, not etanercept" is essentially a guideline in AS patients with eye disease.
IL-17 inhibitors — mixed data
Secukinumab (Cosentyx) and ixekizumab (Taltz) are highly effective for the spine and for psoriasis. Their effect on uveitis is less clear. Some post-marketing reports describe paradoxical uveitis in patients starting secukinumab, though registry data suggest the overall rate is low. For AS patients whose primary problem is spinal inflammation, IL-17 inhibitors are reasonable. For AS patients whose dominant problem is recurrent uveitis, a monoclonal TNF inhibitor remains the preferred first biologic.
JAK inhibitors — emerging
Tofacitinib (Xeljanz) and upadacitinib (Rinvoq) are approved for AS and show promising signals for non-infectious uveitis, with trials ongoing. They are generally a later-line option after TNF failure, but the eye data are worth watching.
Traditional DMARDs
Methotrexate, azathioprine, and mycophenolate are used for chronic or recurrent non-infectious uveitis, particularly as steroid-sparing agents. They do not help the AS spine much but may be combined with a biologic specifically to control the eye.
Complications if Treatment Is Delayed
Most acute anterior uveitis episodes, treated promptly, resolve without lasting damage. Delay — or repeated untreated flares — invites a predictable list of complications:
- Posterior synechiae. The iris scars to the lens. Visible as a pupil that is pulled out of round or that will not dilate evenly. Small synechiae are tolerable; extensive ones can block fluid flow and precipitate secondary glaucoma.
- Cataract. Both chronic inflammation and chronic steroid exposure accelerate cataract formation, often years or decades earlier than normal age-related cataract. Modern cataract surgery is effective but more complex in an eye with a scarred iris.
- Secondary glaucoma. From inflammatory debris clogging the drainage angle, from steroid response, or from synechiae physically blocking outflow. Can cause permanent optic-nerve damage if uncontrolled.
- Cystoid macular edema. Fluid accumulating in the central retina, blurring the sharpest part of your vision. More common when inflammation is prolonged.
- Band keratopathy. A chalky calcium band across the cornea from long-standing chronic inflammation.
- Permanent vision loss. Rare with modern treatment, but real when episodes are missed, under-treated, or repeated over decades.
Your Personal Emergency Action Plan
Write this down, save it in your phone, and share it with anyone who might drive you to care.
- Know the trigger symptoms. One-sided eye pain + redness + light sensitivity + blurred vision = uveitis until proven otherwise.
- Have an ophthalmologist on file before you need one. If you have AS or are HLA-B27 positive, establish care with a uveitis-experienced ophthalmologist now, while your eyes feel fine. Ask for their after-hours number and their policy for same-day add-on appointments.
- Call, do not wait. When symptoms start, call the ophthalmology office immediately and say: "I have ankylosing spondylitis / I am HLA-B27 positive and I have a painful red light-sensitive eye. I need to be seen for possible uveitis today." Most offices will fit you in.
- If you cannot be seen in 24 hours, go to an ED with on-call ophthalmology. Call ahead to confirm ophthalmology coverage. Community ERs without eye coverage are of limited help; academic centers and larger hospitals usually have a resident available.
- Bring your medication list and your rheumatologist's contact. The ophthalmologist will want to know your current AS regimen and may want to discuss escalating systemic therapy.
- Do not self-treat with old steroid drops. Confirm the diagnosis with a slit-lamp exam first — steroids on an undiagnosed herpes or bacterial cause can blind the eye.
- Finish the taper. Once started on prednisolone drops, follow the taper schedule exactly and keep the follow-up appointments. Most rebound flares happen because drops were stopped early.
- Track flares. Keep a simple log: date, which eye, severity, treatment, recovery time. After two or three episodes, bring it to your rheumatologist — it is the single best argument for escalating to (or switching to) a monoclonal anti-TNF.
A note on contact lenses
During an active flare, stop wearing contact lenses in both eyes. The affected eye is too inflamed to tolerate a lens, and any surface trauma from a lens can confuse the diagnosis (uveitis versus contact-lens-related keratitis). Resume lenses only after the ophthalmologist confirms the inflammation is fully resolved and the drops are tapered off. Year-round, enforce standard contact lens hygiene — daily disposables where possible, never sleep in lenses, never rinse or store lenses in tap water — because a corneal infection on top of AS uveitis is a nightmare scenario.
Key Research Papers
- Rosenbaum JT. Acute anterior uveitis and spondyloarthropathies. Arch Ophthalmol. 1989.
- Rudwaleit M, et al. Adalimumab effectively reduces the rate of anterior uveitis flares in patients with active ankylosing spondylitis. Ann Rheum Dis. 2009.
- Braun J, et al. Differences in the incidence of flares or new onset of uveitis during treatment with etanercept, infliximab, and adalimumab. Arthritis Rheum. 2005.
- Jaffe GJ, et al. (VISUAL-1) Adalimumab in patients with active noninfectious uveitis. N Engl J Med. 2016.
- Ramiro S, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. 2023.
- Dick AD, Rosenbaum JT, Al-Dhibi HA, et al. Guidance on noncorticosteroid systemic immunomodulatory therapy in noninfectious uveitis: Fundamentals Of Care for UveitiS (FOCUS) initiative. Ophthalmology. 2018;125(5):757–773.
PubMed Topic Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on AS-associated uveitis biology, diagnosis, and treatment:
- HLA-B27 and acute anterior uveitis
- Ankylosing spondylitis and uveitis prevalence
- Adalimumab and uveitis in spondyloarthritis
- Etanercept and uveitis flares
- Infliximab for anterior uveitis
- Secukinumab and paradoxical uveitis
- JAK inhibitors and uveitis
- Posterior synechiae and iritis treatment
- Prednisolone acetate taper for uveitis
- Cystoid macular edema in uveitis
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- Exercise and PT Protocol
- NSAID Strategy
- Morning Stiffness Management
- Starch-Free Diet and Ebringer
- Pregnancy and AS
- Arthritis
- Lupus
- Inflammatory Bowel Disease
- Psoriasis
- Glaucoma
- Tuberculosis
- Inflammatory Markers
- Uveitis — the general overview of uveitis in all its forms, beyond the AS-associated anterior type.