Alpha-Gal Syndrome: Natural History & Path to Tolerance
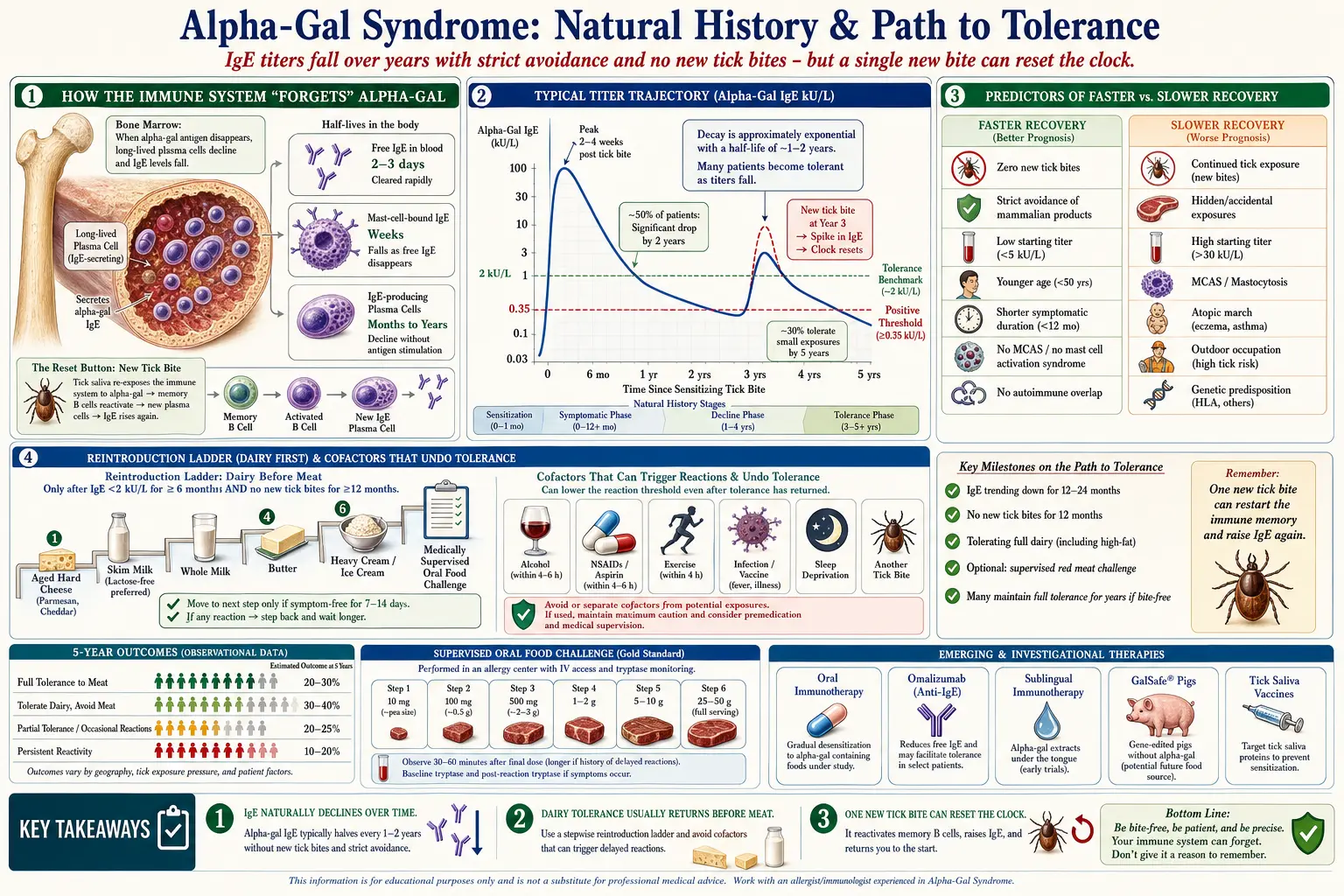
Table of Contents
- The Headline Finding
- How the Immune System "Forgets"
- Typical Titer Trajectory Over Time
- Factors Predicting Faster Recovery
- Factors Predicting Slower Recovery
- The Dairy Tolerance Evolution
- What "Recovery" Looks Like Clinically
- Can You Eat Meat Again?
- Cofactors That Undo Tolerance
- Emerging Treatments — The Research Frontier
- Why Aggressive Avoidance Is Current Best Strategy
- Partial Tolerance and Titration
- Living Well With AGS Long-Term
- Psychological Adjustment
- Children with AGS
- Honest Uncertainty
- Key Research Papers
- Research Papers (PubMed)
- Connections
- Featured Videos
1. The Headline Finding
Here is the most important thing to know if you have been newly diagnosed with Alpha-Gal Syndrome (AGS): alpha-gal IgE levels usually fall over time in patients who strictly avoid mammalian exposure and avoid new tick bites. This is not speculation — it is the consistent finding of the Platts-Mills research group at the University of Virginia, who have tracked AGS patients since the syndrome was first described.
The broad pattern looks like this:
- ~50% of AGS patients show significant titer reduction within 2 years of strict avoidance.
- ~30% of patients clinically tolerate small mammalian exposures within 5 years.
- A minority achieve near-resolution — titers falling below the detection threshold.
- Any new tick bite can reset the clock. Relapse after a fresh bite is common and often dramatic.
In other words: AGS is not necessarily a life sentence, but progress depends on two non-negotiables — avoid the antigen, and avoid the tick that put it there.
2. How the Immune System "Forgets"
IgE antibodies are produced by plasma cells that live primarily in bone marrow. When a plasma cell stops being restimulated by its target antigen, its numbers gradually decline. No new stimulus means no new clones. Over months and years, the alpha-gal-specific plasma cell pool shrinks.
The relevant half-lives:
- Free IgE in blood: 2–3 days.
- IgE bound to mast cells: weeks.
- IgE-producing plasma cells: months to years.
This is why titer decline is slow even when exposure stops completely. The machinery making the antibody takes a long time to wind down. Conversely, a single new tick bite can re-activate memory B cells and rebuild the clone in weeks — which is why prevention is everything.
3. Typical Titer Trajectory Over Time
Real-world trajectories vary widely, but the patterns look like this:
- Peak titer typically arrives 2–4 weeks after a triggering tick bite. The patient may not remember the bite.
- Without new exposures, titers roughly halve every 1–2 years on average.
- With any new tick bite or ongoing small dietary exposures, titers stay elevated or climb.
- Individual variability is enormous. Some patients crash from 30 kU/L to near-zero in 12 months; others plateau at high titers for 10+ years.
The practical recommendation is alpha-gal-specific IgE testing every 6–12 months to track personal trajectory. See Testing and Diagnosis for what to order and how to interpret results.
4. Factors Predicting Faster Recovery
Patients with these features tend to see faster titer decline and earlier clinical tolerance:
- Zero new tick bites — the single most powerful predictor.
- Strict dietary avoidance, including hidden sources (see Mammalian Foods List).
- Low starting titer (<5 kU/L at diagnosis).
- Younger age (under 50).
- Shorter duration of symptoms before diagnosis.
- No coexisting MCAS or significant atopic disease.
- No autoimmune overlap.
5. Factors Predicting Slower Recovery or Persistent AGS
On the other side:
- Continued tick bites. Every new bite resets the immune memory. This is the dominant factor.
- Chronic low-level dietary exposure — hidden mammalian ingredients not caught.
- Very high initial titer (>30 kU/L).
- Coexisting MCAS or mastocytosis.
- Atopic march — multiple existing allergies or asthma.
- Living in endemic tick regions without aggressive prevention.
- Occupational outdoor exposure — hunters, farmers, foresters, landscapers, surveyors, utility workers.
If you recognize yourself in the second list, do not despair — but do take prevention seriously. See Tick Bite Prevention.
6. The Dairy Tolerance Evolution
Many patients who initially react to dairy see dairy tolerance return before meat tolerance. This is thought to reflect the lower alpha-gal content in dairy vs. whole muscle meat and the protective effect of heat-processing and fermentation.
A typical order of dairy return over 1–3 years:
- Hard aged cheeses (parmesan, aged cheddar) — first to return.
- Skim milk and low-fat dairy.
- Whole milk.
- Butter (higher fat, more alpha-gal binding).
- Heavy cream and ice cream — often the last to return.
Meat tolerance, if it returns at all, is typically last. Every reintroduction should be medically supervised, not self-directed.
7. What "Recovery" Looks Like Clinically
There is no single definition, but allergists generally use these benchmarks:
- Titer below 2 kU/L is often associated with tolerance of small exposures without clinical reactions.
- Titer below 0.35 kU/L (the positive threshold) is achieved by roughly 20–30% of patients after 5 years of strict avoidance with no new bites.
- Low titer does not guarantee tolerance. Individual IgE affinity and co-factor sensitivity vary considerably.
- Medically supervised oral food challenge in an allergy clinic is the only way to confirm true clinical tolerance.
8. Can You Eat Meat Again?
Do not test this on your own. A supervised oral challenge in an allergist's office is the standard. The risk of unexpected anaphylaxis is real even with low titers.
Before a challenge is typically considered:
- Alpha-gal IgE titer below 2 kU/L for 6+ months.
- No reactions to accidental exposures for 6+ months.
- No new tick bites in the preceding 12 months.
- Baseline tryptase, stable vital signs, and IV access during the challenge.
A typical protocol uses gradual dose escalation of small amounts over several hours with continuous monitoring. Passing a challenge means tolerating a realistic serving without symptoms.
Even "tolerant" patients usually maintain partial avoidance: small doses may be fine, but large portions, fatty cuts (brisket, pork belly, bacon), and cofactor-heavy meals remain risky.
9. Cofactors That Undo Tolerance
Even after apparent tolerance develops, several cofactors can trigger reactions to normally-tolerated doses:
- Alcohol — amplifies gut absorption and increases reaction severity.
- NSAIDs (aspirin, ibuprofen, naproxen) — lower the reaction threshold.
- Exercise within 4 hours of eating mammalian food — a well-documented AGS cofactor.
- Acute infection or recent vaccination — general immune activation can unmask hidden reactivity.
- Sleep deprivation and acute stress — small but documented effects.
- A new tick bite — the single biggest reset button.
10. Emerging Treatments — The Research Frontier
Several experimental approaches are in various stages of study:
Oral Immunotherapy (OIT)
Systematic low-dose exposure to build tolerance, analogous to peanut OIT. Early pilot work from the Commins group at UVA shows promise. Not yet standard of care.
Omalizumab (Xolair)
Anti-IgE monoclonal antibody; FDA-approved for asthma and chronic urticaria, and recently for some food allergies. Case reports and small series show AGS symptom reduction. Cost is $2,000+ per month; coverage is an insurance battle since it is off-label for AGS.
Ligelizumab
Next-generation anti-IgE biologic in food allergy trials; potentially applicable to AGS.
Dupilumab (Dupixent)
Anti-IL-4/IL-13 biologic; investigational in atopic disease and selected food allergies.
Alpha-Gal-Depleted Meat
Revivicor developed GGTA1-knockout pigs for xenotransplantation — these lack the enzyme that builds alpha-gal. Dietary applications are theoretical but intriguing.
Avian-Derived Medical Products
Rooster-comb hyaluronic acid and other avian substitutes for mammalian-derived medical products are already safe and expanding.
Tolerance Vaccines
Long-term research on vaccines that induce tolerance to alpha-gal rather than suppressing reactions. Very early stage.
11. Why Aggressive Avoidance Is Current Best Strategy
Even with emerging treatments, strict avoidance remains the cornerstone because it:
- Gives the immune system time to forget — the plasma cell pool shrinks without restimulation.
- Prevents escalation of reaction severity.
- Lowers baseline inflammation that can worsen overlap conditions like MCAS and atopic disease.
- Allows titer tracking to guide honest decision-making about future challenges.
- Puts you in the best prognostic position if tolerance does develop.
12. Partial Tolerance and Titration
Some experienced AGS allergists gradually reintroduce small quantities of mammalian food under supervision once titers are sustained low. This is controversial and absolutely not self-directed.
Risks include unexpected reaction, sensitization reset from any new tick bite, and false confidence leading to larger accidental exposures. Only a very experienced AGS specialist should guide any reintroduction protocol.
13. Living Well With AGS Long-Term
- Identity shift. AGS is a chronic condition, not a temporary inconvenience. Expect 3–5 years minimum before seeing major titer drops.
- Dietary creativity and community. Online Alpha-Gal communities share recipes, product lists, and travel intelligence.
- Annual re-testing and careful symptom tracking.
- Emergency preparation as default — carry EpiPens and know your pre-medication protocol (see Anaphylaxis Emergency Plan).
- Address overlapping conditions. MCAS, POTS, and SIBO commonly coexist. See MCAS and SIBO.
14. Psychological Adjustment
The grief for a "normal" diet is real and under-appreciated. Social meals, travel, and family traditions often involve mammalian foods; losing that can be isolating.
- Food-related anxiety is common and can evolve into avoidant/restrictive eating.
- Therapy with a clinician familiar with chronic illness — plus an AGS-aware dietitian — helps with meal planning and nutritional adequacy.
- Community support. Alpha-Gal groups on Facebook and Reddit, plus local meetups in endemic regions, reduce isolation and speed up the learning curve.
15. Children with AGS
Pediatric AGS is less common but appears to have better long-term tolerance outcomes than adult-onset disease, though longitudinal data are limited.
- Close monitoring through adolescence for growth, nutrition, and psychosocial impact.
- 504 Plans for school meals and emergency response.
- Children may eventually outgrow AGS (as with classical pediatric food allergies), but the evidence base is thin.
16. Honest Uncertainty
AGS was only recognized in 2007–2009. That means:
- Long-term outcomes data is less than 15 years old.
- No large longitudinal studies have tracked patients for >10 years with modern assays.
- Outcomes are highly variable and no reliable individual predictor exists at diagnosis.
- Research is active. Better answers are coming in the next decade.
It is appropriate to be hopeful and also appropriate to be cautious. Both are honest responses to the current state of the science.
17. Key Research Papers
- Platts-Mills TAE, et al. α-Gal syndrome diagnosis and management. Allergy. 2020.
- Commins SP, et al. The relevance of tick bites to the production of IgE antibodies to the mammalian oligosaccharide galactose-α-1,3-galactose. J Allergy Clin Immunol. 2011.
- Kennedy JL, et al. Quality of life in α-gal syndrome. J Allergy Clin Immunol Pract. 2019.
- Pattanaik D, et al. Clinical manifestations of α-gal syndrome. Ann Allergy Asthma Immunol. 2019.
18. Research Papers (PubMed)
Additional searchable literature on PubMed:
- Alpha-gal natural history
- Alpha-gal IgE trajectory
- Alpha-gal tolerance
- Alpha-gal oral immunotherapy
- Omalizumab and alpha-gal
- Alpha-gal long-term outcomes
- Alpha-gal tick bite resensitization
- Alpha-gal biologic treatments
Connections
- Mast Cell Activation Syndrome
- Tick Bite Prevention
- Mammalian Foods List
- Anaphylaxis Emergency Plan
- Testing and Diagnosis
- SIBO
- Alpha-Gal Syndrome Overview
- Allergies
- POTS
- Tick-Origin Science
- Restaurant and Travel Survival
- Cross-Reactive Medications
- Lyme Disease
- Alpha-Gal and Cardiovascular Risk
- Elimination Diet
- Salmon
- Tick Borne Co Infections
- Hereditary Alpha Tryptasemia