Alpha-Gal Syndrome & Cardiovascular Risk
Most people with alpha-gal syndrome (AGS) think of it as a food allergy — a problem of hives, stomach cramps, and midnight anaphylaxis after a cheeseburger. But a newer line of research is asking a different and more unsettling question: does the alpha-gal antibody itself, even without food reactions, quietly damage blood vessels? A growing set of studies from the University of Virginia and other centers suggests the answer may be yes — that IgE antibodies against galactose-alpha-1,3-galactose may contribute to coronary artery plaque, especially in people with a lot of tick exposure.
This article walks you through what is known, what is suspected, and what it means practically if you have AGS and heart disease — or tick exposure and a family history of early heart attacks. This is emerging research. It is not yet part of cardiology guidelines, and it should not replace standard prevention (blood pressure, LDL control, not smoking, exercise). But it is real enough, and the implications for your care in a cath lab are concrete enough, that every AGS patient should know the basics.
Table of Contents
- Two Different Diseases in One Antibody
- The Virginia Cohort — Wilson 2018
- Follow-Up Evidence — Vernon 2022 and Beyond
- The Mechanism Hypothesis
- Sensitization Without Symptoms — the Hidden Majority
- What to Tell Your Cardiologist Before a Procedure
- Bioprosthetic Valves and Other Mammalian-Derived Devices
- The Cetuximab Story — How We Learned Any of This
- Statins, Diet, and Everyday CV Risk Management
- When to Get Tested If You Have Tick Exposure and CAD
- Key Research Papers
- Connections
- Featured Videos
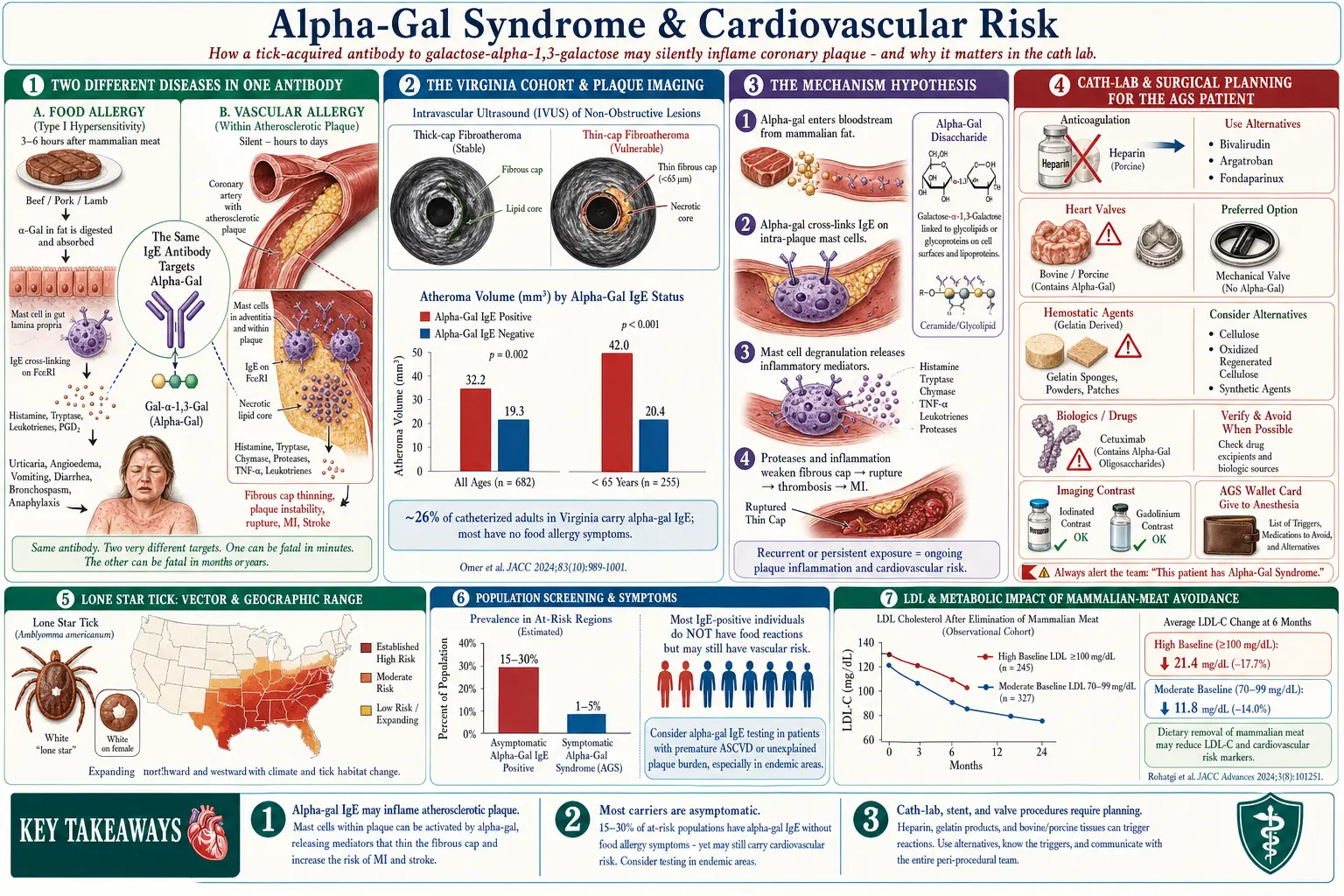
Two Different Diseases in One Antibody
The IgE antibody to alpha-gal is the same molecule whether it causes hives or silently targets blood vessels, but the clinical consequences seem to split into two lanes:
- The food-allergy lane. This is the classic AGS story — delayed (3–6 hour) reactions to beef, pork, lamb, dairy, gelatin. Mast cells in the gut and skin degranulate when alpha-gal-bearing fats from the meal hit the bloodstream. You get hives, GI symptoms, anaphylaxis.
- The vascular lane. The same IgE may also bind to mast cells that live inside the walls of coronary arteries, particularly inside developing atherosclerotic plaque. There, chronic low-grade activation — not dramatic anaphylaxis — may drive inflammation that speeds up plaque growth and instability.
The key insight is that these two lanes can be travelled independently. Some people have eye-watering food reactions and normal coronaries. Others have sky-high alpha-gal IgE, no food symptoms at all, and unusually advanced coronary disease for their age. Researchers suspect the dose of IgE, the subclass, the tick-exposure history, and individual mast-cell biology all determine which lane you end up in.
The Virginia Cohort — Wilson 2018
The study that opened this whole conversation came out of Charlottesville in 2018. Jeffrey Wilson, Thomas Platts-Mills, and colleagues at the University of Virginia looked at 118 adults undergoing cardiac catheterization and ran two tests on each one: intravascular ultrasound of the coronary arteries and blood levels of IgE to alpha-gal.
The findings that grabbed attention:
- About 26% of the cohort had detectable IgE to alpha-gal — a remarkably high figure that tracks the heavy lone-star-tick burden of central Virginia.
- Alpha-gal-sensitized patients had a higher total atheroma volume and more high-risk plaque features (necrotic core, thin fibrous cap) than matched non-sensitized patients.
- The association was strongest in patients under 65 — exactly the group in whom conventional risk factors (age, hypertension, diabetes) explain the least.
- Most of the alpha-gal-positive patients in the study did not report any food allergy. Their sensitization was silent, detected only because the researchers looked.
The study was observational, not a trial. It could not prove that alpha-gal IgE causes the extra plaque — only that the two travel together. But the correlation was strong enough, and the biology plausible enough, that Wilson's group and several others began investigating in earnest.
Follow-Up Evidence — Vernon 2022 and Beyond
Follow-up work from Vernon and colleagues in 2022 and related papers through 2024 tightened the picture:
- Alpha-gal-sensitized patients showed more evidence of active plaque inflammation on imaging, not just more total plaque.
- In mechanistic studies of human coronary plaque specimens, mast cells were found clustered near the necrotic core, the region where plaques rupture and cause heart attacks.
- Patients with high alpha-gal IgE and known coronary artery disease showed elevated markers of mast-cell activation (tryptase, chymase) in some cohorts, though results have been mixed.
- In tick-heavy regions of the southeastern U.S., early-onset coronary disease rates appear to correlate with lone-star-tick density — an ecological observation, not proof, but consistent with the hypothesis.
None of this is settled. Larger prospective studies are underway. But the signal is strong enough that a handful of cardiology centers in the tick belt now quietly check alpha-gal IgE in younger patients with unexplained coronary disease, the same way they check Lp(a) or homocysteine.
The Mechanism Hypothesis
The working theory goes like this. Atherosclerotic plaques are not just piles of cholesterol — they are chronic inflammatory lesions, and mast cells have been found inside them for decades. In a person without AGS, those mast cells are relatively quiet. In a person with circulating IgE to alpha-gal:
- Alpha-gal-bearing glycolipids enter the bloodstream from dietary meat and dairy (even in people who do not get symptomatic food reactions), or from endogenous sources that are still being worked out.
- These molecules cross-link IgE bound to mast cells inside plaques.
- The mast cells release histamine, tryptase, chymase, TNF, and proteases locally into the plaque — not enough to cause systemic symptoms, but enough to digest collagen, thin the fibrous cap, and recruit more inflammatory cells.
- Over years, this low-grade inflammation accelerates plaque growth and makes plaques more prone to rupture — the event that causes a heart attack.
This is a hypothesis, not a proven pathway. But it fits what pathologists see at autopsy, what imaging shows in vivo, and what we already know about mast cells in vascular disease from unrelated work.
Sensitization Without Symptoms — the Hidden Majority
The most important and counter-intuitive finding: most people with IgE to alpha-gal do not know they have it. They eat steak and feel fine. They have never had hives in the middle of the night. They have never seen an allergist.
In heavily tick-exposed regions, population screening studies have found alpha-gal IgE in roughly 15–30% of adults, while symptomatic AGS affects only a small fraction of that group. The ratio of silent sensitization to clinical allergy is perhaps 5:1 or 10:1.
If the vascular hypothesis is correct, this means the health impact of alpha-gal may extend far beyond the population of patients currently diagnosed with AGS. Someone in rural Virginia, Arkansas, or North Carolina with "unexplained" early coronary disease, a history of lots of outdoor work, and a few old tick bites may be carrying a relevant antibody nobody has ever tested for.
Whether to act on this possibility — to test, to modify diet, to change cardiac management — is exactly the question the research is trying to answer. For now, the honest answer is: we don't know yet, but it's worth knowing your number if you're in the risk group.
What to Tell Your Cardiologist Before a Procedure
This part is not emerging research. This part is already a real, documented problem. If you have diagnosed AGS — especially severe AGS — certain routine cardiac procedures involve medications and devices that contain mammalian material.
Heparin. Unfractionated heparin and most low-molecular-weight heparins (enoxaparin/Lovenox, dalteparin) are extracted from porcine intestinal mucosa. Any cardiac cath, stent placement, open-heart surgery, or dialysis exposes you to large doses. Anaphylactic reactions to heparin in AGS patients have been reported. Alternatives exist — bivalirudin, argatroban, fondaparinux — but they are not stocked as routinely and must be planned in advance.
Gelatin. Gelatin appears in some vaccines, in hemostatic sponges used during surgery (Gelfoam, Surgifoam), in certain vascular embolization products, and in capsule shells of many medications. For severe AGS, gelatin-based hemostatic agents are a known trigger.
IV contrast. Most modern iodinated contrast media are synthetic and do not contain alpha-gal. However, some formulations and adjuncts have historically carried mammalian-derived components. Ask specifically. Gadolinium MRI contrast is not a mammalian product and is generally fine from an alpha-gal perspective.
Other cath-lab drugs. Magnesium stearate (a tablet lubricant), stearic acid, certain IV lipid emulsions, and some anesthetic adjuvants may be mammalian-derived. Most are low-risk at the doses used, but in severe AGS, any exposure matters.
Before any cardiac procedure, hand your cardiologist and the anesthesia team a printed list of your AGS triggers and ask them to document alternatives in the chart. Bring your EpiPen. Request that the cath lab have non-mammalian anticoagulation (bivalirudin is the usual answer) available on the shelf before you are rolled in.
Bioprosthetic Valves and Other Mammalian-Derived Devices
This is one of the most discussed and still-unresolved questions in the AGS cardiology literature. Many replacement heart valves are bioprosthetic — made from bovine pericardium or porcine valve tissue. These tissues are fixed in glutaraldehyde, which cross-links the proteins and is thought to reduce but not necessarily eliminate alpha-gal antigenicity.
Case reports exist of bioprosthetic valves showing accelerated structural deterioration in AGS patients — calcifying, stiffening, or failing earlier than expected, possibly because of ongoing alpha-gal-directed immune attack on the foreign tissue. The reports are scattered, the denominator is unknown, and some AGS patients do perfectly well with bioprosthetic valves. But for someone with severe AGS who needs valve replacement, the decision is becoming:
- Mechanical valve — no mammalian tissue, lasts decades, but requires lifelong warfarin.
- Bioprosthetic valve — no warfarin, but may fail earlier in AGS and theoretically stokes ongoing immune activation.
- Synthetic or decellularized alternatives — limited availability; ask a specialty center.
This is controversial and emerging. There is no guideline recommendation either way. If you have severe AGS and face valve surgery, seek a cardiothoracic surgeon who knows the literature and is willing to discuss mechanical options seriously. The same caution applies to vascular grafts, patches, and tissue sealants that use bovine or porcine material.
The Cetuximab Story — How We Learned Any of This
The entire field of alpha-gal research started with a cancer drug. In the mid-2000s, patients in the southeastern U.S. receiving cetuximab (an anti-EGFR antibody for colon cancer and head-and-neck cancer) were having anaphylactic reactions on their first infusion — something allergists were not supposed to see, because anaphylaxis normally requires prior sensitization.
Thomas Platts-Mills' group at Virginia figured out that cetuximab is produced in a mouse cell line and carries two alpha-gal residues on its heavy chain. Patients who had been bitten by lone-star ticks in the Southeast had pre-existing IgE to alpha-gal — and cetuximab delivered the antigen directly into the vein. That was the discovery in 2008, and it was the first time anyone had connected tick bites, meat allergy, and a therapeutic antibody.
For today's AGS patients, cetuximab itself is rarely relevant unless you have the relevant cancers. The historical importance is that it is the proof-of-concept that alpha-gal IgE can drive severe reactions to IV-administered mammalian material — which is precisely why the heparin, bioprosthetic valve, and hemostatic-agent questions matter.
Statins, Diet, and Everyday CV Risk Management
Day-to-day cardiovascular risk management in AGS is mostly the same as for anyone else, with a few wrinkles:
- Statins. Statins are synthetic or fungal-derived, not mammalian. They are generally safe in AGS. The capsule or tablet inactive ingredients (magnesium stearate, lactose in some formulations) are usually fine, but patients with severe AGS have occasionally reacted to tablet fillers — ask the pharmacist for the inactive-ingredient list if you react to a new generic. There is no known interaction between statin therapy and alpha-gal biology.
- Diet. The AGS-mandated diet — no beef, pork, lamb, often no dairy — is in fact a cardiovascularly favorable diet. You are eating less saturated fat, less red and processed meat, and usually more plants, fish, and poultry. Some AGS patients see their LDL drop 20–40 points in the first year of diet compliance without any medication change. If you were considering the Mediterranean or pescatarian pattern anyway, AGS forces the issue.
- Fish, chicken, eggs. These are not mammalian and are safe both allergically and cardiovascularly. They should anchor the plate.
- Ultra-processed "safe" foods. Be careful that your AGS workaround is not pushing you toward high-sodium, high-sugar packaged foods just because they are technically mammal-free. An AGS-safe diet of chips, candy, and soda is worse for your heart than a cheeseburger.
- Blood pressure, smoking, sleep, exercise. These remain the biggest levers. None of the alpha-gal-and-atherosclerosis story changes that.
When to Get Tested If You Have Tick Exposure and CAD
No guideline currently recommends alpha-gal IgE testing as part of routine cardiac workup. But if you fit the following profile, a conversation with your cardiologist or allergist is reasonable:
- You live, or have lived, in the Southeast, Mid-Atlantic, or south-central U.S. (the lone-star-tick range).
- You have a history of multiple tick bites — even if none caused an obvious illness.
- You have coronary artery disease that is out of proportion to your conventional risk factors — early heart attack, extensive plaque on imaging, or unexplained recurrent events despite good LDL and blood pressure control.
- You have unexplained mast-cell-activation features (flushing, urticaria, GI flares after certain foods) alongside the cardiac picture.
The test is a simple blood draw: serum IgE to galactose-alpha-1,3-galactose, often ordered together with total IgE and tryptase. LabCorp and Quest both run it. Cost is typically $50–150 and insurance coverage varies — a clear clinical reason in the order helps.
What you do with a positive result is an open question. At minimum, it changes cath-lab and surgical planning (heparin alternatives, mammalian-device choices). It may justify more aggressive lipid and plaque-stabilization therapy. Whether it should change diet beyond the allergen-avoidance diet is still being studied.
The bottom line is that alpha-gal and cardiovascular disease is one of the most interesting frontiers in allergy-cardiology overlap. The evidence is not yet guideline-level. But if you are an AGS patient, you deserve a cardiologist who has at least heard of it — and if you are a heart patient in the tick belt with nothing else to explain your disease, this is one more stone worth turning over.
Key Research Papers
Foundational and recent peer-reviewed publications on alpha-gal IgE, atherosclerosis, plaque biology, and cardiovascular risk in AGS patients. Author names, titles, and journals are plain text; the year/volume/issue/pages link opens the DOI.
- Wilson JM, Nguyen AT, Schuyler AJ, Commins SP, Taylor AM, Platts-Mills TAE, McNamara CA. IgE to the Mammalian Oligosaccharide Galactose-α-1,3-Galactose Is Associated with Increased Atheroma Volume and Plaques with Unstable Characteristics. Arteriosclerosis, Thrombosis, and Vascular Biology. 2018;38(7):1665–1669.
- Vernon STJ, Kott KA, Hansen T, Finemore M, Baumgart KW, Bhindi R, Yang J, Hansen PS, Nicholls SJ, Celermajer DS, Ward MR, O'Sullivan JF, Grieve SM, Figtree GA. Immunoglobulin E Sensitization to Mammalian Oligosaccharide Galactose-α-1,3 (α-Gal) Is Associated with Noncalcified Plaque, Obstructive Coronary Artery Disease, and ST-Segment-Elevation Myocardial Infarction. Arteriosclerosis, Thrombosis, and Vascular Biology. 2022;42(3):352–361.
- Commins SP, Satinover SM, Hosen J, Mozena J, Borish L, Lewis BD, Woodfolk JA, Platts-Mills TAE. Delayed Anaphylaxis, Angioedema, or Urticaria after Consumption of Red Meat in Patients with IgE Antibodies Specific for Galactose-α-1,3-Galactose. Journal of Allergy and Clinical Immunology. 2009;123(2):426–433.
- Commins SP, James HR, Kelly LA, Pochan SL, Workman LJ, Perzanowski MS, Kocan KM, Fahy JV, Nganga LW, Ronmark E, Cooper PJ, Platts-Mills TAE. The Relevance of Tick Bites to the Production of IgE Antibodies to the Mammalian Oligosaccharide Galactose-α-1,3-Galactose. Journal of Allergy and Clinical Immunology. 2011;127(5):1286–1293.e6.
- Chung CH, Mirakhur B, Chan E, Le QT, Berlin J, Morse M, Murphy BA, Satinover SM, Hosen J, Mauro D, Slebos RJ, Zhou Q, Gold D, Hatley T, Hicklin DJ, Platts-Mills TAE. Cetuximab-Induced Anaphylaxis and IgE Specific for Galactose-α-1,3-Galactose. New England Journal of Medicine. 2008;358(11):1109–1117.
- Steinke JW, Platts-Mills TAE, Commins SP. The Alpha-Gal Story: Lessons Learned from Connecting the Dots. Journal of Allergy and Clinical Immunology. 2015;135(3):589–596.
- Wilson JM, Schuyler AJ, Workman L, Gupta M, James HR, Posthumus J, McGowan EC, Commins SP, Platts-Mills TAE. Investigation Into the α-Gal Syndrome: Characteristics of 261 Children and Adults Reporting Red Meat Allergy. Journal of Allergy and Clinical Immunology: In Practice. 2019;7(7):2348–2358.e4.
- Hilger C, Fischer J, Wölbing F, Biedermann T. Role and Mechanism of Galactose-Alpha-1,3-Galactose in the Elicitation of Delayed Anaphylactic Reactions to Red Meat. Current Allergy and Asthma Reports. 2019;19(1):3.
- Wilson JM, Erickson L, Levin M, Ailsworth SM, Commins SP, Platts-Mills TAE. Tick Bites, IgE to Galactose-α-1,3-Galactose, and Urticarial or Anaphylactic Reactions to Mammalian Meat: The Alpha-Gal Syndrome. Allergy. 2024;79(6):1440–1454.
- Platts-Mills TAE, Li RC, Keshavarz B, Smith AR, Wilson JM. Diagnosis and Management of Patients with the α-Gal Syndrome. Journal of Allergy and Clinical Immunology: In Practice. 2020;8(1):15–23.e1.
- Vaz-Rodrigues R, Mazuecos L, de la Fuente J. Current and Future Strategies for the Diagnosis and Treatment of the Alpha-Gal Syndrome (AGS). Journal of Asthma and Allergy. 2022;15:957–970.
- Carter MC, Ruiz-Esteves KN, Workman L, Lieberman P, Platts-Mills TAE, Metcalfe DD. Identification of Alpha-Gal Sensitivity in Patients with a Diagnosis of Idiopathic Anaphylaxis. Allergy. 2018;73(5):1131–1134.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- Alpha-gal and atherosclerosis
- Alpha-gal and coronary artery disease
- Alpha-gal IgE, mast cells, and coronary plaque
- Alpha-gal and heparin anaphylaxis
- Alpha-gal and bioprosthetic heart valves
- Cetuximab and alpha-gal anaphylaxis
- Asymptomatic alpha-gal sensitization in tick-exposed populations
- Alpha-gal and gelatin-containing medical products
- Lone-star tick exposure and alpha-gal epidemiology
- Mast-cell activation and cardiovascular disease
Connections
- Alpha-Gal Syndrome Overview
- Natural History and Tolerance
- Cardiovascular Disease
- Tick Bite Prevention
- Mammalian Foods List
- Tick-Origin Science
- Restaurant and Travel Survival
- Cross-Reactive Medications
- Anaphylaxis Emergency Plan
- Testing and Diagnosis
- Mast Cell Activation Syndrome
- Coronary Artery Disease
- Atherosclerosis
- Hypertension
- Homocysteine
- Asthma