Alpha-Gal Anaphylaxis Emergency Plan
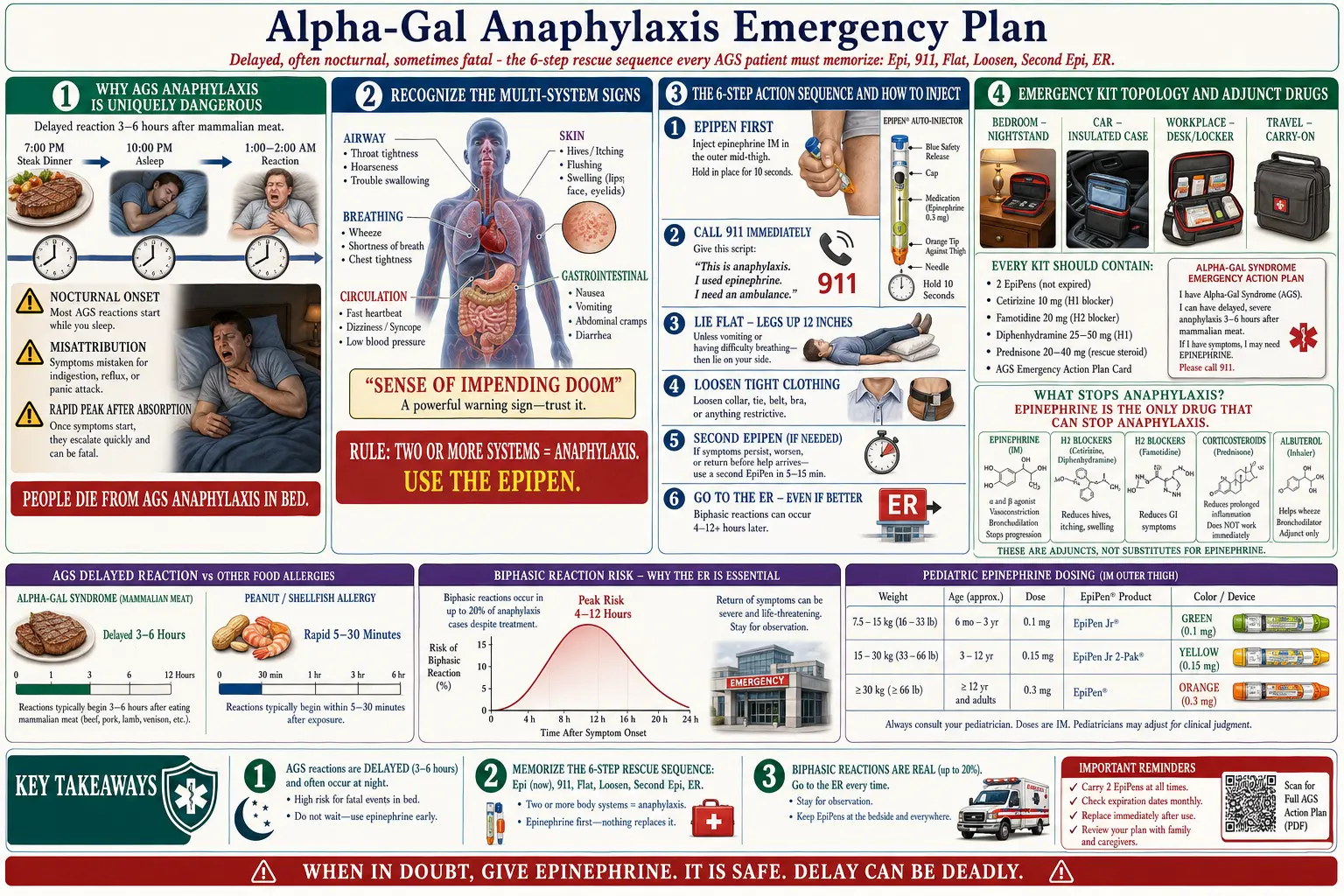
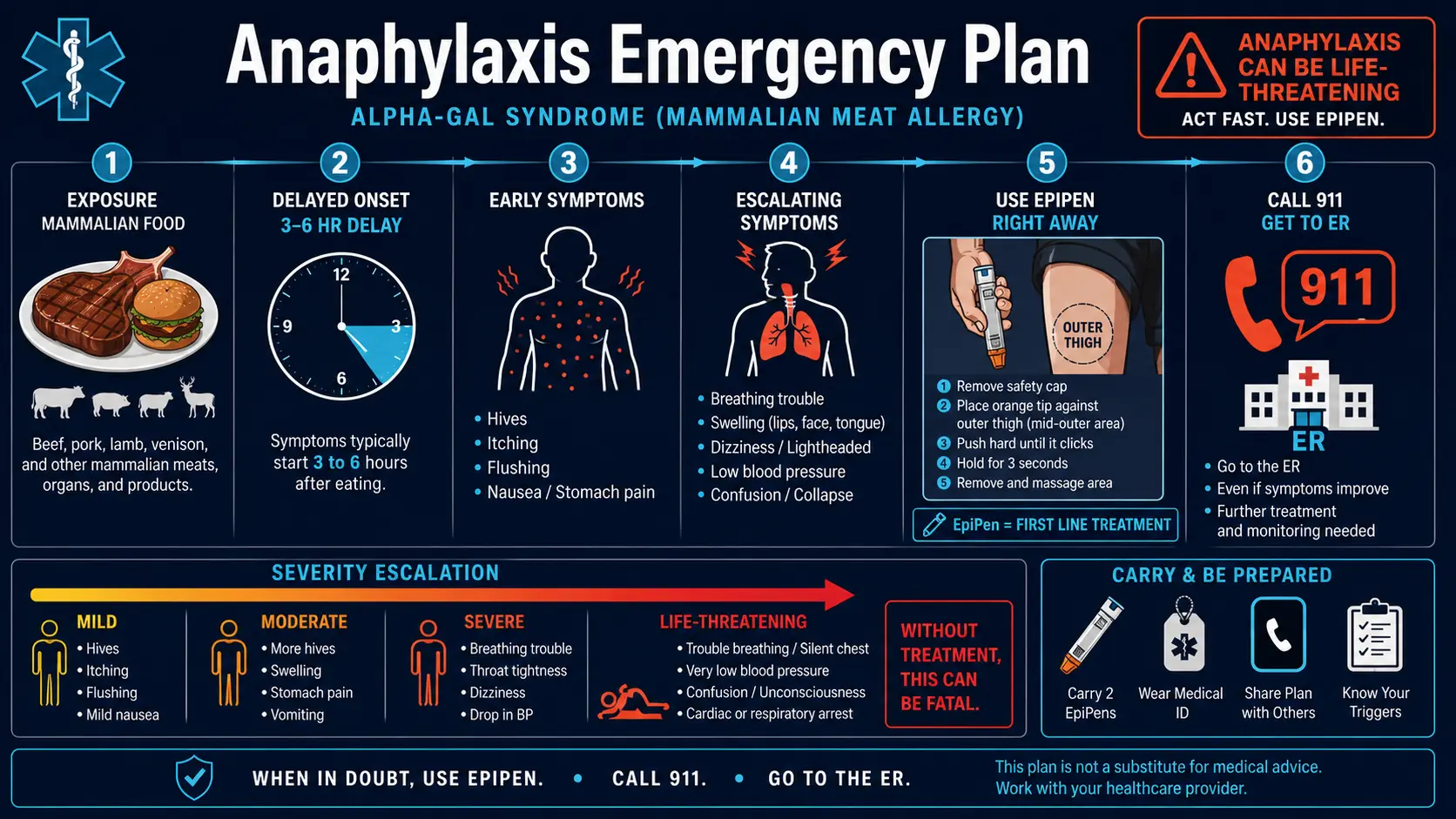
Table of Contents
- Why AGS Anaphylaxis Is Uniquely Dangerous
- Recognize the Signs of Anaphylaxis
- The Emergency Action Sequence (Memorize This)
- How to Actually Use an EpiPen
- The Other Tools Besides Epinephrine
- The Emergency Kit — What to Carry Where
- EpiPen Storage & Expiration
- Briefing Family Members, Partners, Kids
- ER Communication
- Medication Card / Wallet Template
- Biphasic Reactions — The Hidden Risk
- Triggers to Watch For Beyond Food
- After the Reaction — What to Do
- When NOT to Use an EpiPen
- Key Research Papers
- Connections
- Featured Videos
1. Why AGS Anaphylaxis Is Uniquely Dangerous
Standard food anaphylaxis — peanut, shellfish, tree nut — hits within 5 to 30 minutes of exposure. You eat, you react, you know. The allergen and the reaction are tethered in time, and that tether is what saves lives.
Alpha-Gal Syndrome breaks that tether. Because alpha-gal is a carbohydrate bound to mammalian lipids, it has to be digested, absorbed into the lymphatic system, and transported on chylomicrons before it reaches mast cells. That process takes three to six hours, sometimes longer. You eat dinner at 7 p.m. and wake at 2 a.m. covered in hives, throat tight, heart pounding, with no obvious connection to the meal.
This delay creates three specific dangers:
- Nocturnal reactions. Most AGS reactions happen in the middle of the night. People wake up already in trouble, alone in a dark room, confused and sleep-drunk. Some never wake up. People die from AGS anaphylaxis in bed.
- Misattribution. The delay makes it tempting to blame "something that didn’t agree with me." Patients dose Benadryl and go back to sleep as airway swelling progresses.
- Rapid peak. Once symptoms start, the allergen is already fully absorbed. There is no slow build. The reaction can go from hives to airway compromise in minutes.
The rule is simple and worth tattooing onto the inside of your brain: if you have AGS and you wake in the night with hives, swelling, a racing heart, or an odd sense that something is wrong — treat it as anaphylaxis until proven otherwise.
2. Recognize the Signs of Anaphylaxis
Anaphylaxis is not a single symptom. It is a multi-system reaction. The formal definition: two or more organ systems involved = anaphylaxis, full stop. Do not wait for a "worse" symptom. Two systems is the trigger.
Airway
Throat tightness, voice change (hoarse, muffled, "hot potato voice"), wheezing, stridor (high-pitched inhale), difficulty swallowing, the feeling of a lump you can’t clear.
Breathing
Shortness of breath, chest tightness, persistent cough, wheezing, inability to finish a sentence in one breath.
Circulation
Rapid heart rate, dizziness on standing, lightheadedness, fainting, pale or clammy skin, cold sweats, sudden urge to defecate or vomit (vagal response to plummeting blood pressure).
Skin
Widespread hives, severe itching (especially palms, soles, scalp, groin), lip/tongue/face swelling, generalized flushing, a feeling that your skin is "on fire."
Gastrointestinal
Severe cramping, vomiting, explosive diarrhea. In AGS, GI symptoms are often the first signal because the exposure happens through the gut.
Other — take this seriously
A sense of impending doom. Patients describe it as "something is very wrong" or "I feel like I’m about to die." This is not anxiety. It is a documented clinical sign of anaphylaxis, mediated by catecholamine release and failing circulation. If you feel it, use the EpiPen.
Two or more systems involved = anaphylaxis. Use the EpiPen.
3. The Emergency Action Sequence (Memorize This)
Print this. Tape it to the inside of your medication kit. Read it aloud with your spouse. Adrenaline shreds reading comprehension — the sequence has to be automatic.
Step 1. Use the EpiPen immediately.
Outer thigh. Hold 10 seconds. Do not hesitate. Do not "wait and see." Do not take an antihistamine first. Epinephrine goes in first, every time.
Step 2. Call 911.
Or have someone else call. Say exactly this: "Anaphylaxis. Alpha-Gal Syndrome. EpiPen given at [time]." Give the address first, symptoms second. If you are alone and your voice is failing, a text to 911 (available in most US counties) or a speakerphone call works.
Step 3. Lie flat.
Elevate the legs about 12 inches. This keeps blood in the core and protects brain perfusion while blood pressure drops. Exception: if you are vomiting, lie on your side (recovery position); if breathing is worse flat, sit upright.
Step 4. Loosen tight clothing.
Collar, belt, bra. Stay warm but not hot — a blanket, not a heating pad. Heat vasodilates and worsens hypotension.
Step 5. Second EpiPen if symptoms persist or return after 5–15 minutes.
Use the other thigh. Approximately one in five anaphylaxis patients needs a second dose. This is why your allergist prescribes two pens per kit, not one.
Step 6. Go to the ER even if you feel better.
Always. Every time. Biphasic reactions (rebound anaphylaxis) occur in up to 20% of cases, often 4–12 hours after the initial episode resolves. An ER is the only safe place to watch for them.
Epi. 911. Flat. Loosen. Second Epi. ER. Six steps. Memorize them.
4. How to Actually Use an EpiPen
Most people who own EpiPens have never used one. When the day comes, they fumble. Practice with the trainer pen every few months so your hands know the motion before your brain does.
The steps
- Remove the blue safety cap. Pull it straight off. Do not rotate, do not pry. (Blue to the sky, orange to the thigh.)
- Press the orange end firmly into the outer thigh. Mid-thigh, not hip, not groin. Through clothing is fine — jeans, leggings, pajamas. Push until you hear the click.
- Hold for 10 seconds. Not three. Not five. Ten. Count out loud. The needle retracts on removal; pulling too early leaves the dose unfinished.
- Remove and massage the injection site for about 10 seconds to aid absorption.
- Note the time. Write it on your hand if you have to. The ER will ask; paramedics will ask.
- Keep the used pen. Bring it to the ER so staff can confirm dose and lot.
Pediatric dosing
- EpiPen Jr (0.15 mg) — children 15–30 kg (roughly 33–66 lbs).
- EpiPen (0.3 mg) — anyone over 30 kg.
- A newer 0.1 mg auto-injector is available for infants 7.5–15 kg; ask your allergist.
Practice, practice, practice. Every EpiPen prescription comes with a trainer pen. Use it. Run the drill with your spouse, your teenager, your parents. If you can do it asleep, you can do it during anaphylaxis.
5. The Other Tools Besides Epinephrine
Every other medication in your emergency kit is an adjunct. None of them replaces epinephrine. None of them stops anaphylaxis. They buy time, smooth symptoms, and help prevent rebound — that is all.
- H1 antihistamine — cetirizine 10 mg or diphenhydramine 50 mg. Slows hives and itching. Does not treat anaphylaxis alone. Not a substitute for epi.
- H2 antihistamine — famotidine 40 mg. Helps GI symptoms and contributes to cardiovascular stabilization. H1 + H2 together work better than either alone.
- Oral prednisone 40–60 mg, or IV hydrocortisone / methylprednisolone in the ER. Onset takes hours; the purpose is to reduce biphasic reaction risk, not to rescue the current episode.
- Inhaled albuterol — for bronchospasm on top of epi, not instead of it.
Epinephrine is the ONLY drug that stops anaphylaxis. Everything else buys time. Burn this into memory.
6. The Emergency Kit — What to Carry Where
One kit is not enough. AGS patients need several, placed where reactions actually happen.
Bag (the one that goes everywhere)
- 2 EpiPens (never one)
- Epinephrine trainer pen
- Medication card (see template below)
- 4 x cetirizine 10 mg
- 4 x famotidine 20 mg
- Diphenhydramine 50 mg
- Prednisone 60 mg (rescue dose, prescribed by your allergist)
- Your written action plan, signed by your doctor
Bedside nightstand — critical for AGS
Because most AGS reactions happen at night, the bedside kit is arguably the most important one in the house.
- EpiPen within arm’s reach — not in a drawer, not in a closet
- Phone on the nightstand, charged
- Glass of water
- Card with "who to call" (spouse in another room, neighbor, 911)
- Medication card
Car
- EpiPens in an insulated medical case — never loose in the glove box
- Spare set for long trips
- Hot cars destroy epinephrine. Above 86°F the drug degrades rapidly. If your car has been in the sun, assume the pens are compromised and replace them.
Office / workplace
- Spare EpiPen in a labeled lockbox in the break room if your employer allows
- Written manager briefing: what AGS is, what to do, where the pen is
- At least one coworker trained on the trainer pen
7. EpiPen Storage & Expiration
- Room temperature. Ideal is 20–25°C (68–77°F). Brief excursions to 15–30°C are fine.
- Never in a hot car. Not the glove box, not the trunk in July, not on the dashboard. Use a small insulated case if the car is unavoidable.
- Do not refrigerate. Cold degrades the solution and can cause crystallization.
- Do not freeze. Once frozen, discard.
- Protect from light. Keep pens in their original tubes.
- Replace before expiration. Most pens are good for 12–18 months from dispense. Set a calendar alarm 30 days out; insurance sometimes denies early refill, so check GoodRx and manufacturer coupon programs as backup.
- Cloudy or discolored solution = discard. Clear and colorless only.
Generic and alternative auto-injectors
- Auvi-Q — a voice-guided device that talks you through the steps. Excellent for panic situations.
- Adrenaclick and the Teva generic epinephrine auto-injector — FDA-approved equivalents, often significantly cheaper.
- Mylan (Viatris) EpiPen — the brand most people picture.
All four are interchangeable clinically. Pick the one your insurance covers and the one your hands know.
Prefilled syringes of epinephrine (non-auto-injector) are not for lay use. They are a hospital workaround during shortages. Do not substitute.
8. Briefing Family Members, Partners, Kids
The person most likely to save your life is sleeping next to you. Brief them.
Spouse / partner
Must know: where the EpiPen is, how to use it, when to call 911, the six-step sequence. Practice with the trainer pen. Walk through a night-reaction scenario out loud. Do this when calm — never during a flare, never for the first time at 2 a.m. in the dark.
Kids
If old enough (generally 8+), teach them:
- Where mom or dad’s EpiPen is kept
- How to dial 911 and what to say
- "If the grown-up can’t talk, push the orange end into their outer thigh and count to ten."
This is a conversation, not a lecture. Revisit it every few months.
Babysitters, grandparents, visitors
Leave a laminated one-page instruction sheet with pictures. Have them practice with the trainer pen before you leave the house. Do not assume "a nurse in the family" knows how to use an auto-injector — different device, different muscle memory.
Schools
Children with AGS qualify for a Section 504 plan. Work with the school nurse; get authorized staff trained; keep a spare EpiPen in the health office.
Workplace
Notify HR or your manager in writing. Ask that one or two coworkers be trained on the trainer pen. If tolerated by policy, store a spare pen in a labeled break-room lockbox.
9. ER Communication
The ER sees hundreds of allergic reactions a year, but most staff have never managed an AGS reaction specifically. You will need to advocate.
At triage
Say exactly: "I have Alpha-Gal Syndrome. This is anaphylaxis. I received [X] dose(s) of epinephrine at [time(s)]." Hand over your medication card. Triage nurses move faster when the diagnosis is pre-packaged.
What to request
- Observation for at least 4–6 hours — longer if the reaction was severe or required two doses. Many ERs try to discharge at 2 hours. Push back. Biphasic risk is real.
- IV access, continuous cardiac monitoring, pulse oximetry.
- IV corticosteroids (methylprednisolone or hydrocortisone).
- IV diphenhydramine and IV famotidine.
- Repeat epinephrine if symptoms recur.
Warn the ER about cross-reactive medications
This is the part where AGS patients die of preventable exposures during treatment.
- No gelatin-containing IV fluids or volume expanders (e.g., Gelofusine).
- No heparin (bovine or porcine-sourced). Use saline flushes and, if anticoagulation is needed, fondaparinux or a direct oral anticoagulant.
- No pancreatic enzyme products of porcine origin.
- No cetuximab — use panitumumab if oncologic therapy is relevant.
- No bovine/porcine heart valves, catgut sutures, or mammalian collagen products if a procedure is needed.
See Cross-Reactive Medications for the complete list to show the ER team.
At discharge
Request a typed discharge summary listing what was given, when, at what dose, and how you responded. Your allergist will need it. Your future ER visits will need it.
10. Medication Card / Wallet Template (Print This)
Fold this into your wallet. Tape a copy inside your emergency kit. Keep one on the fridge.
ALPHA-GAL SYNDROME — EMERGENCY MEDICAL INFORMATION
I have Alpha-Gal Syndrome, an IgE-mediated allergy to galactose-alpha-1,3-galactose, a carbohydrate present in all non-primate mammalian tissue. Reactions are delayed 3–6 hours after exposure. I may present in anaphylaxis with no obvious recent food trigger.
Avoid (do not administer): beef, pork, lamb, venison, gelatin, mammalian glycerin, heparin, porcine pancreatic enzymes, gelatin-containing IV fluids, cetuximab, bovine/porcine heart valves, catgut sutures, mammalian collagen products. Dairy tolerance varies — I [do / do not] react to dairy.
Safe alternatives: fondaparinux or DOACs (anticoagulation), panitumumab (in place of cetuximab), synthetic or rooster-comb hyaluronic acid, HPMC (vegetable) capsules, polyester or synthetic sutures.
My allergist: ____________________, phone ______________
My pre-medication protocol for unavoidable exposures: cetirizine 10 mg + famotidine 40 mg 1 hour prior; prednisone 40 mg the night before and morning of, per my allergist.
In case of reaction: 2 EpiPens (outer thigh, hold 10 seconds each), 911, lie flat, ER observation 4–6 hours minimum.
11. Biphasic Reactions — The Hidden Risk
You use the EpiPen. Symptoms fade. The ER watches you for two hours. You go home, shaken but fine. Four hours later, the airway tightens again — sometimes worse than the first time.
This is a biphasic reaction: anaphylaxis symptoms that resolve with initial treatment, then return hours later without new exposure. Published rates vary from 5% to 20% of anaphylaxis cases, with the rebound most often appearing 4–12 hours after the initial resolution, occasionally up to 72 hours.
This is why the ER holds you 4–6 hours minimum. This is why you leave with a prescription for oral steroids and a fresh pair of EpiPens. This is why, after discharge:
- Sleep with EpiPens on the nightstand
- Have someone in the room, or at least within earshot, for the first 24 hours
- Have a low threshold to re-dose epinephrine at the first sign of recurrence
- Avoid alcohol, exercise, hot showers, NSAIDs, and stress for 24–48 hours (all lower your anaphylaxis threshold)
12. Triggers to Watch For Beyond Food
Alpha-gal does not act alone. Cofactors — physiological states that raise histamine release and drop the anaphylaxis threshold — routinely turn tolerable exposures into ER visits. The phenomenon is called cofactor-induced anaphylaxis or food-dependent exercise-induced anaphylaxis.
- Exercise within 4 hours before or after a meal with mammalian content.
- Alcohol with or after the meal — vasodilation accelerates reaction kinetics.
- NSAIDs (aspirin, ibuprofen, naproxen) increase gut permeability and lower the threshold.
- Hot showers, hot tubs, saunas — vasodilation again.
- Stress and sleep deprivation — well-documented threshold reducers.
- Menstruation in some women — hormonal fluctuation affects mast cell stability.
- Concurrent viral illness — the immune system is already primed.
If you must eat an uncertain meal, avoid stacking cofactors on the same day.
13. After the Reaction — What to Do
- Follow up with your allergist within one week. Sooner if the reaction was severe or required two doses.
- Journal everything. What did you eat in the 8 hours before? Any dairy? Any hidden gelatin (gummy vitamins, marshmallows, medications)? Medications taken? Exercise? Alcohol? Sleep? Menstrual cycle? Stress? The cofactor is often the missing piece.
- Refill EpiPens immediately. Used one, replace two. Never leave the kit with a single pen.
- Review your written action plan with your doctor and update it if anything went wrong.
- Retest alpha-gal IgE 4–6 weeks out. Titers often spike after a reaction; this informs how aggressive your avoidance needs to be going forward.
- Check for recent tick exposure. A new bite can re-sensitize. See Tick Bite Prevention.
14. When NOT to Use an EpiPen
Almost never.
The absolute contraindications to epinephrine are essentially none in the setting of anaphylaxis. Even patients with coronary disease, uncontrolled hypertension, or advanced age are given epinephrine when anaphylaxis is suspected — because untreated anaphylaxis is more lethal than the worst-case epinephrine side effects.
When in doubt, use it.
The worst that happens with an unnecessary dose: elevated heart rate for 20–30 minutes, a tremor in the hands, a feeling of anxiety or racing thoughts, maybe a headache. All temporary. All survivable.
The worst that happens when you hesitate on a real anaphylaxis: airway closure, cardiovascular collapse, death.
Withholding epinephrine kills more AGS patients than administering it unnecessarily ever will. If you are asking the question, the answer is use it.
15. Key Research Papers
Foundational and recent peer-reviewed publications on anaphylaxis recognition, biphasic reactions, epinephrine auto-injector use, and the unique features of alpha-gal anaphylaxis. Author names, titles, and journals are plain text; the year/volume/issue/pages link opens the DOI.
- Lieberman P, Nicklas RA, Randolph C, Oppenheimer J, Bernstein D, Bernstein J, Ellis A, Golden DBK, Greenberger P, Kemp S, Khan D, Ledford D, Lieberman J, Metcalfe D, Nowak-Wegrzyn A, Sicherer S, Wallace D, Blessing-Moore J, Lang D, Portnoy JM, Schuller D, Spector S, Tilles SA. Anaphylaxis — A Practice Parameter Update 2015. Annals of Allergy, Asthma & Immunology. 2015;115(5):341–384.
- Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, Brown SGA, Camargo CA Jr, Cydulka R, Galli SJ, Gidudu J, Gruchalla RS, Harlor AD Jr, Hepner DL, Lewis LM, Lieberman PL, Metcalfe DD, O'Connor R, Muraro A, Rudman A, Schmitt C, Scherrer D, Simons FER, Thomas S, Wood JP, Decker WW. Second Symposium on the Definition and Management of Anaphylaxis: Summary Report. Journal of Allergy and Clinical Immunology. 2006;117(2):391–397.
- Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Fernandez Rivas M, Fineman S, Geller M, Gonzalez-Estrada A, Greenberger PA, Sanchez Borges M, Senna G, Sheikh A, Tanno LK, Thong BY, Turner PJ, Worm M. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organization Journal. 2020;13(10):100472.
- Commins SP, Satinover SM, Hosen J, Mozena J, Borish L, Lewis BD, Woodfolk JA, Platts-Mills TAE. Delayed Anaphylaxis, Angioedema, or Urticaria after Consumption of Red Meat in Patients with IgE Antibodies Specific for Galactose-α-1,3-Galactose. Journal of Allergy and Clinical Immunology. 2009;123(2):426–433.
- Pattanaik D, Lieberman P, Lieberman J, Pongdee T, Keene AT. The Changing Face of Anaphylaxis in Adults and Adolescents. Annals of Allergy, Asthma & Immunology. 2018;121(5):594–597.
- Stone CA Jr, Commins SP, Choudhary S, Vethody C, Heavrin JL, Wingerter J, Hemler JA, Babe K, Phillips EJ, Norton AE. Anaphylaxis after Vaccination in a Pediatric Patient: Further Implicating Alpha-Gal Allergy. Journal of Allergy and Clinical Immunology: In Practice. 2019;7(1):322–324.e2.
- Lee S, Bellolio MF, Hess EP, Erwin P, Murad MH, Campbell RL. Time of Onset and Predictors of Biphasic Anaphylactic Reactions: A Systematic Review and Meta-Analysis. Journal of Allergy and Clinical Immunology: In Practice. 2015;3(3):408–416.e1–2.
- Simons FER, Ardusso LRF, Bilò MB, El-Gamal YM, Ledford DK, Ring J, Sánchez-Borges M, Senna GE, Sheikh A, Thong BY. World Allergy Organization Anaphylaxis Guidelines: Summary. Journal of Allergy and Clinical Immunology. 2011;127(3):587–593.e22.
- Platts-Mills TAE, Li RC, Keshavarz B, Smith AR, Wilson JM. Diagnosis and Management of Patients with the α-Gal Syndrome. Journal of Allergy and Clinical Immunology: In Practice. 2020;8(1):15–23.e1.
- Wilson JM, Schuyler AJ, Workman L, Gupta M, James HR, Posthumus J, McGowan EC, Commins SP, Platts-Mills TAE. Investigation Into the α-Gal Syndrome: Characteristics of 261 Children and Adults Reporting Red Meat Allergy. Journal of Allergy and Clinical Immunology: In Practice. 2019;7(7):2348–2358.e4.
- Hilger C, Fischer J, Wölbing F, Biedermann T. Role and Mechanism of Galactose-Alpha-1,3-Galactose in the Elicitation of Delayed Anaphylactic Reactions to Red Meat. Current Allergy and Asthma Reports. 2019;19(1):3.
- Wilson JM, Erickson L, Levin M, Ailsworth SM, Commins SP, Platts-Mills TAE. Tick Bites, IgE to Galactose-α-1,3-Galactose, and Urticarial or Anaphylactic Reactions to Mammalian Meat: The Alpha-Gal Syndrome. Allergy. 2024;79(6):1440–1454.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- Alpha-gal delayed anaphylaxis
- Biphasic anaphylaxis
- Epinephrine auto-injector use
- Food-dependent exercise-induced anaphylaxis
- Alpha-gal cofactor reactions
- Alpha-gal nocturnal reactions
- Alpha-gal emergency management
- Anaphylaxis observation time in ER
Connections
- Tick Bite Prevention
- Cross-Reactive Medications
- Natural History and Tolerance
- Alpha-Gal Syndrome Overview
- Allergies
- Mammalian Foods List
- Tick-Origin Science
- Restaurant and Travel Survival
- Testing and Diagnosis
- Mast Cell Activation Syndrome
- POTS
- Food Intolerance
- Asthma
- Alpha-Gal and Cardiovascular Risk
- Lyme Disease
- Hives and Flushing
- Anaphylaxis — the general condition, its diagnostic criteria, and standard emergency treatment.