Cross-Reactive Medications in Alpha-Gal Syndrome
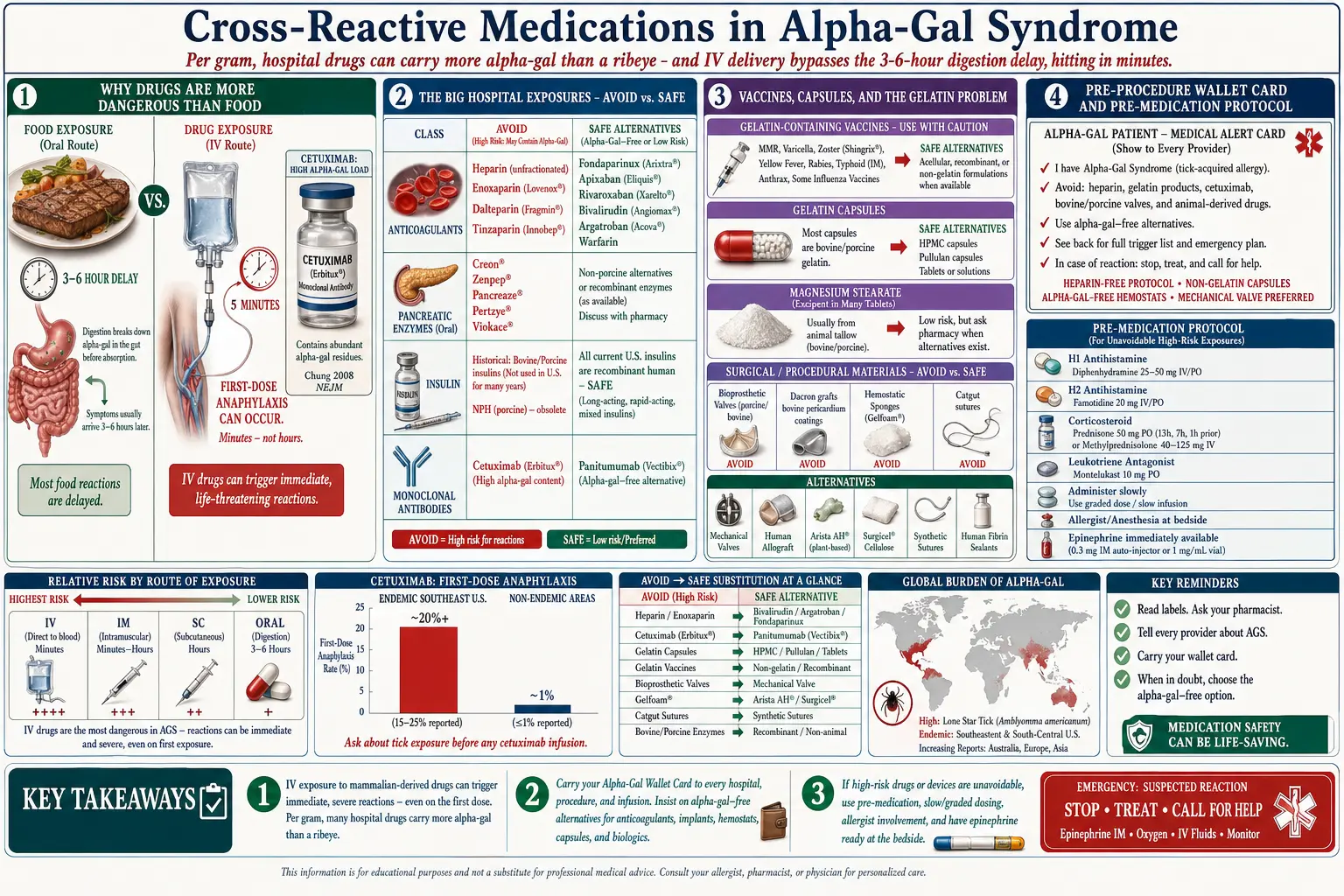
Table of Contents
- Why This Matters More Than You’d Expect
- Cetuximab (Erbitux)
- Heparin and Related Anticoagulants
- Porcine Pancreatic Enzymes
- Insulin — Historical and Current
- Vaccines Containing Gelatin
- Capsule Shells
- Magnesium Stearate — The Debate
- Surgical & Procedural Exposures
- Anesthesia Considerations
- Radiocontrast Dyes
- Dental & Wound Care
- Everyday Supplements & OTC
- The Pre-Procedure Wallet Card / Action Letter
- Pre-Medication Protocols for Unavoidable Exposures
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why This Matters More Than You’d Expect
Most Alpha-Gal Syndrome (AGS) patients focus hard on food labels and restaurant menus, and then get blindsided in a hospital. Medications and medical products can contain far more alpha-gal per gram than a ribeye steak, and many are delivered intravenously or by injection — bypassing the stomach entirely.
That matters because digestion is what slows food-borne alpha-gal reactions down. Eat beef and you react 3–6 hours later. Infuse a mammalian-derived drug and you can be in anaphylaxis within minutes, often during the first dose.
Your primary care doctor, your pharmacist, and the anesthesia team prepping you for surgery may have never heard of alpha-gal. You are the last line of defense. This page is the checklist.
2. Cetuximab (Erbitux)
Cetuximab is the monoclonal antibody that accidentally discovered alpha-gal. In 2008, Chung and colleagues at the University of Virginia published the landmark paper in the New England Journal of Medicine showing that patients in the Southeastern US were suffering first-dose anaphylaxis to cetuximab — and that their pre-existing IgE targeted a sugar on the drug, not the protein.
Why cetuximab is so dangerous in AGS
- Used for metastatic colorectal cancer and head/neck squamous cell carcinoma
- Produced in mouse myeloma (SP2/0) cells, which heavily glycosylate the Fab region with galactose-α-1,3-galactose
- First-dose IV exposure with no pre-existing tolerance
- Anaphylaxis rates of 20%+ in tick-endemic regions before screening became standard
Alternative
Panitumumab (Vectibix) is a fully human monoclonal antibody produced in a human-derived cell line and does not carry alpha-gal. For EGFR-targeted therapy in an AGS patient, panitumumab is the drug of choice.
3. Heparin and Related Anticoagulants
Heparin is the single most common intraoperative exposure. It is extracted from porcine intestinal mucosa (pork) and, historically, bovine lung. It is glycosaminoglycan-rich and can carry alpha-gal contamination.
AVOID
- Unfractionated heparin (UFH) — porcine
- Enoxaparin (Lovenox) — porcine low-molecular-weight heparin
- Dalteparin (Fragmin) — porcine
- Tinzaparin (Innohep) — porcine
SAFE alternatives
- Fondaparinux (Arixtra) — fully synthetic pentasaccharide, alpha-gal-free
- Apixaban (Eliquis) — synthetic DOAC, SAFE
- Rivaroxaban (Xarelto) — synthetic DOAC, SAFE
- Dabigatran (Pradaxa) — synthetic DOAC, SAFE
- Edoxaban (Savaysa) — synthetic DOAC, SAFE
- Warfarin (Coumadin) — synthetic coumarin, SAFE
- Bivalirudin, argatroban — synthetic direct thrombin inhibitors, SAFE
Before any major procedure, tell the anesthesia and surgical team in writing that you require a heparin-free protocol. Many cardiac catheterization labs and orthopedic units use bivalirudin or fondaparinux as a default substitute when heparin is contraindicated.
4. Porcine Pancreatic Enzymes
Pancreatic enzyme replacement therapy (PERT) for chronic pancreatitis, cystic fibrosis, or post-Whipple pancreatic insufficiency is almost universally porcine-derived.
AVOID (porcine)
- Creon
- Zenpep
- Pancreaze
- Pertzye
- Viokace
There is no widely available non-mammalian PERT product on the US market. Some AGS patients tolerate these enzymes because the enteric coating delivers them past the stomach and they are largely destroyed by gut proteases before systemic exposure — but others react strongly. The decision is individual and should involve an allergist, a GI specialist, and a pre-medication protocol on the first attempt.
5. Insulin — Historical and Current
Historical: Before the 1980s, insulin was extracted from bovine and porcine pancreas. Those products are no longer used in developed markets.
Current insulins are SAFE. All modern human insulin (Humulin, Novolin) and insulin analogs — lispro (Humalog), aspart (NovoLog), glargine (Lantus, Basaglar), detemir (Levemir), degludec (Tresiba) — are recombinant products made in yeast or E. coli. No mammalian cells, no alpha-gal.
6. Vaccines Containing Gelatin
Porcine gelatin is a common vaccine stabilizer, especially in live attenuated products. A single MMR dose contains roughly 15 mg of porcine gelatin — enough to trigger reactions in sensitized AGS patients.
Gelatin-containing (use caution or pre-medicate)
- MMR (M-M-R II) — porcine gelatin
- Varicella (Varivax) — porcine gelatin
- Zostavax (discontinued in US) — porcine gelatin
- FluMist nasal influenza — porcine gelatin
- YF-VAX (yellow fever) — porcine gelatin
- Japanese encephalitis (JE-VAX, historical)
- Tick-borne encephalitis (European formulations)
SAFE alternatives
- Shingrix for zoster — recombinant, no gelatin, SAFE
- Injectable flu shots — Fluzone, Fluarix, Afluria, Flucelvax formulations without gelatin; confirm with the pharmacist at time of dispensing
- mRNA platforms — no gelatin
- Most Tdap, hepatitis A, hepatitis B, HPV, pneumococcal, meningococcal vaccines — gelatin-free
If an AGS patient needs a gelatin-containing vaccine (pregnancy planning and MMR, travel and yellow fever), pre-medication plus a graded-dose protocol in an allergist’s office with epinephrine on hand makes it possible for most patients.
7. Capsule Shells
Most hard-shell and soft-gel capsules are made of porcine or bovine gelatin. The active drug inside may be completely synthetic, but the shell alone can provoke reactions.
SAFE alternatives
- HPMC (hypromellose) capsules — plant-derived, vegan/vegetarian, alpha-gal-free
- Pullulan capsules — fermented tapioca, SAFE
- Tablets — usually no gelatin coating; confirm
- Oral solutions, suspensions, powders — no capsule at all
Compounding pharmacies can re-encapsulate almost any drug in HPMC shells for a modest fee. Ask your prescriber for a note reading “dispense in non-gelatin capsule” — most insurance will still cover it.
8. Magnesium Stearate — The Debate
Magnesium stearate is the most common tablet-flow agent in the industry. The stearic acid can come from vegetable sources (palm, soy, coconut) or from beef tallow. The label almost never says which.
Here is the honest answer: most AGS patients tolerate magnesium stearate regardless of source. The amounts are milligram-scale, the molecule is a fatty acid salt (not intact protein or intact glycolipid), and the processing denatures most of the alpha-gal structure.
If you are a high-titer, highly reactive patient on a daily maintenance medication, call the manufacturer and ask for a source-of-stearate letter. Many will provide one on request. Bulk-compounded or branded products like Jarrow and Pure Encapsulations often label “vegetable stearate” explicitly.
9. Surgical & Procedural Exposures
Surgery is where AGS gets dangerous fast. Flag every product below to your surgeon and anesthesiologist in writing, ideally two weeks before the operation.
AVOID
- Bovine or porcine bioprosthetic heart valves (Edwards Magna, Medtronic Hancock, Mosaic). Alternative: mechanical valve (St. Jude, On-X) or a valve-in-valve procedure using decellularized tissue.
- Porcine skin grafts in burn care. Alternative: human cadaveric allograft or synthetic (Integra, Biobrane).
- Bovine bone grafts (Bio-Oss, orthopedic demineralized bone matrix). Alternative: synthetic beta-TCP, hydroxyapatite, or autograft.
- Bovine-derived hyaluronic acid joint injections (Hyalgan, Synvisc historical bovine). Alternative: rooster-comb-derived (avian) HA — SAFE in AGS — or synthetic HA products.
- Bovine or porcine collagen injections (cosmetic fillers, wound care collagen). AVOID.
- Hemostatic agents: Floseal (bovine gelatin + bovine thrombin), Surgiflo (porcine gelatin), Gelfoam (porcine gelatin), Surgicel Fibrillar (bovine thrombin-soaked). AVOID.
- Catgut sutures — sheep or bovine submucosa. AVOID.
SAFE alternatives
- Tisseel, Evicel — human-derived fibrin sealants (confirm formulation; most are safe)
- Surgicel Original — oxidized regenerated cellulose, no mammalian, SAFE
- Arista AH — plant-derived microporous polysaccharide hemostat, SAFE
- Polyglycolic acid (Vicryl), polypropylene (Prolene), nylon, silk sutures — SAFE
10. Anesthesia Considerations
Most anesthesia drugs are fully synthetic and SAFE. The risks are in the adjuncts.
SAFE
- Succinylcholine — synthetic
- Rocuronium, vecuronium, cisatracurium — synthetic neuromuscular blockers
- Propofol — soybean oil + egg lecithin emulsion, no mammalian content
- Fentanyl, morphine, hydromorphone, remifentanil, sufentanil — synthetic opioids
- Lidocaine, bupivacaine, ropivacaine — synthetic local anesthetics
- Sevoflurane, isoflurane, desflurane — synthetic inhaled agents
WATCH OUT FOR
- Heparin flushes in IV lines — request saline-only flushes
- Gelatin-based volume expanders (Gelofusine, Haemaccel in Europe) — request crystalloid (Lactated Ringer’s, normal saline) or albumin
- Sugammadex — synthetic cyclodextrin, SAFE, and ironically a rescue option when rocuronium needs reversal
11. Radiocontrast Dyes
Most iodinated contrast agents (iohexol, iopamidol, iodixanol) used in CT and angiography are fully synthetic iodine-based molecules and are SAFE for alpha-gal.
Gadolinium-based contrast for MRI is also synthetic and generally SAFE, although carrier molecules and preservatives should be reviewed for sensitive patients.
Do not confuse classical radiocontrast hypersensitivity (a non-IgE pseudoallergy with its own pre-medication protocol) with alpha-gal reactivity — they are different mechanisms and require different workups.
12. Dental & Wound Care
Dentists almost never think about alpha-gal. Bring the wallet card.
- Gelatin hemostatic sponges (Gelfoam) after extractions — AVOID. Request oxidized cellulose (Surgicel Original) or tranexamic acid rinse.
- Bovine collagen gum grafts in periodontal surgery — request connective tissue autograft or acellular dermal matrix from a non-mammalian source.
- Catgut sutures — AVOID. Request silk, nylon, or Vicryl.
- Local anesthetics (lidocaine with epinephrine) — SAFE.
13. Everyday Supplements & OTC
The supplement aisle is a minefield. Assume mammalian unless the label says otherwise.
- Glucosamine — often shellfish-derived (SAFE) but sometimes bovine cartilage. Check label.
- Chondroitin — almost always bovine trachea or porcine. AVOID unless explicitly labeled shark or marine.
- Collagen powders, peptides — almost always bovine or porcine. AVOID. Marine collagen from fish skin is SAFE.
- Fish oil softgels — the fish oil itself is fine, but the softgel shell is usually bovine gelatin. Switch to liquid fish oil or HPMC-encapsulated fish oil (Nordic Naturals and Carlson offer these).
- CoQ10, vitamin D, vitamin E, vitamin K softgels — same softgel issue. Liquid drops or HPMC versions are SAFE.
- Lanolin-sourced vitamin D3 — technically sheep-derived. Most AGS patients tolerate it (highly processed, low alpha-gal content), but vegan D3 from lichen is an alternative.
- Bovine desiccated thyroid (Armour, NP Thyroid) — AVOID. Use levothyroxine (Synthroid, generic) — synthetic, SAFE.
14. The Pre-Procedure Wallet Card / Action Letter
Print this. Laminate it. Carry it in your wallet and give a copy to every doctor, dentist, and surgeon you see.
I have Alpha-Gal Syndrome — an IgE-mediated allergy to galactose-α-1,3-galactose, a carbohydrate present in all non-primate mammals.
I must avoid: heparin and low-molecular-weight heparins (use fondaparinux or a DOAC); porcine pancreatic enzymes; bovine and porcine gelatin (hemostatic agents, vaccine stabilizers, capsule shells); bovine and porcine heart valves; bovine-derived hyaluronic acid; catgut sutures; gelatin-containing IV volume expanders; collagen injections and grafts.
Safe alternatives exist for every item above.
Pre-medication protocol (per my allergist): prednisone 40–60 mg at 13, 7, and 1 hour before procedure; cetirizine 10 mg and famotidine 20 mg one hour before; IV diphenhydramine 50 mg and hydrocortisone 100 mg available; epinephrine auto-injector at bedside.
My allergist: [name, phone]. In anaphylaxis: 0.3 mg IM epinephrine, call 911, transport.
Pre-printed cards are available from Alpha-Gal Information (alphagalinformation.org) and the Virginia Tech Center for Food Animal Health.
15. Pre-Medication Protocols for Unavoidable Exposures
When an AGS patient absolutely needs a mammalian-derived product (a heparin-free surgical plan impossible; a gelatin-containing vaccine mandatory for travel), the standard allergy-desensitization framework applies.
Standard pre-medication
- Prednisone 40–60 mg orally at 13, 7, and 1 hour before exposure
- Cetirizine 10–20 mg (H1 antihistamine) 1 hour before
- Famotidine 20–40 mg (H2 antihistamine) 1 hour before
- Montelukast 10 mg evening before (optional; blocks leukotriene pathway)
Procedure-day setup
- IV access secured before exposure
- Injectable diphenhydramine 50 mg and hydrocortisone 100 mg drawn up and ready
- Epinephrine 1:1000 (0.3 mg IM dose) at bedside, not in a cabinet
- Continuous pulse oximetry and blood pressure monitoring
- Slow initial infusion rate — 1/10 of normal rate for the first 30 minutes, titrate up if tolerated
- Observation for at least 2 hours after completion
This is the same framework used for cetuximab desensitization and taxane hypersensitivity. It works for the majority of unavoidable AGS exposures.
16. Key Research Papers
- Chung CH, et al. Cetuximab-induced anaphylaxis and IgE specific for galactose-α-1,3-galactose. N Engl J Med. 2008.
- Dunkman WJ, et al. Perioperative anaphylaxis to gelatin in a patient with alpha-gal syndrome. J Allergy Clin Immunol. 2017.
- Platts-Mills TAE, et al. Diagnosis and management of patients with the α-Gal syndrome. Allergy. 2020.
- Stone CA, et al. Anaphylaxis after zoster vaccine and other drugs in patients with the alpha-gal syndrome. J Allergy Clin Immunol Pract. 2020.
17. Research Papers
Open literature searches on PubMed:
- alpha-gal + heparin
- alpha-gal + vaccine gelatin
- alpha-gal + perioperative
- cetuximab + anaphylaxis
- alpha-gal + bovine heart valve
- alpha-gal + magnesium stearate
- alpha-gal + pancreatic enzyme
- alpha-gal + drug reaction
Connections
- Natural History and Tolerance
- Alpha-Gal Syndrome Overview
- Tick Bite Prevention
- Mammalian Foods List
- Tick-Origin Science
- Restaurant and Travel Survival
- Anaphylaxis Emergency Plan
- Testing and Diagnosis
- Mast Cell Activation Syndrome
- Lyme Disease
- Allergies
- Alpha-Gal and Cardiovascular Risk
- Collagen
- Magnesium
- Food Intolerance
- Salmon