Alpha-Gal Syndrome Testing & Diagnosis Guide
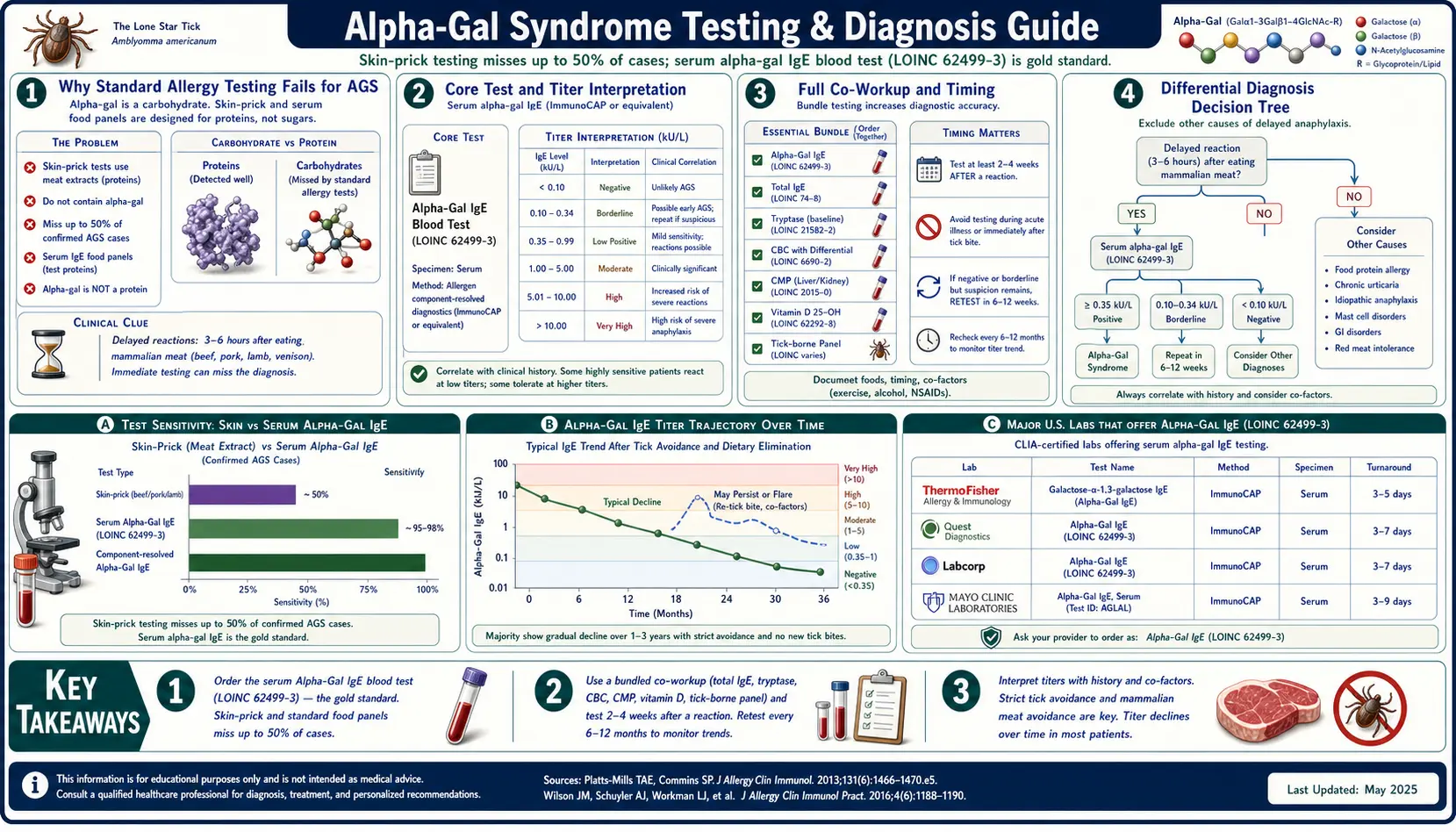
Table of Contents
- Why Standard Allergy Testing Fails for AGS
- The Core Test: Alpha-Gal-Specific IgE
- Labs Offering Alpha-Gal IgE
- Why Timing Matters
- Total IgE + Component Testing
- Tryptase — For MCAS Overlap
- Skin-Prick Testing (Limited Usefulness)
- Oral Food Challenge
- Differential Diagnosis — What Else Could It Be
- Co-Workup to Order Alongside Alpha-Gal IgE
- How to Advocate When Your Doctor Doesn’t Know AGS
- Tracking Titer Over Time
- Pediatric Considerations
- Insurance Coding
- At-Home Testing Options
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why Standard Allergy Testing Fails for AGS
If you walk into a typical allergist’s office with textbook alpha-gal syndrome symptoms — hives or anaphylaxis three to six hours after a steak dinner — there is a real chance you will walk out told that you are not allergic to meat. That is because the first test most allergists reach for — the skin-prick test — is the wrong tool for this particular allergy.
Classic skin-prick testing uses raw protein extracts applied to the skin for a short incubation, then reads the wheal within 15–20 minutes. It works beautifully for peanut, shellfish, dust mite, and grass pollen, because those are fast-presenting protein allergens. Alpha-gal is different. It is a carbohydrate (galactose-alpha-1,3-galactose) bound to a lipid, absorbed slowly through the gut after a fatty meal, with symptoms appearing three to six hours later. That biochemistry does not reproduce in a skin prick.
The result: up to 50% of AGS patients test negative on skin prick even when they have a clearly positive alpha-gal specific IgE blood test and a textbook clinical history. The gold standard for AGS diagnosis is a serum alpha-gal IgE blood test, not skin testing.
2. The Core Test: Alpha-Gal-Specific IgE
This is the single most important test. Everything else is supportive.
What to ask for
Tell your doctor: “Alpha-gal IgE” or “Galactose-alpha-1,3-galactose IgE.” The LOINC code is 62499-3. Printing that LOINC on a note you hand the front desk cuts through a lot of confusion.
Reference range
Reference ranges vary slightly between labs, but generally:
- <0.10 kU/L — negative
- 0.10–0.35 kU/L — low positive or indeterminate
- >0.35 kU/L — positive
Titer interpretation
- 0.35–2 kU/L: mild sensitization. Symptoms possible with high-fat mammalian meals plus cofactors (alcohol, exercise, NSAIDs, hot shower, menstrual cycle).
- 2–10 kU/L: moderate AGS. Symptoms typically occur with ordinary mammalian meals.
- 10–50 kU/L: severe AGS. Small exposures — gelatin, a bite of bacon, cross-contamination — can trigger reactions.
- >50 kU/L: very high titer. Strict avoidance and full anaphylaxis preparedness are critical.
Cost
Cash price is typically $50–$150. Insurance usually covers the test when AGS-consistent symptoms are documented in the chart (hives, GI distress, or anaphylaxis after red meat).
3. Labs Offering Alpha-Gal IgE
Five major labs run alpha-gal IgE. Results are directly comparable because all of them are now built on standardized ImmunoCAP chemistry or equivalent.
Viracor Eurofins
Viracor Eurofins specializes in food and environmental IgE and runs its own validated assay. Turnaround is typically the fastest — three to five business days.
Mayo Clinic Laboratories
Mayo Clinic Labs is reliable, widely used, and accessible through most health systems via send-out. Mayo was one of the institutions that helped characterize AGS clinically.
LabCorp
LabCorp uses ImmunoCAP. It is the easiest order for most primary-care offices because the account is usually already in place.
Quest Diagnostics
Quest Diagnostics also uses ImmunoCAP. Equivalent to LabCorp for the alpha-gal assay.
ARUP Laboratories
ARUP Labs is used by many academic medical centers and offers alpha-gal IgE as part of their standard immunology menu.
4. Why Timing Matters
Alpha-gal IgE titer is not static. It rises after tick bites and after reaction events, and it falls with sustained avoidance. When you draw the blood changes the number you see.
- Within weeks of a reaction: highest sensitivity. Titer peaks roughly 2–4 weeks post-exposure. If you are chasing a diagnosis after a suspected AGS reaction, test soon.
- Baseline measurement: wait at least 4 weeks after the last reaction for a stable number you can use as a tracking baseline.
- Trajectory: retest every 6–12 months. A downward trend suggests tolerance building; an upward trend suggests new tick exposure.
5. Total IgE + Component Testing
Total IgE
Total IgE puts your alpha-gal number in context. Someone with very high total IgE (above 1000 IU/mL from atopic disease or parasite exposure) may have a diluted alpha-gal specific reading. Some researchers argue the ratio of alpha-gal IgE to total IgE is a better marker of allergic potential than the alpha-gal number alone.
Component testing for co-existing meat allergy
A full food-component panel can rule out classical IgE meat-protein allergy, which is a different diagnosis with different management. The key components are bos d 6 (bovine serum albumin, beef) and sus s 1 (pork serum albumin). A positive alpha-gal IgE with negative bos d 6 and sus s 1 is the classic AGS pattern.
6. Tryptase — For MCAS Overlap
A meaningful fraction of AGS patients have elevated baseline tryptase or concurrent mast cell activation syndrome. Reactions tend to be more severe, more multi-system, and more unpredictable when both conditions coexist.
- Serum total tryptase — draw at baseline (not during a reaction). Normal is typically <11.4 ng/mL.
- If baseline tryptase is >8 ng/mL, consider genetic testing for hereditary alpha-tryptasemia (HαT), which is a TPSAB1 gene copy-number variant.
- See the Hereditary Alpha-Tryptasemia page for genetic testing logistics.
7. Skin-Prick Testing (Limited Usefulness)
Skin testing is not the diagnostic workhorse for AGS, but there are scenarios where an allergist may still perform it.
Commercial meat extract prick
Standard commercial extracts of beef, pork, and lamb are often negative in confirmed AGS. A negative result here does not rule out AGS.
Fresh food prick-to-prick
Higher sensitivity. The allergist pricks a piece of patient-supplied fresh raw meat and then pricks your skin with the same lancet. Better catches the carbohydrate-lipid complex, though still imperfect.
Intradermal testing
Can convert positive when prick is negative, but intradermal testing carries higher anaphylaxis risk during the procedure itself. It should only be done in an allergist’s office with epinephrine and monitoring available.
8. Oral Food Challenge
An oral food challenge — eating a measured dose of mammalian meat under medical supervision — is not a routine diagnostic step for AGS. Blood IgE plus a consistent clinical history is usually sufficient, and the delayed timing of reactions makes in-office challenges impractical. Oral challenges are reserved for supervised research protocols or carefully designed re-introduction attempts in patients whose titer has dropped substantially.
9. Differential Diagnosis — What Else Could It Be
Several conditions mimic AGS. A clean workup rules them in or out.
- FPIES (food protein-induced enterocolitis syndrome): delayed GI reaction (vomiting, diarrhea) but typically no hives or anaphylaxis. IgE testing is negative.
- Classical meat allergy: immediate IgE reaction (minutes, not hours) to specific meat proteins such as bos d 6 or sus s 1, not the alpha-gal sugar.
- Red meat intolerance: no IgE involvement; dose-dependent GI symptoms, not severe, not anaphylactic.
- Mast cell activation syndrome (MCAS): multi-trigger, multi-system. Often coexists with AGS. See Mediators & Symptom Map.
- Hereditary alpha-tryptasemia (HαT): genetic trait with elevated baseline tryptase and multi-system hyperreactivity.
- Histamine intolerance: overlaps with MCAS and responds to DAO supplementation and histamine-lowering diet.
- Exercise-induced anaphylaxis (no specific food trigger): distinct entity; worth considering if reactions only occur with exercise.
10. Co-Workup to Order Alongside Alpha-Gal IgE
When you are going to the trouble of a blood draw, order the full supporting panel in one go:
- Tryptase — MCAS screen.
- Complete blood count (CBC) with differential — eosinophilia is a clue to atopic load.
- Comprehensive metabolic panel — baseline organ function.
- Thyroid panel (TSH, free T4, TPO antibodies) — autoimmune thyroid disease co-occurs with AGS more than chance.
- Lyme serology — Western blot, not just ELISA. The same tick bite that delivered alpha-gal can transmit Borrelia. ELISA alone misses a meaningful number of Lyme cases.
- Anti-vinculin and anti-CdtB antibodies — if you have SIBO-pattern GI symptoms.
- Vitamin B12, ferritin, iron studies — dietary restriction plus mammalian avoidance can push nutrient levels down.
11. How to Advocate When Your Doctor Doesn’t Know AGS
AGS is still under-recognized outside the southeastern United States. Many primary-care physicians have heard of it only in passing. You may need to advocate.
- Bring a printed copy of the CDC Alpha-Gal Syndrome Overview (cdc.gov/ticks/alphagal/).
- Bring a one-page summary of the 2020 Platts-Mills JACI review on diagnosis and management.
- Say: “Please order alpha-gal-specific IgE through LabCorp, Quest, or Viracor.”
- If your PCP refuses, most insurers allow self-referral to allergy/immunology without a gatekeeper.
- Telemedicine allergists increasingly AGS-aware: Mayo Clinic, Cleveland Clinic, Vanderbilt, UNC Chapel Hill, and UVA (Thomas Platts-Mills’s institution and the global epicenter of AGS research).
12. Tracking Titer Over Time
AGS is one of the few food allergies that can genuinely resolve. Tracking your titer tells you whether you are heading that direction.
- Every 6 months for the first 2 years post-diagnosis, then annually if trending downward.
- Graph your results. A spreadsheet with date and titer value, plotted, reveals trend faster than reading numbers in isolation.
- A new tick bite typically causes a 2–4x titer spike within 4–8 weeks. If your number jumps, check yourself for bites and review your outdoor exposure.
- Sustained strict avoidance typically halves titer every 1–2 years, though individual variability is huge. Some patients drop fast; others plateau for years.
- Titer below 2 kU/L is associated in some research with loosening tolerance. Do not self-experiment — discuss carefully supervised re-introduction with your allergist. See Natural History and Tolerance.
13. Pediatric Considerations
AGS is less common in children than in adults but does occur, particularly in rural and outdoor-active kids in the tick-endemic southeastern, mid-Atlantic, and lower midwestern United States. The testing approach is the same — alpha-gal specific IgE — and the threshold for ordering it should be low in any child with unexplained recurrent urticaria, delayed anaphylaxis, or GI distress hours after meat. Ask about tick exposure explicitly; children often do not report bites.
14. Insurance Coding
If the claim is denied, these are the codes that tend to work:
- ICD-10 T78.07XA — anaphylaxis due to mammalian (red) meat, initial encounter.
- ICD-10 Z91.048 — other (non-nut, non-seafood) food allergy status by history.
- CPT 86008 or CPT 86003 — allergen-specific IgE by immunoassay (alpha-gal IgE).
15. At-Home Testing Options
Direct-to-consumer allergy testing has expanded, but AGS-specific options remain narrow.
- Viracor direct-to-consumer is available in some states and offers physician-network ordering.
- Everlywell, imaware, and LetsGetChecked sell food allergy panels, but AGS-specific coverage is inconsistent — check the panel contents before buying.
- Best approach: physician-ordered alpha-gal IgE through LabCorp, Quest, Mayo, Viracor, or ARUP. Get your doctor on board — the result goes into your medical record, the cost is often lower, and the result triggers real clinical follow-up.
16. Key Research Papers
- Platts-Mills TAE, et al. Diagnosis and management of α-Gal syndrome. J Allergy Clin Immunol Pract. 2020.
- Commins SP, et al. Delayed anaphylaxis, angioedema, or urticaria after red meat in patients with IgE antibodies specific for galactose-alpha-1,3-galactose. J Allergy Clin Immunol. 2009.
- Pattanaik D, et al. Clinical manifestations of the α-gal syndrome. Ann Allergy Asthma Immunol. 2019.
- Fischer J, Biedermann T. Delayed immediate-type hypersensitivity to red meat and innards. 2016.
17. Research Papers
PubMed searches for deeper reading:
- alpha gal IgE testing
- galactose alpha 1 3 galactose IgE
- alpha gal skin prick test
- alpha gal titer trajectory
- alpha gal diagnosis review
- ImmunoCAP alpha gal
- alpha gal tryptase MCAS
- alpha gal hereditary alpha tryptasemia
Connections
- Natural History and Tolerance
- Mast Cell Activation Syndrome
- Alpha-Gal Syndrome Overview
- Allergies
- Hereditary Alpha-Tryptasemia
- Tick Bite Prevention
- Mammalian Foods List
- Tick-Origin Science
- Restaurant and Travel Survival
- Cross-Reactive Medications
- Anaphylaxis Emergency Plan
- Lyme Disease
- Food Intolerance
- MCAS Mediators and Symptom Map
- Complete Blood Count
- Alpha-Gal and Cardiovascular Risk