MCAS Testing Guide
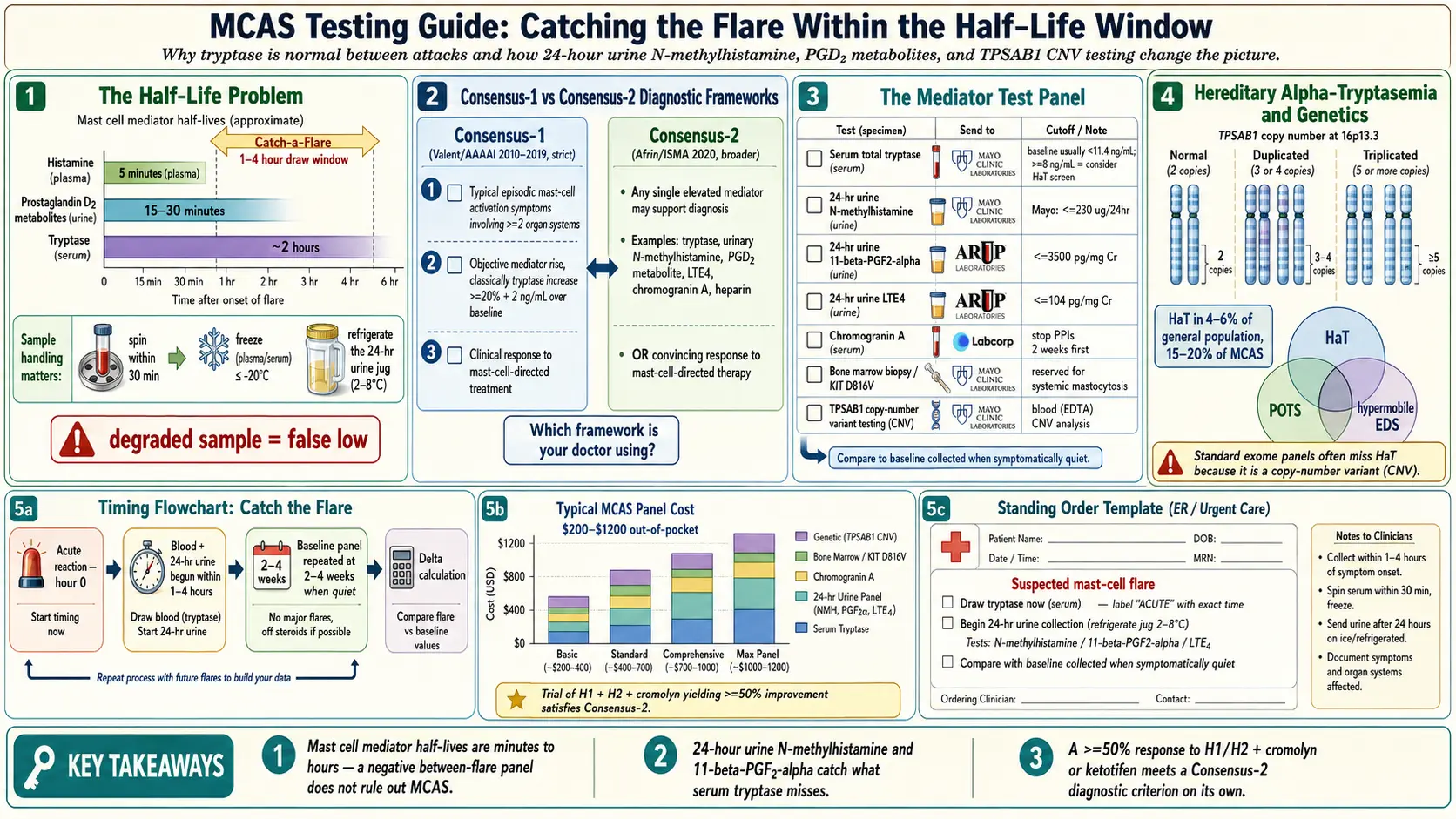
Table of Contents
- Why MCAS Testing Is Frustrating
- The Two Competing Diagnostic Frameworks
- Serum Tryptase
- 24-Hour Urine N-Methylhistamine
- 24-Hour Urine Prostaglandin D2 Metabolite
- 24-Hour Urine Leukotriene E4
- Chromogranin A
- Plasma Histamine
- Bone Marrow Biopsy
- Genetic Testing for Hereditary Alpha-Tryptasemia
- Timing Strategy — The “Catch a Flare” Approach
- What to Do With “All-Normal” Tests
- Labs That Do MCAS Testing Well
- At-Home Test Kits
- Costs and Insurance
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why MCAS Testing Is Frustrating
If you’ve been told your tryptase is “normal” and therefore you don’t have mast cell activation syndrome, you need to understand something before your next appointment: mast cell mediators have extremely short half-lives. The biology of the test is working against you.
- Tryptase has a half-life of roughly 2 hours.
- Histamine — just 5 minutes in plasma.
- Prostaglandin D2 metabolites — 15–30 minutes.
If your blood is drawn between flares — which is the default when you show up at a routine appointment — most results will look perfectly normal. This does not mean you don’t have MCAS. It means the test was timed badly. You are measuring whether a fire is burning by walking through the kitchen an hour after it was put out.
The second hidden obstacle: sample handling. Mast cell mediators are delicate. 24-hour urine samples must be kept chilled during collection. Plasma samples for histamine and PGD2 must be placed on ice and spun down into plasma within specific time windows (often under 30 minutes), then frozen. Many hospital labs don’t handle these samples correctly, and the degraded result comes back falsely low. Ask the ordering physician to confirm with the lab exactly how samples must be collected, transported, and processed before collection day.
None of this is your fault, and none of it is in your head.
2. The Two Competing Diagnostic Frameworks
There is no single agreed-upon definition of MCAS. There are two, and which one your doctor uses dictates whether you get a diagnosis.
Consensus-1 (Valent / AAAAI, 2010; updated 2019)
Requires all three:
- Typical episodic symptoms involving at least two organ systems (skin, GI, cardiovascular, respiratory).
- An acute ≥20% + 2 ng/mL rise in serum tryptase above the patient’s own baseline, measured during a flare.
- Response to antihistamines or mast-cell-targeted therapy.
This is the stricter framework. The tryptase-rise criterion is the one most patients “fail” — either because the flare wasn’t timed right for a draw, or because their mast cells release histamine and prostaglandins without releasing much tryptase. Many real patients are excluded.
Consensus-2 (Afrin / ISMA, 2020)
Requires:
- Typical mast-cell-mediator symptoms (same multi-system picture).
- Any single elevated mast cell marker — tryptase, urinary histamine metabolites, prostaglandin D2, leukotriene E4, chromogranin A, or heparin — OR a convincing clinical response to mast-cell-directed treatment.
This framework is broader and catches far more real-world patients. It was built by clinicians who were watching patients with textbook symptoms get turned away because of the tryptase-rise rule.
Which framework your doctor uses matters enormously. Most allergist-immunologists trained in the last decade default to Consensus-1 and will tell you “you don’t meet criteria.” MCAS-specialized physicians (often fewer in number and further away) tend toward Consensus-2. If you’re being dismissed, ask directly: “Are you using Consensus-1 or Consensus-2 criteria?” The answer tells you what you’re up against.
3. Serum Tryptase
Order: “total serum tryptase.”
Baseline reference: <11.4 ng/mL is normal. Anything above that raises suspicion for hereditary alpha-tryptasemia (HαT) or systemic mastocytosis.
During a flare: draw within 1–4 hours of an acute reaction; the ideal window is 1–2 hours. Repeat at a quiet baseline 2–4 weeks later. The Consensus-1 diagnostic rise is ≥20% + 2 ng/mL above that personal baseline.
Tryptase is relatively forgiving on handling — it’s stable at room temperature for 24–48 hours, so sample mishandling is less of an issue than with other mast cell markers.
4. 24-Hour Urine N-Methylhistamine
For many patients this is the single most useful MCAS test — more useful than tryptase — because it captures accumulated histamine activity over an entire day rather than a single moment.
Order: “24-hour urine N-methylhistamine.” Available through Mayo Clinic Labs, ARUP, and LabCorp.
How it works: you are given a large collection jug and asked to collect every urination for 24 hours. The jug must be kept in the refrigerator throughout the collection. Skip that step and the histamine degrades.
Reference cutoffs vary by lab. Mayo considers ≤230 µg/24 hr normal. Because reference ranges differ, always read them off your own report, not a web page.
This test’s great advantage is that it is far less dependent on flare timing. If you have frequent low-grade activation, the histamine piles up across 24 hours and shows as an elevated metabolite — even if no single moment looked dramatic.
5. 24-Hour Urine Prostaglandin D2 Metabolite (11β-PGF2α)
PGD2 is a mast-cell-specific prostaglandin. Its urine metabolite 11β-prostaglandin F2α is one of the strongest indicators of MCAS when elevated, particularly in patients whose tryptase is stubbornly normal.
Order: “24-hour urine 11-beta-prostaglandin F2-alpha” (or “PGD2 metabolite”).
Mayo reference: roughly ≤3500 pg/mg creatinine (ranges vary by lab and method).
If your clinician doubts you, an elevated PGD2 metabolite is often the finding that tips the conversation. It is highly specific for mast cell activity.
6. 24-Hour Urine Leukotriene E4 (LTE4)
Leukotrienes drive airway and GI symptoms. Elevated LTE4 is especially informative in patients with asthma, chronic rhinosinusitis, nasal polyps, or GI-dominant MCAS.
Mayo reference: ≤104 pg/mg creatinine.
A positive LTE4 also hints that montelukast or zileuton may help — useful information for the treatment plan.
7. Chromogranin A
A serum test that rises in MCAS, systemic mastocytosis, and neuroendocrine tumors.
Critical caveat: proton pump inhibitors (omeprazole, pantoprazole, esomeprazole) produce falsely elevated chromogranin A. You must stop PPIs for at least 2 weeks before the draw or the number is meaningless. H2 blockers do not cause this interference.
8. Plasma Histamine
Generally not useful. Histamine’s 5-minute half-life means that unless you are drawing blood mid-anaphylaxis, the level will be normal. Plasma N-methylhistamine is slightly more durable but still inferior to the 24-hour urine version for practical use. If your doctor wants to order plasma histamine, politely ask for the 24-hour urine N-methylhistamine instead.
9. Bone Marrow Biopsy
Reserved for suspected systemic mastocytosis, not routine MCAS. Indications include a persistently elevated baseline tryptase (often above 20 ng/mL), unexplained cytopenias, or hepatosplenomegaly. The biopsy looks for mast cell clusters, aberrant CD25 expression, and the KIT D816V mutation. Most MCAS patients never need this test.
10. Genetic Testing for Hereditary Alpha-Tryptasemia (HαT)
If your baseline tryptase runs above 8 ng/mL — even though that’s technically in the “normal” range — consider TPSAB1 copy number variant (CNV) testing. Duplication or triplication of the TPSAB1 gene defines hereditary alpha-tryptasemia.
Labs: Gene by Gene and Genetic Testing Laboratories run the assay. Most standard exome panels miss it because it’s a copy-number variant, not a point mutation.
HαT affects 4–6% of the general population but 15–20% of MCAS patients. It frequently overlaps with POTS and hypermobile EDS. See the Hereditary Alpha-Tryptasemia article for the full story.
11. Timing Strategy — The “Catch a Flare” Approach
Because mediator levels collapse between flares, the only reliable way to capture a positive result is to test while you are actively reacting. Plan this in advance, before you are flaring.
- During an acute reaction (within 1–4 hours): go to an urgent care, ER, or arranged outpatient draw and get (a) serum tryptase; (b) start the 24-hour urine collection (N-methylhistamine, PGD2 metabolite, LTE4).
- Baseline comparison (2–4 weeks later, when quiet): repeat the same panel. The delta is what makes the diagnosis under Consensus-1.
- Pre-emptive flare induction — a controlled food, temperature, or exercise challenge done only at an experienced MCAS center, then immediate testing. Rarely needed and carries real risk.
Practical tip: pre-prepare a standing order. Some immunologists will write you a blood-draw order that lives in your chart, so that if you flare you can walk into a lab or ER and hand it over without negotiating. Ask for it explicitly.
12. What to Do With “All-Normal” Tests
Perfectly normal tests do not rule out MCAS. This is the single most important sentence on this page. Your options from here:
- Repeat the panel during another flare. Timing is everything. A negative between-flare panel and a positive during-flare panel are two different experiments.
- Trial of mast-cell-targeted treatment. A convincing response — generally a ≥50% symptom improvement on an H1 + H2 blocker stack plus cromolyn or ketotifen — satisfies a Consensus-2 criterion on its own. This is diagnostically legitimate, not a placebo experiment.
- Expand to less-common markers: chymase, heparin (difficult to measure accurately), plasma PGD2, or a broader Mayo MCAS panel.
- Seek out an MCAS-literate immunologist. Not all allergists read the MCAS literature. Patient advocacy groups (The Mastocytosis Society, TMS) maintain informal lists of clinicians known to take MCAS seriously.
You are not obligated to accept a dismissal simply because one panel came back inside the reference range.
13. Labs That Do MCAS Testing Well
- Mayo Clinic Labs — the gold standard for the MCAS panel; trusted reference ranges for N-methylhistamine, PGD2 metabolite, and LTE4.
- ARUP Laboratories — comparable quality, often faster turnaround.
- LabCorp and Quest Diagnostics — offer the mainstream markers; confirm sample handling details before collection.
- Ackerman Cancer Center — historically referenced for specialized PGD2 assays.
- Gene by Gene — TPSAB1 copy-number variant testing for HαT.
Always ask your ordering physician to confirm sample handling requirements with the specific lab before collection day. A single mishandled tube can waste a flare that may not return for months.
14. At-Home Test Kits (Limited Options)
- Vibrant Wellness MCAS panel — includes urinary histamine, PGD2, and LTE4. Insurance often denies coverage, so budget cash.
- Cyrex Labs — advanced histamine and immune panels.
Results from these kits are not always accepted by mainstream allergist-immunologists, who may view them as “not standardized.” That said, they can be useful data, especially if mainstream labs keep coming back unremarkable and you want another signal. Bring the report to a clinician who respects the findings rather than one who will wave it away.
15. Costs and Insurance
- Serum tryptase: $30–80, usually covered.
- 24-hour urine mediator panels: $150–400 per marker. Mayo and ARUP are typically covered with prior authorization; commercial plans vary.
- TPSAB1 CNV testing: $300–600 cash; rarely covered by insurance.
- Prior authorization is often required. A letter from your clinician citing MCAS clinical criteria and the specific suspected mediator pattern materially improves approval odds.
If cost is a barrier, prioritize in this order: (1) serum tryptase during a flare + baseline pair, (2) 24-hour urine N-methylhistamine, (3) 24-hour urine PGD2 metabolite. That three-test bundle catches the majority of positives.
16. Key Research Papers
- Valent P, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. J Allergy Clin Immunol. 2019.
- Afrin LB, et al. Diagnosis of mast cell activation syndrome: a global “consensus-2.” Diagnosis (Berl). 2020.
- Weiler CR, et al. AAAAI Mast Cell Disorders Committee Work Group Report: Mast cell activation syndrome (MCAS) diagnosis and management. J Allergy Clin Immunol. 2019.
- Lyons JJ, et al. Elevated basal serum tryptase identifies a multisystem disorder associated with increased TPSAB1 copy number. Nat Genet. 2016.
17. Research Papers
Curated PubMed topic searches of peer-reviewed literature on MCAS testing. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: MCAS diagnostic criteria
- PubMed: Serum tryptase in MCAS
- PubMed: 24-hour urine N-methylhistamine
- PubMed: Prostaglandin D2 in MCAS
- PubMed: Hereditary alpha-tryptasemia and TPSAB1
- PubMed: MCAS and leukotriene E4
- PubMed: Mast cell activation criteria (Afrin)
Connections
- MCAS Overview
- Hereditary Alpha-Tryptasemia
- H1 and H2 Blocker Stacks
- Cromolyn and Ketotifen Protocols
- Alpha-Gal Syndrome
- POTS
- Triggers and Flare Management
- Natural Mast Cell Stabilizers
- Low-Histamine Diet
- Mediators and Symptom Map
- Allergies
- SIBO
- Ehlers-Danlos Syndrome
- Chronic Fatigue Syndrome (ME/CFS)
- Hormone Sensitivity: Estrogen & Menstrual Flares
- POTS MCAS EDS Triad
- POTS MCAS and the EDS Triad
- Tryptase — the lab test itself: reference ranges, draw timing, and what a baseline value means.