Cromolyn and Ketotifen Protocols for MCAS
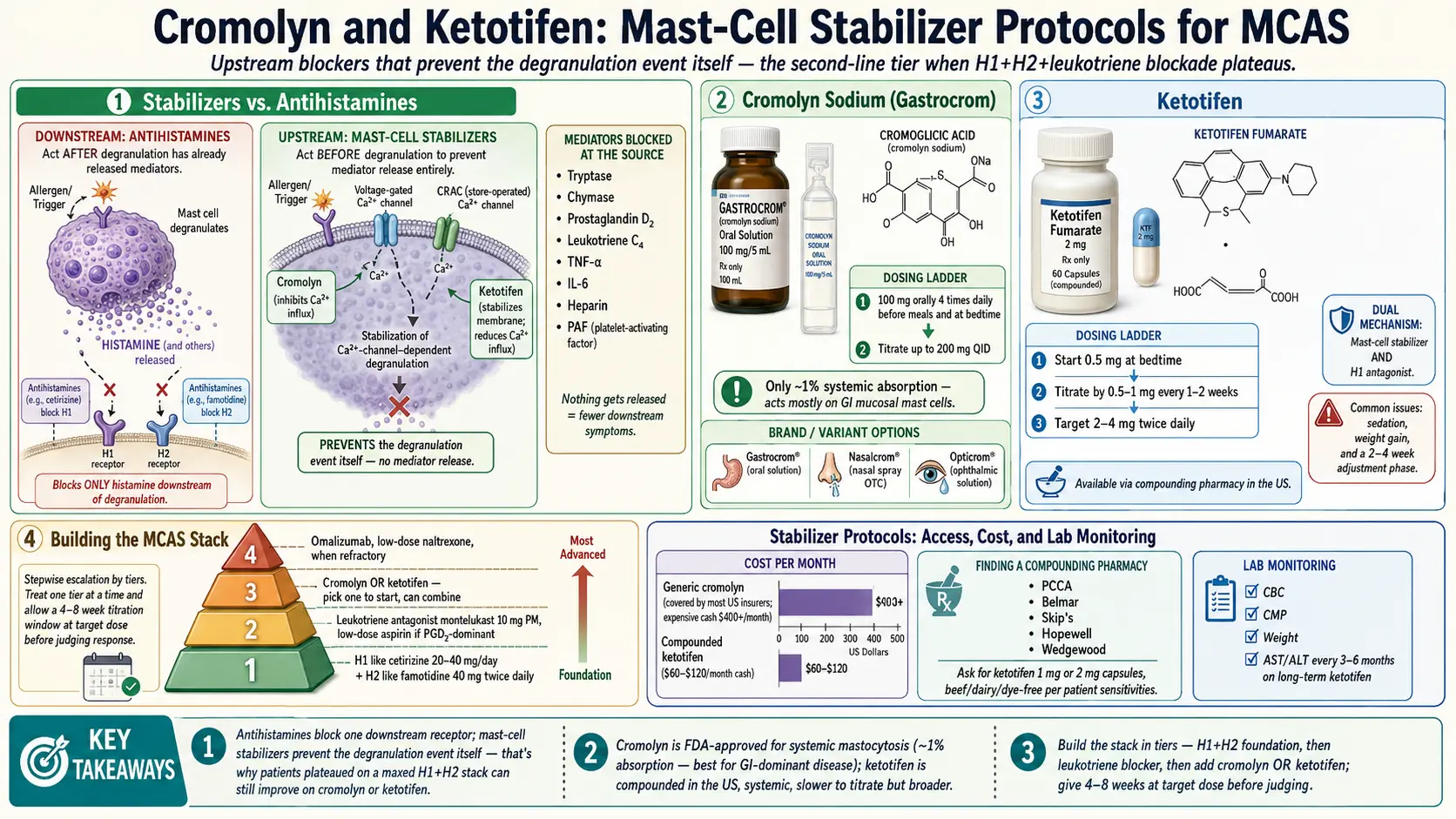
Table of Contents
- Why Stabilizers Are Different from Antihistamines
- Cromolyn Sodium (Gastrocrom, Nalcrom, Nasalcrom, Opticrom)
- Cromolyn Dosing Protocol
- Cromolyn Side Effects & Troubleshooting
- Cromolyn Costs & Access
- Ketotifen
- Ketotifen Dosing Protocol
- Ketotifen Side Effects
- Ketotifen Costs & Access
- Finding a Compounding Pharmacy
- Cromolyn vs Ketotifen — Which to Pick?
- Combining with the H1/H2 Stack
- When Stabilizers Aren’t Enough
- Lab Monitoring
- Stopping Stabilizers
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why Stabilizers Are Different from Antihistamines
Antihistamines — cetirizine, famotidine, loratadine, diphenhydramine — only work after the mast cell has already released histamine. They compete at the H1 or H2 receptor, blocking the signal from being received. That’s useful, but it’s downstream damage control.
Mast cell stabilizers work upstream. They bind to the mast cell membrane itself, stabilize calcium channels, and prevent the degranulation event from happening in the first place. When a mast cell doesn’t degranulate, it doesn’t release anything — not just histamine, but also tryptase, chymase, prostaglandin D2, leukotriene C4, TNF-alpha, IL-6, heparin, and platelet-activating factor.
This is why patients who have plateaued on a maxed-out H1+H2+montelukast stack can still improve on a stabilizer. The antihistamines were blocking one downstream receptor family. The stabilizer cuts off the whole cascade at the source.
2. Cromolyn Sodium (Gastrocrom, Nalcrom, Nasalcrom, Opticrom)
Cromolyn sodium (also called cromoglicic acid or disodium cromoglycate) has been around since the 1960s. It’s sold under several brand names depending on the route of administration:
- Gastrocrom (US) / Nalcrom (UK, EU, Canada) — oral concentrate for systemic MCAS, 100 mg/5 mL ampules
- Nasalcrom — OTC nasal spray for allergic rhinitis
- Opticrom / Crolom — ophthalmic drops for allergic conjunctivitis
- Intal — inhaler for asthma (largely discontinued in the US)
FDA Approvals
Cromolyn is formally approved for systemic mastocytosis, allergic conjunctivitis, and allergic rhinitis. MCAS use is off-label, but the mastocytosis indication is close enough that most informed prescribers are comfortable writing it.
How It Works — and Its Biggest Limitation
Oral cromolyn binds to the mast cell membrane and stabilizes the calcium channels that drive degranulation. The catch: less than 1% of oral cromolyn is systemically absorbed. It works almost entirely locally in the GI tract.
That’s great news if your dominant symptoms are food reactions, diarrhea, cramping, or bloating — the drug sits exactly where it’s needed. It’s less great if your flares are skin, brain fog, or flushing without gut involvement. That said, intestinal mast cells generate a large fraction of systemic mediator load, so many patients report surprising whole-body benefit even with a gut-local drug.
3. Cromolyn Dosing Protocol
Standard Adult Dose
- 200 mg (2 ampules = 10 mL) four times daily — before each meal plus at bedtime
- Total daily dose: 800 mg/day
- Mix each dose in about 1/2 cup of water, drink 15–30 minutes before meals and at bedtime
- Do not mix with juice or food at the time of dosing (though juice can be used after for taste rinse)
Start Low, Titrate Up
Rapid dose escalation can trigger a paradoxical flare in mast-cell-sensitive patients. Start with:
- 100 mg twice daily (BID) for 5–7 days
- Increase by 100 mg every 5–7 days as tolerated
- Target: 200 mg QID over 3–4 weeks
Pediatric Dosing
100 mg four times daily for children — same before-meals-plus-bedtime schedule.
Time to Effect
Antihistamines work within an hour. Cromolyn does not. Expect:
- 2–6 weeks for noticeable symptom reduction
- 3–4 months for full therapeutic effect
If you’re two weeks in and see nothing, that doesn’t mean it isn’t working — keep going. Premature discontinuation is the most common reason patients fail cromolyn.
Do Not Stop Abruptly
Mast cells primed on a stabilizer can rebound if the drug is pulled overnight. Taper over 2–4 weeks if discontinuing.
4. Cromolyn Side Effects & Troubleshooting
- Paradoxical flare in weeks 1–2. Common. Drop dose by 50% for 3–5 days, then re-escalate more slowly. This usually resolves and is not a reason to abandon the drug.
- Headache or dizziness. Usually transient; typically fades by week 3.
- GI upset. Taking the dose with a small amount of food reduces nausea (at the cost of some efficacy). Dilute the ampule in more water.
- Bitter taste. The concentrate is genuinely unpleasant. Mix in more water or follow with a fruit-juice chaser.
- True allergic reaction to cromolyn. Rare — roughly 0.1% of users. If you develop a rash, respiratory symptoms, or anaphylaxis after a dose, stop immediately.
5. Cromolyn Costs & Access
- Gastrocrom (brand): $500–900/month retail. Insurance often covers with prior authorization if the indication is mastocytosis; MCAS off-label coverage is harder to secure.
- Compounded cromolyn oral solution: $200–400/month from a compounding pharmacy. Same active ingredient, much lower price.
- Nasalcrom (OTC nasal spray): $15–30. Useful for nasal/sinus MCAS and can be used alongside oral cromolyn.
- Opticrom / Crolom (eye drops): OTC in the US. Useful for ocular itching, redness, and conjunctival flares.
Insurance tip: have the prescription written with a mastocytosis ICD-10 code (D47.02 or Q82.2) if clinically defensible. MCAS coding (D89.40–.49) is newer and some formularies haven’t caught up.
6. Ketotifen
Ketotifen fumarate is a benzocycloheptathiophene antihistamine with dual action. Commercially sold as Zaditen (EU, Canada, UK, Australia) and Ketof (Asia), oral ketotifen is not commercially available in the United States. US patients must source it through a compounding pharmacy.
FDA Status
In the US, only the ophthalmic form (Zaditor, Alaway) is FDA-approved — for allergic conjunctivitis. In other countries, oral ketotifen is approved for pediatric asthma prophylaxis and chronic urticaria. MCAS use is off-label everywhere.
How It Works — Dual Mechanism
Ketotifen does two things at once:
- H1 antihistamine — blocks the histamine-1 receptor (similar to cetirizine, but sedating)
- Mast cell stabilizer — prevents degranulation of mast cells and basophils
This is useful when you want one drug to cover two mechanisms — especially for a patient who has not yet committed to a large stack and wants a simpler trial. Unlike cromolyn, ketotifen is systemically absorbed, so it works on mast cells throughout the body, not just the gut.
7. Ketotifen Dosing Protocol
Adult Target Range
1–4 mg total daily, usually dosed at bedtime because of the sedation profile.
Titration Schedule
- Week 1: 0.5–1 mg qhs (at bedtime)
- Week 2: 1–2 mg qhs
- Weeks 3–4: 2–4 mg qhs as tolerated
BID vs Bedtime-Only
Some patients do better with a split dose (for example, 1–2 mg AM + 1–2 mg PM), especially when flares occur during the day. Others find daytime dosing intolerably sedating and prefer bedtime-only. Start with bedtime, then decide.
Time to Effect
- Antihistamine effect: immediate — same night
- Stabilization effect: 2–4 weeks to develop fully
8. Ketotifen Side Effects
- Sedation — the main one. Drowsiness is almost universal in the first 1–2 weeks. Most patients tolerize. If you still feel flattened at week 3, drop back a step.
- Weight gain. A real issue — typically 5–10 lbs over 6 months from appetite stimulation. Worth knowing in advance.
- Dry mouth. Anticholinergic-adjacent effect.
- Urinary retention. Rare but possible, especially in older men with prostatic issues.
- Paradoxical insomnia. A small subset of patients are stimulated by ketotifen. If that happens, switch to AM dosing.
9. Ketotifen Costs & Access
- Compounded 1–4 mg capsules: $30–60/month cash pay — dramatically cheaper than Gastrocrom
- Insurance rarely covers compounded medications, but the cash price is usually tolerable
US compounding pharmacies that stock or routinely make ketotifen (patient-verified through MCAS communities):
- Skip’s Pharmacy (Florida)
- Belmar Pharmacy (Colorado)
- Olympia Pharmacy (Florida)
- ROIDrx (Texas)
- Nelson Pharmacy (Massachusetts)
All of these ship nationally. You usually do not need an in-person visit — your prescriber faxes or e-prescribes directly to the pharmacy.
10. Finding a Compounding Pharmacy
If you’re outside the reach of the pharmacies above, here is how to locate one locally:
- PCCA directory (Professional Compounding Centers of America). PCCA-member pharmacies are certified in compounding and searchable by state at pccarx.com.
- MCAS patient communities. MastAttack.org, The Mast Cell Disease Society (tmsforacure.org), and the larger Facebook MCAS groups maintain member-verified pharmacy lists. This is often more reliable than a blind directory search.
- Ask if they pre-weigh ketotifen. Pre-weighed bulk powder yields more consistent dosing than per-script weighing. It’s a reasonable sanity-check question.
- Ask about shipping. Ketotifen capsules are stable at room temperature and ship easily; most pharmacies ship overnight or 2-day. Cromolyn oral concentrate is also shelf-stable.
- Ask about dye-free and filler-free options. MCAS patients often react to capsule dyes, lactose fillers, or magnesium stearate. Good compounding pharmacies will substitute with hypoallergenic fillers on request.
11. Cromolyn vs Ketotifen — Which to Pick?
This is the most common question MCAS patients face when their H1/H2 stack plateaus. A practical decision tree:
- GI-dominant symptoms (food reactions, diarrhea, cramping, bloating, nausea with meals) → cromolyn. Acts locally in the gut, timed 15–30 min before meals to protect GI mast cells during digestion.
- Systemic symptoms (flushing, brain fog, fatigue, skin flares, insomnia, anxiety) → ketotifen. Absorbed systemically; reaches mast cells throughout the body.
- Severe insomnia + MCAS overlap → ketotifen. The sedation is a bonus, not a bug.
- Food sensitivities that dominate the clinical picture → cromolyn.
- Already on many daytime meds and fatigue is a concern → cromolyn (non-sedating).
Many Patients Take Both
The two drugs are complementary, not competitive. A common refractory-MCAS regimen is:
- Cromolyn 200 mg before each meal (4x daily) for GI protection, plus
- Ketotifen 1–4 mg at bedtime for systemic coverage and sleep
There is no meaningful drug-drug interaction between them.
12. Combining with the H1/H2 Stack
Stabilizers augment the antihistamine stack. They do not replace it. Keep running whatever combination you’ve built up — cetirizine, famotidine, montelukast, low-dose aspirin — and layer the stabilizer on top.
See H1 and H2 Blocker Stacks for the full antihistamine layer. The stabilizer addresses a different step in the cascade (release) than the antihistamines (receptor blockade), so their benefits are additive.
Patients who drop their antihistamines after starting cromolyn or ketotifen usually flare within days. Don’t do it unless a cautious taper is clearly indicated.
13. When Stabilizers Aren’t Enough
A subset of MCAS patients continue to flare even on maximally dosed antihistamines plus cromolyn plus ketotifen. The next tier:
- Omalizumab (Xolair). Anti-IgE monoclonal antibody, subcutaneous injection every 4 weeks. ~$2000+/month. Potent in refractory MCAS, especially with elevated serum IgE or co-existing chronic urticaria. Often the first biologic tried.
- Imatinib. Tyrosine kinase inhibitor, useful in KIT D816V-negative systemic mastocytosis. Rarely helpful in typical MCAS.
- Avapritinib (Ayvakit). FDA-approved for advanced systemic mastocytosis and indolent systemic mastocytosis. Selectively targets KIT D816V. Spectacular in KIT-positive disease; not indicated in standard MCAS.
- IVIG. Used in autoimmune-overlap MCAS, especially with co-existing CVID, small-fiber neuropathy, or autoimmune urticaria.
These tiers require a specialist — allergy/immunology, hematology, or an MCAS-focused clinic.
14. Lab Monitoring
Neither cromolyn nor ketotifen requires routine monitoring. Both drugs have decades of real-world safety data and no FDA-mandated lab schedule.
For long-term users (more than a year), a reasonable annual panel:
- CBC with differential
- Comprehensive metabolic panel including LFTs
More for general surveillance than drug-specific concern.
15. Stopping Stabilizers
If you need to discontinue — because the drug isn’t helping, because of a side effect, or because you’re transitioning to a biologic — taper over 2–4 weeks. Do not stop cold.
A typical taper for cromolyn: drop one ampule (100 mg) per week. For ketotifen: drop 0.5–1 mg every 5–7 days. Rebound flares during abrupt withdrawal are well-documented and can undo months of stabilization in a matter of days.
16. Key Research Papers
- Valent P, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. Journal of Allergy and Clinical Immunology. 2019.
- Molderings GJ, et al. Pharmacological treatment options for mast cell activation disease. Journal of Allergy and Clinical Immunology. 2016.
- Akin C. Treatment of mast cell activation disorders. Current Opinion in Allergy and Clinical Immunology. 2019.
- Afrin LB, et al. Diagnosis of mast cell activation syndrome: a global “consensus-2.” Allergy. 2020.
17. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: Cromolyn sodium in mastocytosis
- PubMed: Ketotifen and mast cells
- PubMed: MCAS treatment with stabilizers
- PubMed: Cromolyn in irritable bowel syndrome
- PubMed: Ketotifen for chronic urticaria
- PubMed: Omalizumab in mast cell disease
- PubMed: Mast cell stabilizer reviews
Connections
- MCAS Overview
- H1 and H2 Blocker Stacks
- Mediators and Symptom Map
- MCAS Testing Guide
- Low-Histamine Diet
- Triggers and Flare Management
- Natural Mast Cell Stabilizers
- Hereditary Alpha-Tryptasemia
- Hormone Sensitivity and Menstrual Flares
- POTS
- Allergies
- Alpha-Gal Syndrome
- SIBO
- Asthma
- Quercetin
- Bloating
- Brain Fog