IBD Fatigue, Anemia, and Nutrient Deficiencies
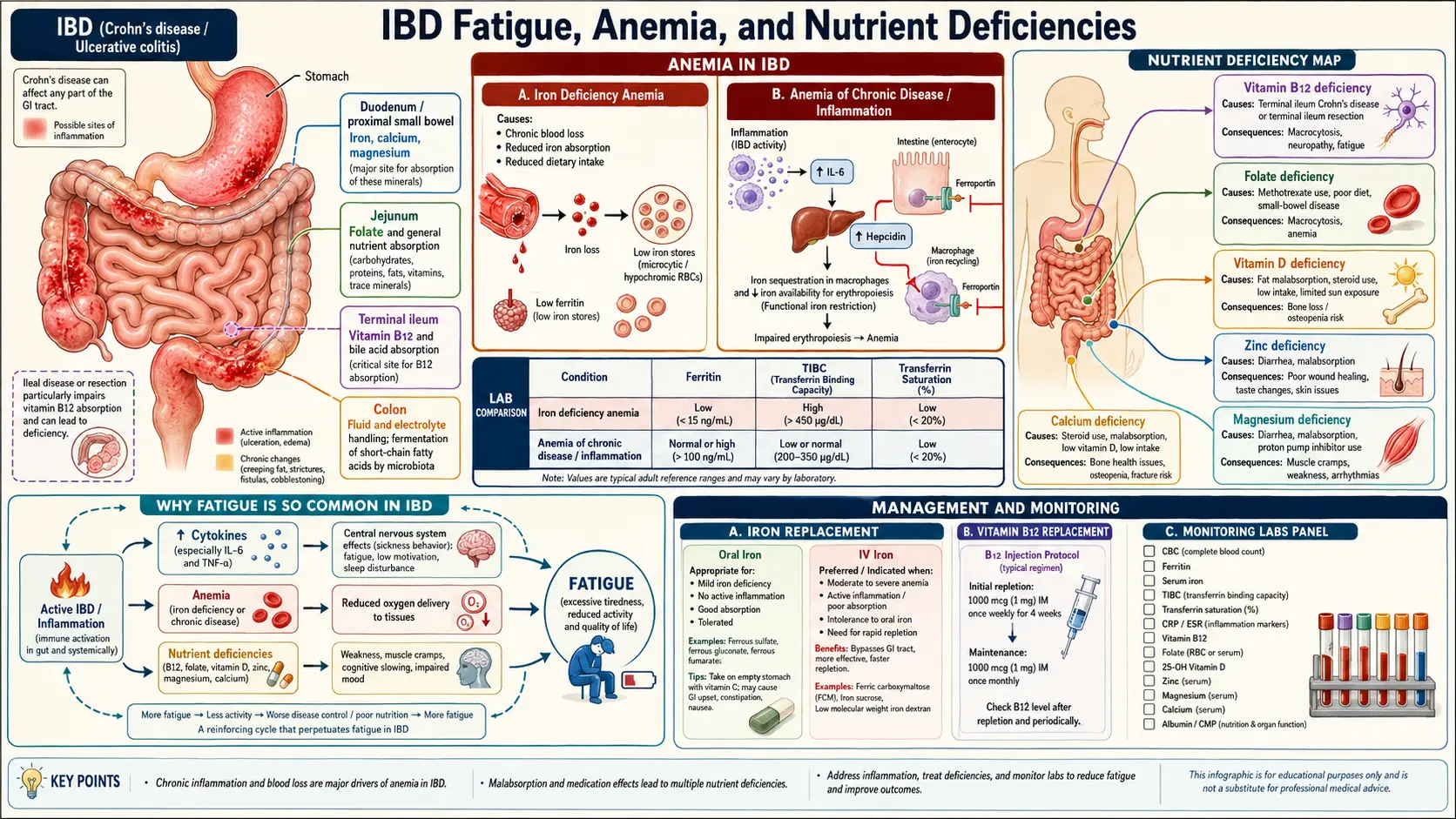
Table of Contents
- Why Fatigue Persists Even in Remission
- Iron Deficiency Anemia — the Most Common IBD Deficiency
- Ferritin in Inflammation — Why <100 Matters in IBD
- Oral Iron vs IV Iron — When to Switch
- Vitamin B12 and Folate
- Vitamin D Deficiency
- Calcium and Bone Density
- Zinc — Especially in Crohn's with Diarrhea
- Magnesium
- Protein-Calorie Undernutrition
- Sleep Disruption
- Anxiety, Depression, and the Fatigue Overlap
- When to Test for Thyroid Disease or Celiac
- Evidence-Based Supplements vs Hype
- A Practical Lab-Monitoring Schedule
- Key Research Papers
- Connections
- Featured Videos
Why Fatigue Persists Even in Remission
The cruelest surprise of inflammatory bowel disease is that the bathroom chaos can settle down — calprotectin normal, colonoscopy clean, biologic doing its job — and you are still wrecked by fatigue. In large patient surveys, roughly 40–50% of people in clinical and endoscopic remission still report significant fatigue. This is not laziness, not depression masquerading as something else, and not a sign your medication is failing. It is a real, measurable biological state with several overlapping causes.
The main drivers, in rough order of how often they turn out to be fixable:
- Iron deficiency — frequently present even when hemoglobin is technically "normal." Low iron stores sap energy long before red-cell counts drop.
- Vitamin D deficiency — almost universal in IBD, contributes to muscle fatigue and low mood.
- B12 or folate deficiency — especially after terminal ileum resection or with methotrexate use.
- Subclinical inflammation — low-grade cytokine activity (IL-6, TNF-alpha) directly produces "sickness behavior" in the brain: tiredness, brain fog, low motivation.
- Disrupted sleep — nocturnal bowel movements, urgency anxiety, pain, or steroid-induced insomnia.
- Psychological load — the chronic vigilance of living with IBD is exhausting even when nothing flares.
- Coexisting conditions — thyroid disease, celiac, sleep apnea, depression.
Fatigue deserves the same workup as a new flare. Ask your GI team for a "fatigue panel," and if they do not run one, ask your primary care doctor. The list below is the one to hand them.
Iron Deficiency Anemia — the Most Common IBD Deficiency
Iron deficiency is the single most common extraintestinal problem in IBD. Depending on the cohort, 36–76% of IBD patients have iron deficiency, and roughly a third meet criteria for frank anemia at some point in their disease. It happens for three reasons stacked on top of each other:
- Chronic blood loss from inflamed gut mucosa — sometimes visible (UC rectal bleeding), sometimes silent (Crohn's small-bowel oozing).
- Impaired absorption — iron is absorbed in the duodenum and upper jejunum, and inflammation upstream or gastric acid suppression (PPIs) blunts uptake.
- Inflammation blocks iron use — hepcidin, a hormone made by the liver during inflammation, locks iron inside storage cells and prevents it from being released to make red cells. This is the "anemia of chronic disease" piece, and it is why iron studies in IBD look weird.
Symptoms to notice before labs confirm it: exertional breathlessness, cold hands and feet, brittle or spoon-shaped nails, restless legs at night, pica (craving ice or starch), hair shedding, and the deep "I slept nine hours and still feel hungover" fatigue. You can have every one of these with a hemoglobin that still reads in the low-normal range.
See also the dedicated mineral page on iron.
Ferritin in Inflammation — Why <100 Matters in IBD
In a healthy adult, a serum ferritin below 30 ng/mL diagnoses iron deficiency. In IBD, that cutoff is wrong and will miss most cases. Ferritin is an acute-phase reactant: when the body is inflamed, the liver pumps out ferritin regardless of whether stores are actually full. A ferritin of 60 in someone with active colitis can mask genuinely empty stores.
European Crohn's and Colitis Organisation (ECCO) and AGA guidelines therefore use context-specific cutoffs:
- No clinical or biochemical inflammation: iron deficiency = ferritin < 30 ng/mL.
- Active IBD or CRP elevated: iron deficiency = ferritin < 100 ng/mL or transferrin saturation < 20%.
The full iron workup your doctor should order: ferritin, serum iron, total iron binding capacity (TIBC), transferrin saturation (Tsat), complete blood count with indices (MCV, MCH), reticulocyte count, and CRP. Soluble transferrin receptor (sTfR) is an option when the picture is unclear because it is not affected by inflammation, though it is not available at every lab.
If your ferritin report comes back in the 40–90 range and your doctor says "normal," push back politely. Quote the 100 ng/mL cutoff for IBD with inflammation. It is written into mainstream guidelines.
Oral Iron vs IV Iron — When to Switch
Oral iron (ferrous sulfate, ferrous gluconate, ferrous bisglycinate) is cheap and available over the counter. It works for mild iron deficiency when the gut is not actively inflamed. But in IBD it fails often enough that ECCO guidelines recommend IV iron as first-line in several common situations:
- Active IBD (inflammation upregulates hepcidin, which blocks oral absorption).
- Hemoglobin < 10 g/dL.
- Intolerance or failed response to oral iron.
- Need for rapid correction (before surgery, during pregnancy, ahead of biologic initiation).
- Concurrent erythropoietin therapy.
Oral iron also has a reputation for worsening IBD symptoms — unabsorbed iron reaches the colon and may feed inflammation and alter the microbiome. Whether this matters clinically is debated, but it is another reason many IBD specialists prefer IV.
Modern IV iron preparations have made the therapy fast, safe, and office-based. The two dominant options:
- Ferric carboxymaltose (Injectafer, Ferinject) — up to 750–1000 mg in a single 15-minute infusion. Two infusions a week apart usually fully replete stores. Main watch-outs: transient hypophosphatemia (often asymptomatic, sometimes causing fatigue and bone pain of its own), and a $1,000–$1,500 per-dose U.S. list price that insurance usually covers.
- Ferric derisomaltose (Monoferric) — up to 1000–1500 mg in a single 20-minute infusion. Lower hypophosphatemia risk than ferric carboxymaltose in head-to-head trials.
- Iron sucrose (Venofer) and ferric gluconate (Ferrlecit) — older, cheaper, but require multiple visits (200 mg per session, 5–10 sessions).
Expect a gradual lift in energy over 2–4 weeks after repletion, with peak benefit at 6–8 weeks. Hemoglobin typically rises 1–2 g/dL per month. Recheck ferritin and Tsat at 8–12 weeks.
If oral iron is worth trying first, the tolerability trick is alternate-day dosing. A 2017 study showed that taking iron every other day actually absorbs more total iron than daily dosing, because daily doses spike hepcidin and block the next day's absorption. Take 60–120 mg elemental iron every other morning, on an empty stomach with vitamin C (a glass of orange juice or 250 mg ascorbate), and avoid calcium, coffee, and tea for two hours on either side.
Vitamin B12 and Folate
Vitamin B12 is absorbed almost exclusively in the terminal ileum, the exact segment that Crohn's disease loves to inflame and that surgeons often resect. The risk curve is steep:
- Terminal ileum resection under 20 cm — most patients still absorb enough B12, but check annually.
- Resection 20–60 cm — deficiency is likely within a few years; lifelong supplementation is usually needed.
- Resection over 60 cm, or total ileal loss — B12 deficiency is essentially certain without replacement.
- Active terminal ileitis without resection — still a risk factor; check yearly.
Replacement options: intramuscular cyanocobalamin or hydroxocobalamin 1000 mcg weekly for a month then monthly, or high-dose oral/sublingual cyanocobalamin 1000–2000 mcg daily (around 1% is absorbed by passive diffusion even without intrinsic factor, which is usually enough). IM is traditional; oral works for most people if you take it reliably. Nasal sprays exist but are more expensive with thinner evidence.
Watch for symptoms that appear before the lab value tanks: tingling or numbness in feet, balance problems, tongue soreness, memory slips, irritability, and the classic megaloblastic anemia picture of large red cells (MCV > 100). Serum B12 can be misleading; if it sits in the gray zone (200–400 pg/mL), ask for methylmalonic acid (MMA) and homocysteine, both of which rise in true tissue deficiency before the serum B12 drops.
Folate deficiency is less common but real, especially if you are on methotrexate (which blocks folate metabolism) or sulfasalazine (which impairs folate absorption). Standard replacement is 1–5 mg daily. Never replace B12 deficiency with folate alone — folate will correct the anemia on labs while the neurological damage of B12 deficiency silently progresses.
See the full page on vitamin B12.
Vitamin D Deficiency
Somewhere between 60% and 80% of people with IBD are vitamin D deficient or insufficient. Active Crohn's disease of the small bowel reduces absorption of fat-soluble vitamins, steroid use accelerates bone loss, and many IBD patients avoid sunlight because of biologic-associated skin-cancer concerns or are simply too tired to go outside.
Measure 25-hydroxyvitamin D (25(OH)D), not 1,25-dihydroxyvitamin D. Target ranges:
- Deficient: < 20 ng/mL (50 nmol/L) — high-dose repletion indicated.
- Insufficient: 20–30 ng/mL — supplementation recommended.
- IBD target: many GIs aim for 40–60 ng/mL based on small trials showing lower flare rates at the upper end of normal.
Standard replacement: vitamin D3 (cholecalciferol) 2000–5000 IU daily for maintenance, or 50,000 IU weekly for 8–12 weeks for deficiency, then retest. Take with a meal containing fat — vitamin D absorption is roughly 30% higher with dietary fat. If absorption is severely impaired, switch to sublingual or liquid preparations.
See the full page on vitamin D.
Calcium and Bone Density
IBD patients have elevated fracture risk for several stacking reasons: steroid courses (cumulative prednisone dose matters), chronic inflammation, low vitamin D, reduced calcium absorption in small-bowel Crohn's, and dairy avoidance because of lactose intolerance. Up to 50% of IBD patients have osteopenia and 10–30% have osteoporosis on DXA.
Practical steps:
- DXA bone-density scan at diagnosis if there are risk factors, and every 1–3 years if abnormal or if you have had cumulative steroid exposure of more than 3 months.
- Calcium intake 1000–1200 mg/day from food when possible (dairy, fortified plant milks, sardines with bones, leafy greens). Supplement only if dietary intake is clearly inadequate — calcium supplements have a modest association with cardiovascular events when used at high doses.
- Vitamin D adequacy first (see above) — calcium does little if D is low.
- Weight-bearing exercise, smoking cessation, limited alcohol.
- Bisphosphonates if T-score drops into the osteoporosis range or after fragility fracture; gastroenterology coordination is needed because oral bisphosphonates can irritate GI mucosa — IV zoledronate is often preferred in IBD.
Zinc — Especially in Crohn's with Diarrhea
Zinc is lost in diarrheal fluid. Crohn's patients with high-output ileostomies, chronic loose stools, or jejunoileal disease are the highest-risk group. Deficiency shows up as hair loss, slow wound healing, skin rashes at the corners of the mouth or around body orifices (acrodermatitis enteropathica-like), loss of taste and smell, impaired immunity, and male hypogonadism.
Serum zinc is a rough test — it is also an acute-phase reactant and drops in inflammation independent of stores. If clinical signs are present, trial replacement is reasonable. Typical dose: zinc gluconate or zinc picolinate 15–30 mg daily with food. Do not exceed 40 mg daily long-term — high-dose zinc chronically suppresses copper absorption and can cause a second deficiency that looks like myelopathy. If you need more than 40 mg daily for more than a few weeks, add 1–2 mg of copper.
Magnesium
Magnesium is absorbed throughout the small intestine and to some degree the colon, and like zinc it is lost in diarrheal fluid. Proton pump inhibitors (frequently prescribed to IBD patients) also deplete magnesium over years of use. Symptoms: muscle cramps (especially at night), eyelid twitching, palpitations, migraine, constipation when oral intake is low, and poor sleep.
Serum magnesium misses most deficiency because only about 1% of body magnesium is in blood. RBC magnesium or ionized magnesium is more sensitive, though less commonly offered. A practical approach: if you have suggestive symptoms and no contraindications, trial magnesium glycinate or magnesium malate 200–400 mg at bedtime for 4–6 weeks. Magnesium citrate works but tends to loosen stools — a bug, not a feature, in IBD. Magnesium oxide is poorly absorbed and not worth buying.
See the full page on magnesium.
Protein-Calorie Undernutrition
Not every IBD patient is underweight — many are normal or even overweight thanks to steroids and inactivity — but sarcopenia (low muscle mass) is common at every body weight. Lean-mass loss correlates with worse surgical outcomes, more post-op complications, higher flare rates, and more fatigue. Causes include inflammation-driven protein breakdown, inadequate intake during flares, small-bowel malabsorption, and protein-losing enteropathy through inflamed mucosa.
Targets in IBD:
- Calories: 25–30 kcal/kg/day in remission; up to 35–40 kcal/kg/day during flares or after surgery.
- Protein: 1.0–1.2 g/kg/day in remission, 1.2–1.5 g/kg/day in active disease or post-op. Split across 3–4 meals so every meal has at least 25–30 g of protein.
- Oral nutrition supplements (ONS) — polymeric shakes like Ensure, Boost, Kate Farms, Orgain — are a reasonable bridge when food intake is low. Partial enteral nutrition (replacing 35–50% of calories with a formula) has trial evidence in Crohn's maintenance.
A registered dietitian with IBD experience is the single best investment if weight or muscle mass is an issue. Most IBD centers have one on staff; ask for a referral.
Sleep Disruption
Sleep and IBD fatigue feed each other. Active disease wakes you up to use the bathroom. Even in remission, nocturnal urgency anxiety ("will I make it?") disrupts sleep architecture. Steroids cause insomnia, especially prednisone doses above 20 mg. Pain from fissures, abscesses, or joint involvement keeps you from deep sleep. And restless legs from iron deficiency is its own sleep destroyer.
What actually helps, in rough order of payoff:
- Treat iron deficiency and vitamin D aggressively — restless legs often resolves.
- If on steroids, take the full dose in the morning.
- Consistent sleep-wake times, even on weekends.
- Screen for obstructive sleep apnea if you snore, wake gasping, or feel unrefreshed regardless of hours slept — OSA is more common in IBD than in the general population.
- Cognitive behavioral therapy for insomnia (CBT-I) — outperforms sleep medications long-term; available as apps (Somryst, Sleepio) and online programs.
- Avoid alcohol within 3 hours of bed — it fragments sleep even when it helps you fall asleep.
Anxiety, Depression, and the Fatigue Overlap
Roughly one in three IBD patients meets criteria for an anxiety or depressive disorder at any given time — two to three times the general-population rate. This is not a character weakness. The brain-gut-immune axis is bidirectional: inflammation directly produces depressive symptoms through cytokine signaling to the central nervous system, and chronic illness with unpredictable flares generates legitimate anxiety.
Depression and fatigue overlap enormously. Low energy, poor concentration, anhedonia, and sleep changes are core features of both. You do not need to decide which one is "really" the problem — treat both. Evidence-based options:
- CBT adapted for IBD — reduces fatigue scores in trials even without changing disease activity.
- Gut-directed hypnotherapy — good evidence in functional overlay; IBD-specific trials are smaller but positive.
- SSRIs/SNRIs — sertraline, escitalopram, duloxetine are common first-line choices; duloxetine has analgesic properties that help overlap pain.
- Low-dose tricyclics (amitriptyline 10–25 mg at night) — help pain, sleep, and mood simultaneously; watch constipation in UC.
- Exercise — moderate-intensity activity 150 min/week is as effective as SSRIs for mild-to-moderate depression in several meta-analyses.
If your IBD team does not have a psychologist on staff, a GI psychologist can be found through the Rome Foundation's directory or the Crohn's & Colitis Foundation's provider finder.
When to Test for Thyroid Disease or Celiac
Two co-travelers with autoimmune IBD deserve a low threshold for testing when fatigue dominates:
Thyroid disease. Autoimmune thyroid disease (Hashimoto's, Graves') clusters with IBD. Check TSH, free T4, and anti-TPO antibodies if you have unexplained fatigue, weight change, temperature intolerance, dry skin, hair shedding, or menstrual changes. TSH alone is a reasonable screen in someone with no symptoms; add free T4 and antibodies if clinical suspicion is present.
Celiac disease. The prevalence of celiac in IBD is debated (some studies show it's similar to the general population, others suggest modestly increased). More importantly, the symptoms overlap heavily — diarrhea, fatigue, iron deficiency, B12 deficiency, low vitamin D — and iron deficiency that does not respond to repletion is a celiac red flag. Check tissue transglutaminase IgA (tTG-IgA) with total IgA while still on a gluten-containing diet. If positive, duodenal biopsy confirms. See the dedicated page on celiac disease.
Other worth-considering workup items for treatment-resistant fatigue: HbA1c (steroid-induced diabetes), testosterone in men (low in chronic illness), morning cortisol (adrenal insufficiency from recent steroid tapering), and sleep study if snoring or witnessed apnea.
Evidence-Based Supplements vs Hype
The IBD supplement market is a jungle. Here is a reasonable triage:
Worth trying (decent evidence, low risk):
- Iron — when deficient. IV if oral fails or disease is active.
- Vitamin D3 — target 40–60 ng/mL.
- Vitamin B12 — when deficient or after ileal resection.
- Omega-3 fish oil — trial evidence in IBD is mixed for flare prevention but supports cardiovascular health and mood.
- Curcumin — modest trial evidence as adjunct in UC at 2–3 g/day of standardized extract (BCM-95, Theracurmin); not a substitute for mainstream therapy.
- Psyllium (soluble fiber) — useful in UC remission for stool form; avoid in active Crohn's with strictures.
- Specific probiotics — E. coli Nissle 1917 has UC maintenance data; VSL#3/Visbiome has pouchitis data. Most other strains lack IBD-specific evidence.
Worth considering case-by-case:
- Zinc — if diarrhea is chronic or deficiency is documented.
- Magnesium — for cramps, migraine, sleep, or PPI-related depletion.
- Folate — mandatory if on methotrexate; otherwise only if deficient.
- Vitamin K — if small-bowel disease is extensive and PT/INR is elevated.
Hype — skip unless your doctor specifically recommends:
- Glutamine for "gut healing" — trials are negative or tiny in IBD.
- Colostrum, deer antler, sea moss, celery juice, etc. — no evidence.
- Aggressive mega-dose multivitamins — targeted repletion based on labs is always better.
- High-dose turmeric with black pepper extract (piperine) — piperine inhibits liver enzymes that metabolize tacrolimus, cyclosporine, and some other IBD drugs; choose a non-piperine formulation if you are on those.
A Practical Lab-Monitoring Schedule
Copy this into your notes app and ask your GI team to schedule it. Exact timing is judgment; this is a reasonable default.
- Every 3 months in active disease; every 6–12 months in remission: CBC, CRP, albumin, fecal calprotectin, iron studies (ferritin, Tsat), vitamin D, B12 (annually or if deficient), folate (if on methotrexate/sulfasalazine or deficient).
- Annually: Full metabolic panel, magnesium, TSH, HbA1c if steroid history.
- At diagnosis and every 1–3 years if risk factors: DXA bone density.
- Case-by-case: zinc if diarrhea; copper if chronic high-dose zinc; methylmalonic acid and homocysteine if B12 is borderline; tTG-IgA for celiac.
You are entitled to your lab values — not a phone call from a nurse saying "everything is fine." Ask the patient portal or records department to release them. Track ferritin, vitamin D, and B12 over time. Trend is more informative than any single number.
Key Research Papers
- Dignass AU, et al. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel diseases. J Crohns Colitis. 2015.
- Bischoff SC, et al. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease. Clin Nutr. 2023.
- Moum B, Ekbom A, et al. Fatigue in patients with inflammatory bowel disease: systematic review. Aliment Pharmacol Ther. 2015.
- Stoffel NU, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days. Lancet Haematol. 2017.
- Gisbert JP, Gomollón F. Common misconceptions in the diagnosis and management of anemia in inflammatory bowel disease. Am J Gastroenterol. 2008.
- Jones JL, et al. The impact of inflammatory bowel disease on patients' lives — an analysis of fatigue. Aliment Pharmacol Ther. 2018.
- Weisshof R, Chermesh I. Micronutrient deficiencies in inflammatory bowel disease. Nutrients. 2019.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on fatigue, anemia, and nutrient deficiencies in IBD:
- IBD and fatigue
- Iron deficiency anemia in IBD
- Ferric carboxymaltose in IBD
- Ferric derisomaltose and iron deficiency
- Vitamin B12 and ileal resection in Crohn's disease
- Vitamin D in IBD
- Bone density and osteoporosis in IBD
- Zinc deficiency in Crohn's disease
- Magnesium deficiency in IBD
- Sarcopenia in IBD
- Depression and anxiety in IBD
- Celiac disease and IBD overlap
Connections
- Inflammatory Bowel Disease Overview
- Crohn's vs Ulcerative Colitis: Key Differences
- Diagnostic Workup: Calprotectin, Colonoscopy, MRE
- Biologics: TNF, IL-23, and Integrin Inhibitors
- Diet for IBD: SCD and Mediterranean
- IBD Surgery Decisions
- Extraintestinal Manifestations: Joints, Skin, Eyes
- Pregnancy and IBD
- JAK Inhibitors and S1P Modulators
- Crohn's Disease
- Celiac Disease
- Iron
- Vitamin B12
- Vitamin D3
- Magnesium
- Zinc
- Anemia
- Vitamin B12 Lab Test