IBD Surgery Decisions — Resection, J-Pouch, and Ostomy
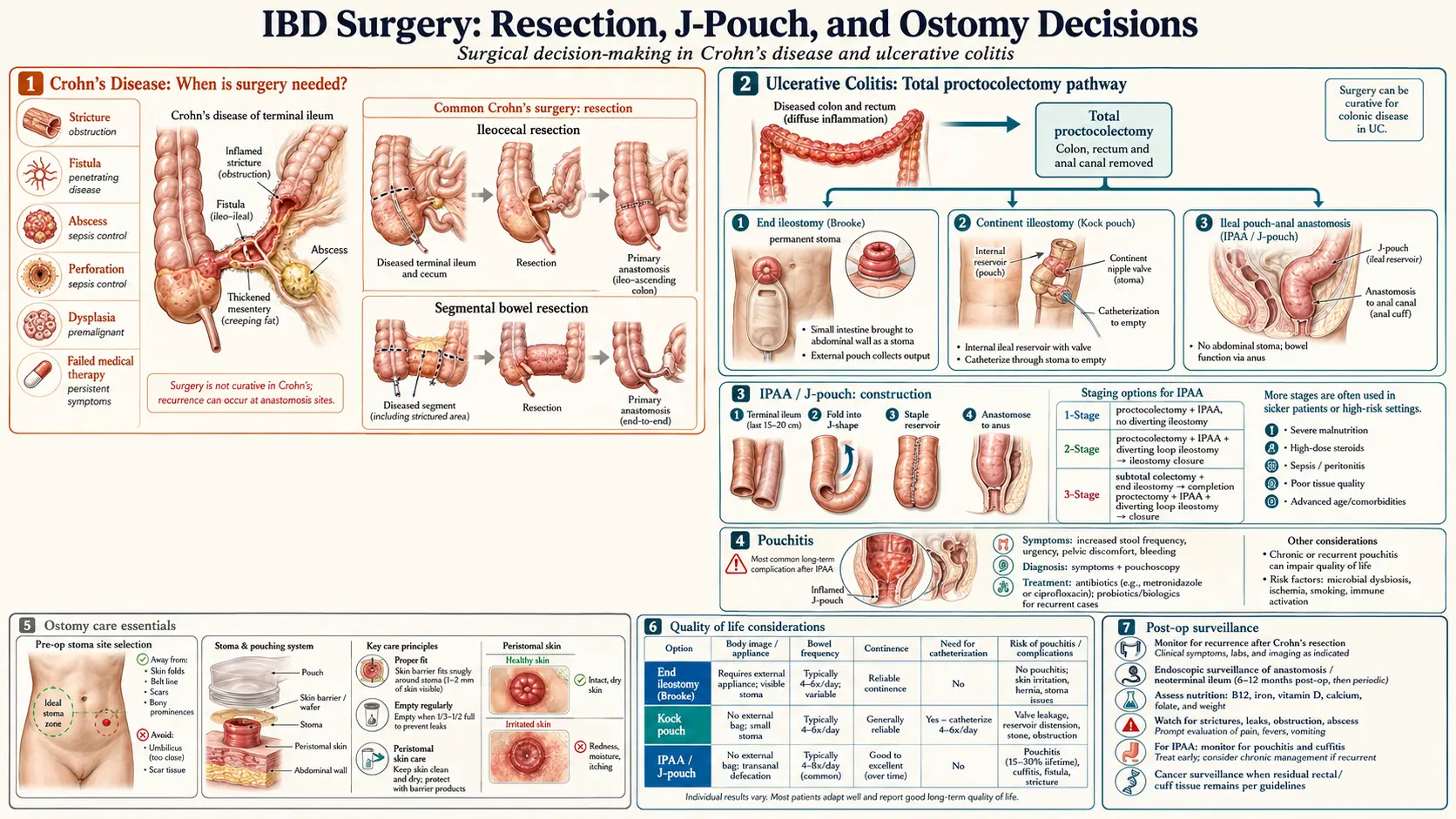
Table of Contents
- When Surgery Beats Another Biologic
- Crohn's: Ileocecal Resection and the LIR!C Trial
- Stricturoplasty — Saving Bowel Length
- Fistula Surgery in Crohn's
- Post-Op Prophylaxis and the Rutgeerts Score
- UC: Subtotal Colectomy — Emergency vs Elective
- The J-Pouch (IPAA) — 2-Stage vs 3-Stage
- Pouchitis, Cuffitis, and Pouch Failure
- Fertility, Pregnancy, and Sexual Function
- The Kock Pouch — A Historical Alternative
- Life with a Permanent Ileostomy
- Supplies, Appliance Brands, and Insurance
- Choosing a Surgeon — Volume Matters
- Post-Op Diet — First Weeks and Beyond
- Key Research Papers
- Connections
- Featured Videos
When Surgery Beats Another Biologic
Surgery in IBD is no longer a last resort. Thirty years ago it carried that reputation because the only patients who reached an operating room were the ones whose disease had already wrecked their bodies — perforation, obstruction, sepsis, cancer. Today the calculus is different. For the right patient, an operation done early is faster, safer, and often cheaper than cycling through a third or fourth biologic while losing weight, missing work, and watching a stricture slowly close.
Four scenarios tip the balance toward surgery:
- Short-segment Crohn's at the ileocecal valve that responds poorly to medication. The LIR!C trial changed practice here.
- Fibrotic (non-inflammatory) strictures. A scar is not going to be fixed by a TNF inhibitor. MRE or CT with careful reading can tell you whether the wall is inflamed or fibrosed — fibrosis points straight to surgery or endoscopic dilation.
- UC with steroid dependence after two or more biologic classes have failed, especially in a patient who is chronically anemic, underweight, or unable to work.
- Dysplasia on surveillance colonoscopy in long-standing colitis. High-grade dysplasia is a colectomy indication, full stop.
The question patients rarely get asked directly is: what do you want the next year of your life to look like? A well-performed surgery at a high-volume center can close the door on years of inflammation in a single admission. A new biologic started today will tell you in 12–16 weeks whether it worked. If it didn't, you are another four months older, still sick, and down another insurance-authorized option.
Crohn's: Ileocecal Resection and the LIR!C Trial
The terminal ileum and cecum are the single most common location for Crohn's disease. An ileocecal resection removes the last few inches of small bowel and the cecum, then connects (anastomoses) the healthy small bowel to the ascending colon. Done laparoscopically at an experienced center, the hospital stay is 3–5 days and most patients are back to light activity in two weeks.
The landmark LIR!C trial (Ponsioen et al., published in Lancet Gastroenterology & Hepatology in 2017, with long-term follow-up in 2020) randomized 143 patients with limited ileocecal Crohn's — failing conventional therapy but not yet on biologics — to either laparoscopic ileocecal resection or infliximab. At one year, quality-of-life scores were equivalent. At five-year follow-up, surgery patients reported equal or better outcomes, with 42% of the infliximab group eventually needing surgery anyway. Cost analysis favored the surgical arm.
The takeaway is not that every ileocecal Crohn's patient should have surgery. It is that, for short-segment disease, surgery is a reasonable first-line option rather than a rescue maneuver, and deferring it in favor of biologics does not reliably prevent the operation — it often just delays it.
Stricturoplasty — Saving Bowel Length
Patients with multifocal small-bowel Crohn's can accumulate several strictures over years. Resecting each one would eventually shorten the bowel enough to cause short bowel syndrome — chronic diarrhea, malabsorption, and dependence on intravenous nutrition. Stricturoplasty is the length-sparing alternative: the surgeon opens the narrowed segment longitudinally and sews it closed transversely, widening the lumen without removing tissue.
The two common techniques are the Heineke-Mikulicz (for short strictures under 10 cm) and the Finney or side-to-side isoperistaltic (for long strictures). Recurrence at a stricturoplasty site is no higher than at a resection anastomosis, and preserved bowel length is the payoff. A patient with five small-bowel strictures may leave the operating room with all five widened and every centimeter of intestine intact.
Fistula Surgery in Crohn's
Perianal fistulas affect roughly 25% of Crohn's patients over their lifetime, and they are miserable: constant drainage, recurrent abscesses, pain with sitting, and a sharp hit to body image and sexual function. Surgery for fistulas in Crohn's is deliberately conservative, because aggressive cutting in an inflamed anal sphincter risks incontinence the patient will live with forever.
- Exam under anesthesia (EUA) with MRI mapping is usually the first step — defining tracks, identifying abscesses, and often placing a seton (a soft silicone loop) through each fistula tract to keep it draining while medications work.
- Seton drainage + biologic therapy (infliximab is best studied) is the mainstay. The seton prevents abscess; the biologic reduces inflammation and allows some tracts to close.
- Fistulotomy (laying open the tract) is reserved for low, simple fistulas not crossing significant sphincter muscle.
- Advancement flap and LIFT procedure (ligation of the intersphincteric fistula tract) are sphincter-sparing options for complex disease.
- Mesenchymal stem-cell therapy (darvadstrocel / Alofisel) is approved in Europe and selected U.S. centers for complex refractory perianal Crohn's fistulas.
Post-Op Prophylaxis and the Rutgeerts Score
Here is the brutal truth about Crohn's surgery: the disease comes back. Endoscopic recurrence — visible inflammation at the anastomosis — appears in 70–90% of patients within one year if no medication is given afterward. Clinical symptoms follow later, and surgical recurrence (another operation) happens in 25–35% at ten years.
Why? The honest answer is that no one fully knows. The favored theory is that stool exposure triggers the immune reaction that drives Crohn's, and the neoterminal ileum — the new end of small bowel sitting just upstream of the anastomosis — is suddenly bathed in colonic contents it wasn't designed to handle. Bile acids, bacterial load, and oxygen gradients all change at that junction.
The Rutgeerts score, developed by Paul Rutgeerts in 1990, grades endoscopic recurrence at colonoscopy performed 6–12 months post-op:
- i0 — no lesions. Prognosis excellent.
- i1 — fewer than five aphthous ulcers. Still good.
- i2 — more than five aphthous ulcers, or skip lesions. Watch closely.
- i3 — diffuse aphthous ileitis with inflamed mucosa. Escalate therapy.
- i4 — diffuse inflammation with larger ulcers, nodules, or narrowing. High risk of clinical recurrence.
The modern approach: start post-op prophylaxis within 4–8 weeks of surgery in anyone with risk factors (smoking, prior resection, penetrating disease, active inflammation at the margin, young age at diagnosis). Most guidelines now recommend an anti-TNF agent as prophylaxis for high-risk patients, confirmed with colonoscopy at 6–12 months to catch recurrence early. Smokers: quitting after surgery cuts recurrence risk roughly in half. If you were ever going to quit, this is the moment.
UC: Subtotal Colectomy — Emergency vs Elective
Because ulcerative colitis is confined to the colon, removing the colon is curative for the intestinal disease. That fact drives every UC surgical decision. The two paths into the operating room are very different.
Emergency colectomy means acute severe UC that is failing rescue therapy (intravenous steroids, then infliximab or cyclosporine) — or worse, toxic megacolon or perforation. The operation is a subtotal colectomy with end ileostomy: the colon comes out, the rectum is stapled closed and left in place (the “Hartmann stump”), and the small bowel is brought to the skin as a temporary stoma. The patient recovers, builds nutrition back up, and returns months later for the next stage. Doing more than this during an emergency is unsafe — the inflamed rectum cannot hold an anastomosis.
Elective colectomy is scheduled, usually for medication-refractory chronic disease or dysplasia. It can still begin with a subtotal colectomy, but in a healthy patient at a high-volume center, the surgeon and patient may go directly to a one- or two-stage reconstruction.
The J-Pouch (IPAA) — 2-Stage vs 3-Stage
The ileal pouch-anal anastomosis (IPAA), almost always shaped like the letter J, is the modern reconstruction of choice after colectomy for UC. The surgeon folds the last 30–40 cm of small bowel back on itself, staples it into a pouch that serves as a neorectum, and connects the bottom of the pouch to the anal canal. The patient keeps bowel continuity and sits on the toilet like anyone else — just more often.
Two staging strategies dominate:
- 2-stage IPAA. Stage 1: total proctocolectomy + J-pouch + diverting loop ileostomy (so the new pouch heals with no stool passing through it). Stage 2, about 8–12 weeks later: reverse the loop ileostomy. Used in healthy elective patients.
- 3-stage IPAA. Stage 1: subtotal colectomy + end ileostomy (the emergency or very-sick scenario). Stage 2, 3–6 months later when the patient is off steroids and nutritionally stable: completion proctectomy + J-pouch + diverting loop ileostomy. Stage 3, another 8–12 weeks later: ileostomy reversal.
Expect 4–8 bowel movements per day with a mature pouch, sometimes one at night. Most patients describe life a year after the final stage as “completely different — I'm a person again.” Continence is preserved in the large majority. The trade-off is that the pouch is not a normal colon and it has its own set of complications, discussed next.
Pouchitis, Cuffitis, and Pouch Failure
Pouchitis is inflammation of the J-pouch mucosa — the most common long-term complication, affecting roughly 50% of IPAA patients at least once within five years. Symptoms: increased stool frequency, urgency, cramping, sometimes blood and low-grade fever. First-line treatment is a two-week course of ciprofloxacin or metronidazole, which works in over 80% of acute episodes. Chronic or antibiotic-refractory pouchitis may respond to vedolizumab (the EARNEST trial, 2023), budesonide, or biologic therapy used for IBD.
Cuffitis is inflammation of the short strip of residual rectal mucosa (the “cuff”) left when the pouch is stapled rather than hand-sewn. It acts like a tiny patch of persistent UC and responds to topical mesalamine or hydrocortisone suppositories.
Pouch failure — pouch excision or permanent diversion — occurs in 5–10% of patients at 10 years. The most common causes are Crohn's disease discovered after colectomy (the pathology changed the diagnosis), refractory pouchitis, and pelvic sepsis from anastomotic leak. A failed pouch does not mean a failed life: conversion to permanent ileostomy is straightforward, and most patients feel better afterward than during the years of pouch trouble.
Fertility, Pregnancy, and Sexual Function
For women of reproductive age, IPAA has one documented cost: infertility roughly triples compared with the same woman before surgery. The mechanism is pelvic adhesions around the fallopian tubes, not hormonal or ovarian. The spontaneous-conception rate is around 20% at 12 months of trying, versus 50–60% in age-matched controls. IVF bypasses the problem completely; outcomes with IVF are equivalent to the general population.
Two strategies can reduce this risk:
- Laparoscopic or robotic IPAA creates fewer adhesions than open surgery. Choose a high-volume minimally invasive surgeon.
- Delayed reconstruction. Some women with severe UC take the subtotal colectomy first, keep the end ileostomy, complete their family, and then have the J-pouch created afterward. This is a real and reasonable plan — discuss it openly with the colorectal surgeon and a reproductive endocrinologist before the first operation.
Sexual function: most men have unchanged erectile and ejaculatory function after J-pouch surgery; retrograde ejaculation occurs in a small minority, usually from nerve irritation that recovers over months. Women may have dyspareunia from pelvic scarring. Both are far more likely with open surgery than with minimally invasive technique.
The Kock Pouch — A Historical Alternative
Before the J-pouch became standard in the 1980s, Swedish surgeon Nils Kock developed the continent ileostomy (“Kock pouch”) in 1969. A reservoir of small bowel is built inside the abdomen with a nipple-valve leading to a flush stoma on the skin. Instead of wearing an external bag, the patient intubates the stoma with a catheter several times a day to empty the pouch.
Kock pouches are now performed at only a few specialized centers (Cleveland Clinic, Mayo, a handful of others). Indications are narrow: the J-pouch failed or is not an option, but the patient refuses a traditional external appliance. Long-term complications — valve slippage, difficulty catheterizing, pouchitis — are common enough that most surgeons steer patients toward an end ileostomy instead. It is worth knowing the Kock pouch exists; it is rarely the right answer in 2026.
Life with a Permanent Ileostomy
A permanent ileostomy is not a failure. For many patients with extensive Crohn's of the colon, poor anal sphincter function, pelvic radiation history, or recurrent pouch failure, it is the operation that gives back the most life. Surveys repeatedly show post-ileostomy quality-of-life scores that exceed matched pre-operative IBD scores. The reason is simple: the disease is over. Urgency is over. The 3 a.m. sprints to the bathroom are over. You plan your day around ordinary things again.
Practical realities worth knowing:
- Output: 600–1200 mL of liquid-to-porridge stool per day. You empty the pouch 4–8 times daily.
- Diet: most people eat a near-normal diet within three months. High-fiber raw foods (corn, nuts, mushrooms, celery) can occasionally block the stoma — chew well.
- Hydration: the colon normally reabsorbs a liter of water a day; without it, you must drink more and watch sodium. Oral rehydration solution helps during heat, exercise, or high output.
- Activity: swimming, weightlifting, running, sex — all routine with a stoma. Contact sports use a stoma guard.
- Appearance: modern low-profile flat appliances are invisible under most clothing. The stigma in patients' heads is almost always worse than the reality in strangers' eyes.
- Body image and mental health: the first 3–6 months are hard. Ostomy support groups (United Ostomy Associations of America; local Facebook groups) are genuinely helpful. Consider a few sessions with a therapist who specializes in chronic illness.
Supplies, Appliance Brands, and Insurance
Three companies dominate the U.S. ostomy appliance market, each with one-piece and two-piece systems, cut-to-fit and pre-cut wafers, and drainable or closed pouches:
- Hollister — New Image two-piece is the most widely prescribed starter system.
- Coloplast — SenSura Mio has a flexible wafer popular with active patients.
- ConvaTec — Esteem and Natura lines; strong convex wafers for flush or retracted stomas.
Try several. What works for one stoma shape, skin, and lifestyle is wrong for another. Manufacturers send free sample kits on request — take advantage of this in the first three months before committing to a supplier.
Insurance tactics. Medicare covers ostomy supplies as durable medical equipment (HCPCS codes A4375–A4434). Private insurance usually follows, but watch for monthly quantity caps — a reasonable baseline is 20 pouches and 10 wafers per month; document higher use in writing if your output requires it. Mail-order suppliers (Edgepark, Byram Healthcare, 180 Medical) usually charge less than pharmacy pickup and will handle insurance billing directly. A WOC nurse (Wound, Ostomy, and Continence certified) at your hospital is worth her weight in gold — ask for one in pre-op, again in-hospital, and for follow-up visits. Many insurers pay for at least two outpatient WOC visits.
Choosing a Surgeon — Volume Matters
This is the single most under-discussed variable in IBD surgery outcomes. Study after study shows that high-volume surgeons and high-volume centers have lower complication rates, lower mortality, shorter hospital stays, and fewer re-operations for the same procedures. The effect is largest for complex operations like IPAA, where a leak rate of 3% at a high-volume center can become 12% at a low-volume one.
Reasonable targets when choosing where to have your operation:
- The surgeon personally performs at least 20 IPAA operations per year (ideally 50+).
- The center has a dedicated IBD surgical program, a WOC nurse, and a GI team that co-manages in-hospital.
- The surgeon is board-certified in colon and rectal surgery.
- They will tell you their own complication rate, leak rate, and conversion rate without hedging. If they won't, keep looking.
Traveling to a center of excellence for a planned operation is not vanity — it is the rational choice when a single decision shapes the next forty years of your life. Major U.S. programs include Cleveland Clinic, Mayo Rochester, Mount Sinai, UCSF, Massachusetts General, and University of Chicago. Academic programs with active IBD research generally do better than community centers at complex pouch work.
Post-Op Diet — First Weeks and Beyond
Every surgical team has its own exact protocol, but the general arc looks like this:
- Days 0–3 in hospital: sips of clear liquids, advanced to full liquids as bowel function returns. Chewing gum and early ambulation genuinely speed return of motility — not folklore, backed by ERAS data.
- Weeks 1–3 at home: low-residue diet — white rice, white bread, bananas, eggs, tender cooked chicken, fish, smooth peanut butter, applesauce. Small frequent meals. Avoid raw vegetables, seeds, nuts, corn, popcorn, and tough skins. This is the riskiest window for a stoma blockage.
- Weeks 4–12: slowly reintroduce higher-fiber foods one at a time, chewing thoroughly. Keep a food diary for the first month — it makes cause-and-effect patterns obvious.
- Long term after ileostomy: hydration (2.5–3 L/day including oral rehydration), salt liberally, electrolyte monitoring during heat or exercise.
- Long term after J-pouch: most patients reach a near-normal diet by month 6. Slowing stool output may require soluble fiber (psyllium), loperamide, or bile-acid sequestrants — all compatible with a pouch.
See the sibling diet for IBD article for longer-term eating strategies once healing is complete.
Key Research Papers
- Ponsioen CY, et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn's disease (LIR!C): a randomised controlled, open-label, multicentre trial. Lancet Gastroenterol Hepatol. 2017.
- Stevens TW, et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn's disease: retrospective long-term follow-up of the LIR!C trial. Lancet Gastroenterol Hepatol. 2020.
- Rutgeerts P, et al. Predictability of the postoperative course of Crohn's disease. Gastroenterology. 1990. (Original Rutgeerts score.)
- Travis S, et al. Vedolizumab for the treatment of chronic pouchitis (EARNEST). N Engl J Med. 2023.
- Fazio VW, et al. Ileal pouch anal anastomosis: analysis of outcome and quality of life in 3707 patients. Ann Surg. 2013.
- Waljee A, et al. Threefold increased risk of infertility: a meta-analysis of infertility after ileal pouch anal anastomosis in ulcerative colitis. Gut. 2006.
Live PubMed Searches
For deeper reading, these PubMed topic searches return current peer-reviewed work on IBD surgical decision-making, reconstruction, and post-operative care:
- LIR!C trial and ileocecal resection in Crohn's
- Stricturoplasty in Crohn's disease
- Perianal Crohn's fistula management
- Rutgeerts score and post-operative recurrence
- Ileal pouch-anal anastomosis outcomes
- Pouchitis and vedolizumab (EARNEST)
- IPAA and female fertility
- Permanent ileostomy and quality of life
- Surgeon volume and colorectal surgery outcomes
- Kock pouch and continent ileostomy
Connections
- Inflammatory Bowel Disease Overview
- Crohn's vs Ulcerative Colitis: Key Differences
- Diagnostic Workup: Calprotectin, Colonoscopy, MRE
- Biologics: TNF, IL-23, and Integrin Inhibitors
- JAK Inhibitors and S1P Modulators
- Diet for IBD: SCD and Mediterranean
- Extraintestinal Manifestations: Joints, Skin, Eyes
- IBD Fatigue, Anemia, and Nutrient Deficiencies
- Pregnancy and IBD
- Crohn's Disease
- Ulcerative Colitis
- Diverticulitis
- Irritable Bowel Syndrome
- Chronic Diarrhea
- AS and IBD Overlap