Adrenal Fatigue (HPA Axis Dysfunction)
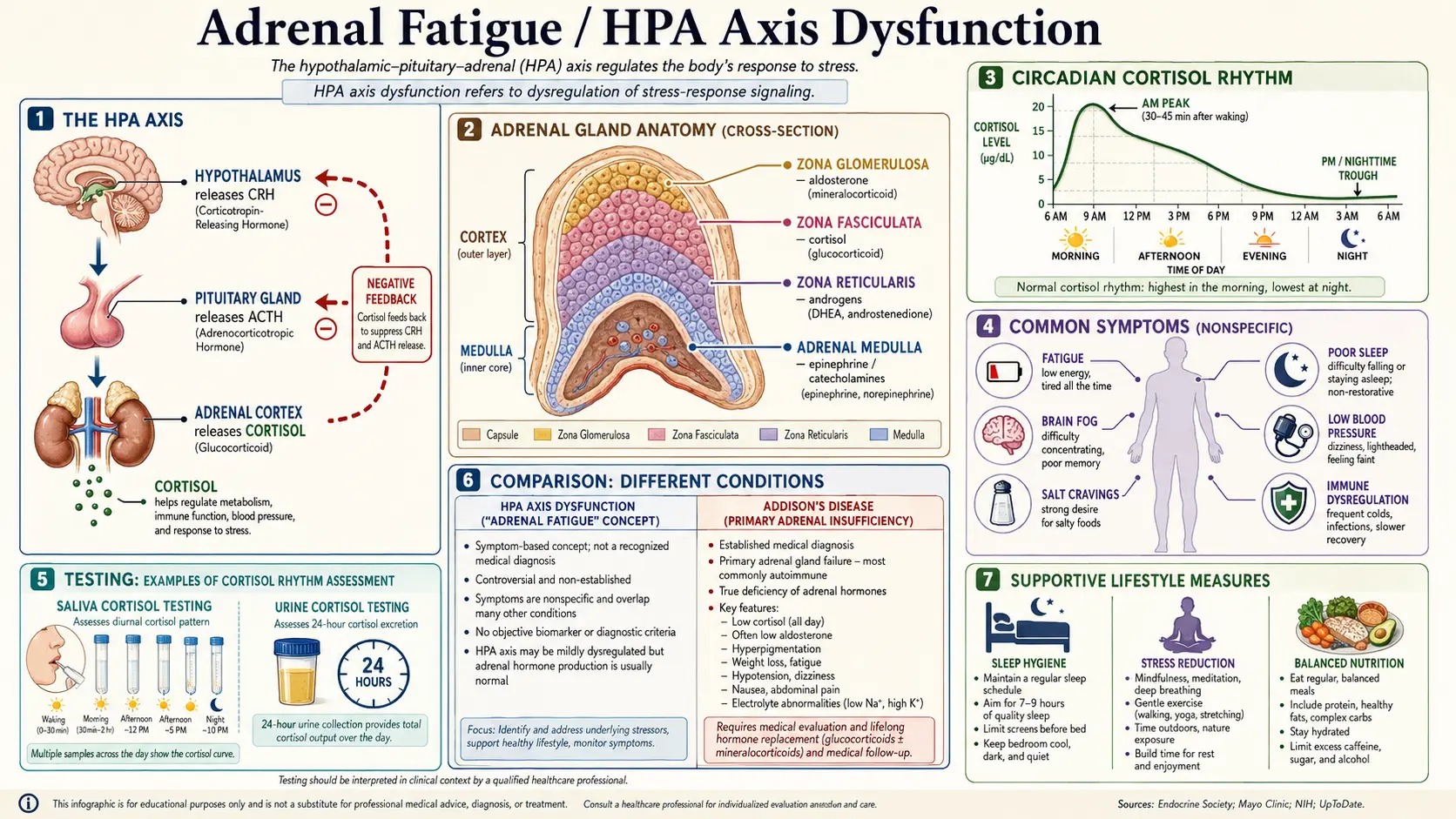
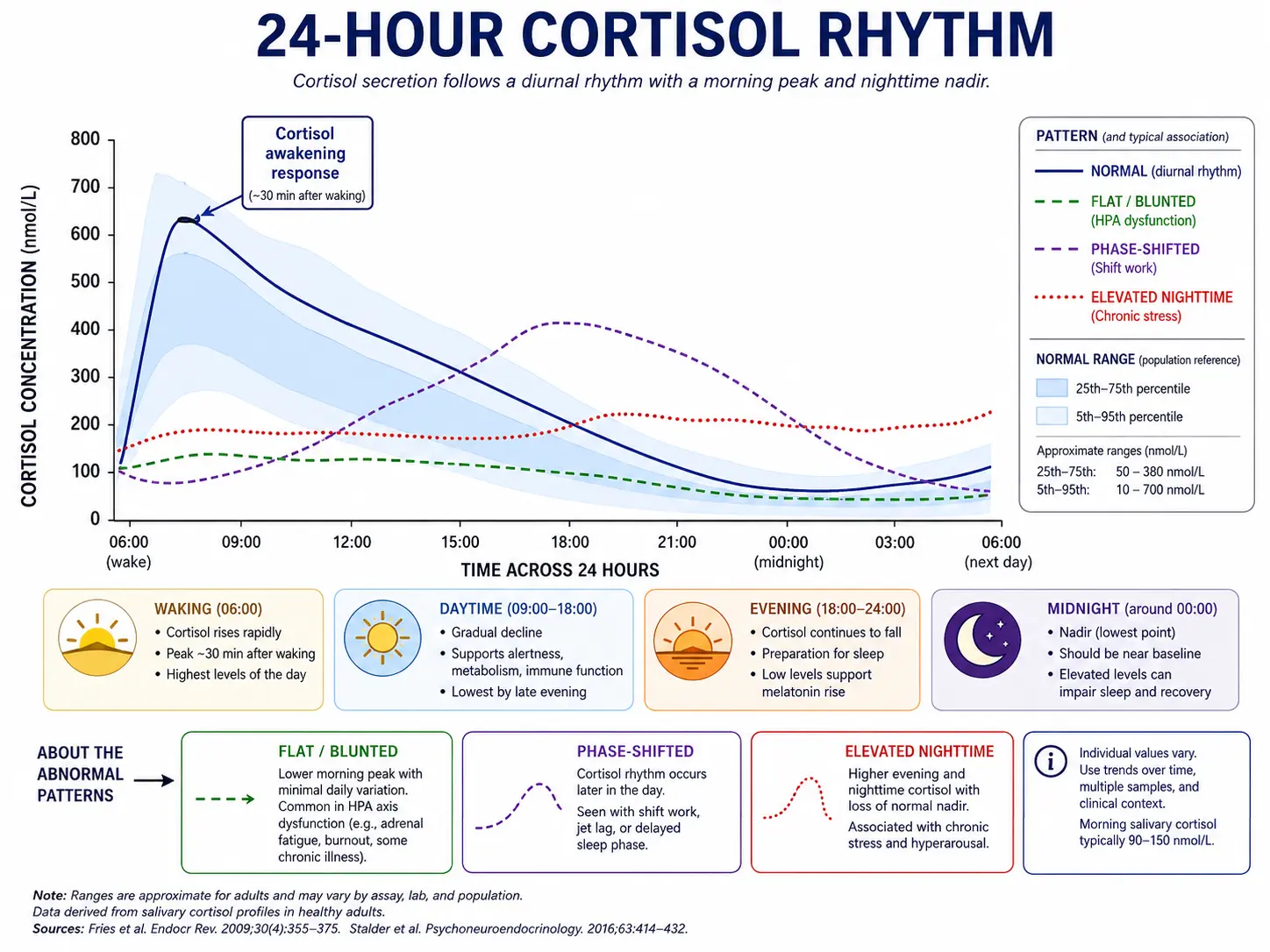
Table of Contents
- What is Adrenal Fatigue?
- The HPA Axis and Cortisol Rhythm
- HPA Axis Dysfunction Patterns
- Symptoms
- Testing
- Differential Diagnosis
- Management and Recovery
- Research Papers
- Connections
- Featured Videos
What is Adrenal Fatigue?
"Adrenal fatigue" is a popular term — coined by chiropractor James Wilson in 1998 — for a constellation of symptoms (chronic tiredness, brain fog, salt cravings, low stress tolerance) that supposedly arise when the adrenal glands become "exhausted" from prolonged stress and stop producing enough cortisol. The term is widely used in functional and integrative medicine but is not recognized as a medical diagnosis by the Endocrine Society, the American Medical Association, or any major endocrinology body. A 2016 systematic review in BMC Endocrine Disorders examined 58 studies and found no consistent evidence that "adrenal fatigue" exists as a discrete physiological entity.
That does not mean the symptoms aren't real. What it means is that the underlying physiology is more accurately described as HPA axis dysfunction — a dysregulation of the hypothalamic-pituitary-adrenal signaling network — rather than the adrenal glands themselves being "tired." Chronic psychological stress, poor sleep, irregular meals, inflammation, and trauma can genuinely shift cortisol output away from its healthy rhythm. The adrenals don't burn out; the brain's signaling to them changes.
It is critical to distinguish this functional dysregulation from Addison's disease (primary adrenal insufficiency), which is a real, life-threatening autoimmune or infectious destruction of the adrenal cortex producing severely low cortisol and aldosterone. Addison's affects roughly 1 in 100,000 people, requires lifelong hydrocortisone replacement, and is diagnosed by a low morning cortisol with a failed ACTH stimulation test. "Adrenal fatigue" as discussed in functional medicine is a different concept, and the two should never be confused or treated interchangeably.
The functional-medicine framing is useful because it gives patients a shared vocabulary for symptoms that conventional medicine often dismisses or relabels as "depression" or "deconditioning." The framing becomes harmful when it short-circuits proper workup — people self-treating presumed adrenal fatigue with hydrocortisone or large pregnenolone doses can suppress their own HPA axis and develop the iatrogenic version of the very condition they were trying to fix. The honest middle ground: take the symptoms seriously, rule out conventional causes thoroughly, then work on HPA axis recovery through sleep, circadian alignment, blood sugar stability, and stress reduction.
The HPA Axis and Cortisol Rhythm
The hypothalamic-pituitary-adrenal (HPA) axis is the body's master stress-response network. When the brain perceives a stressor — psychological, physical, inflammatory, or simply the act of waking up — the hypothalamus releases corticotropin-releasing hormone (CRH). CRH travels a few millimeters down to the anterior pituitary, which releases adrenocorticotropic hormone (ACTH) into the bloodstream. ACTH reaches the adrenal cortex (the outer layer of the small triangular glands sitting on top of the kidneys) and stimulates synthesis of cortisol. Cortisol then feeds back to the hypothalamus and pituitary to dampen further CRH and ACTH release — a classic negative-feedback loop.
Cortisol is not just a stress hormone. It mobilizes glucose, modulates immune function, sets blood pressure tone, regulates inflammation, and — most relevantly here — runs on a sharp diurnal rhythm coordinated with the suprachiasmatic nucleus (the brain's master clock). In a healthy adult:
- Cortisol Awakening Response (CAR): Cortisol rises sharply in the 30–45 minutes after waking, peaking 50–75% above the wake-time value. The CAR is what gets you out of bed, mobilizes blood sugar for the day, and sets cognitive alertness. A robust CAR is one of the strongest markers of a healthy stress system.
- Mid-morning peak: Total cortisol output is highest between 7–9 AM.
- Gradual decline: Cortisol falls steadily through the day, with a small bump after lunch in some people.
- Evening trough: By 6–8 PM, cortisol should be at roughly 10–20% of its morning peak.
- Nadir: Around midnight, cortisol reaches its lowest point. This low cortisol is a permissive signal for melatonin release and deep slow-wave sleep.
The diurnal curve illustrated above shows the healthy pattern alongside the most common dysregulated patterns — flat, phase-shifted, and elevated-nighttime — that emerge with chronic stress, shift work, jet lag, or persistent inflammation. The shape of the curve, not just the average daily total, is what matters for energy, sleep, and recovery.
HPA Axis Dysfunction Patterns
Modern stress research describes HPA dysregulation as a progression rather than a single state. People often move through phases over months or years:
1. Hyperactivation (early stage)
- Elevated cortisol throughout the day, especially evening and night.
- "Wired but tired" feeling: hard to wind down, hard to stay asleep at 3 AM.
- High blood sugar reactivity, central weight gain, anxiety.
- This phase often correlates with the early years of a high-stress job, new caregiving role, or chronic insomnia.
2. Mixed dysregulation
- Normal or slightly elevated total cortisol but a phase-shifted curve — cortisol peaks later in the morning or lingers high into the evening.
- Common in shift workers, parents of young children, and people with severe jet lag.
- Often paired with a blunted CAR — the morning rise is shallow even when total output looks fine.
3. Hypoactivation ("burnout")
- Total cortisol output is low or low-normal, with a flat curve — little difference between morning and evening.
- Profound morning fatigue, inability to feel rested no matter how long you sleep, low motivation, low blood pressure, salt cravings.
- Documented in chronic fatigue syndrome (ME/CFS), fibromyalgia, PTSD, and long-standing burnout.
- This is the pattern most popularly — and inaccurately — called "adrenal fatigue."
4. Reactive hypercortisolism on a hypoactive baseline
- The most clinically confusing pattern: a flat baseline curve with sharp cortisol spikes in response to even mild stressors (a difficult email, traffic, an argument).
- Reflects loss of feedback regulation and an exaggerated central CRH response.
- Patients describe this as "fragile" energy: feeling shaky, post-adrenaline crashes after minor events.
Importantly, the adrenal glands themselves are not damaged in any of these patterns. ACTH stimulation testing in HPA dysregulation is virtually always normal — the adrenals will produce cortisol just fine when directly told to. The problem is upstream, in how the brain orchestrates the signal.
Symptoms
The symptom profile of HPA dysfunction overlaps heavily with depression, hypothyroidism, anemia, and sleep disorders — which is why thorough differential workup matters. Hallmark complaints include:
- Chronic fatigue not relieved by sleep — you sleep 8–10 hours and still wake unrefreshed.
- Morning sluggishness — the first 1–2 hours after waking are particularly rough; coffee feels essential, not optional.
- Mid-afternoon energy crash at 3–4 PM — often coinciding with a normal post-lunch cortisol dip that becomes intolerable when overall HPA function is weak.
- Second wind in the evening — energy paradoxically returns at 9–11 PM, making it hard to fall asleep.
- 3 AM wake-ups — a classic sign of nighttime cortisol spikes; you wake feeling alert and anxious.
- Salt cravings — mediated by aldosterone, which is also adrenal-cortex output and can fall in mineralocorticoid-deficient states.
- Sugar and caffeine cravings — the body chases blood-sugar bumps to compensate for poor cortisol-mediated glucose mobilization.
- Postural lightheadedness — standing up makes you dizzy; this is partly low blood pressure from low aldosterone tone.
- Low libido — chronic stress shifts hormonal precursors toward cortisol and away from DHEA, testosterone, and progesterone.
- Brain fog and impaired short-term memory — cortisol is a major regulator of hippocampal function; both excess and deficiency impair recall.
- Irritability and emotional lability — reduced stress tolerance, easy tears, short fuse with family.
- Cold intolerance and feeling cold all the time — overlaps with hypothyroid symptoms and demands thyroid testing.
- Slow recovery from illness or exercise — a workout that used to take a day to recover from now takes three.
- Hypoglycemia symptoms between meals — shakiness, irritability, headache that resolves with food.
None of these symptoms are specific. Each one needs a real differential. The constellation, especially when combined with a documented stressful life period (new baby, caregiving for a dying parent, job loss, post-viral state), is what raises suspicion for HPA dysregulation.
Testing
Conventional and functional medicine use overlapping but distinct testing approaches. Both have a role.
Conventional first-line tests
- AM serum cortisol (drawn between 7–9 AM): a single morning value below 3 mcg/dL strongly suggests primary or secondary adrenal insufficiency. A value above 15 mcg/dL effectively rules out frank adrenal insufficiency. The middle ground (3–15 mcg/dL) requires further workup.
- ACTH stimulation test (cosyntropin / Synacthen): 250 mcg of synthetic ACTH is injected; cortisol is measured at 30 and 60 minutes. A peak above 18–20 mcg/dL excludes adrenal insufficiency. This is the definitive test for Addison's disease and central (pituitary) adrenal insufficiency.
- Plasma ACTH: high in primary adrenal insufficiency (Addison's), low in secondary/central insufficiency.
- Serum aldosterone and renin: low aldosterone with high renin is characteristic of primary adrenal insufficiency.
- Comprehensive metabolic panel and electrolytes: hyponatremia and hyperkalemia hint at primary adrenal insufficiency.
Functional medicine tests
- Four-point salivary cortisol: samples collected at waking, 30 minutes post-wake, midday, and bedtime. Maps the diurnal curve and reveals patterns that a single morning blood draw cannot.
- DUTCH test (Dried Urine Test for Comprehensive Hormones): extends salivary cortisol with cortisone, cortisol metabolites (5a-THF, 5b-THF), DHEA, and sex hormones from the same 24-hour urine collection. Gives a richer picture of total cortisol production vs. clearance.
- DHEA-S: dehydroepiandrosterone sulfate is the most abundant steroid in circulation and a marker of adrenal cortex output. Low DHEA-S relative to age-adjusted norms supports HPA hypofunction.
- Cortisol-to-DHEA ratio: a high ratio reflects catabolic stress dominance.
Workup to rule out mimics
- Complete blood count and ferritin — iron deficiency anemia mimics fatigue precisely.
- Comprehensive thyroid panel (TSH, free T4, free T3, reverse T3, TPO antibodies) — hypothyroidism and Hashimoto's overlap with HPA symptoms heavily.
- Vitamin B12, folate, vitamin D — deficiencies of any of these produce identical fatigue.
- Fasting glucose, insulin, hemoglobin A1c — reactive hypoglycemia and early insulin resistance both mimic afternoon crashes.
- EBV titers, Lyme panel, sleep study — if symptoms are severe or post-viral, these become essential.
Differential Diagnosis
Before settling on "HPA axis dysfunction," every conventional cause of fatigue must be ruled out. A fatigue presentation without proper workup is the single most common reason patients with treatable disease are mislabeled as having "adrenal fatigue" and lose years to ineffective supplements.
- Iron deficiency anemia — common, especially in menstruating women; ferritin below 30 ng/mL is symptomatic even without overt anemia.
- Hypothyroidism / Hashimoto's thyroiditis — cold intolerance, brain fog, weight gain, hair loss; demands a full thyroid panel, not just TSH.
- Obstructive sleep apnea — the most under-diagnosed cause of "adrenal fatigue" in adults over 35; a home sleep study is cheap and fast.
- Major depressive disorder — anhedonia, low energy, sleep disturbance, weight change; the symptom overlap is near-total and depression itself disrupts the HPA axis.
- Type 2 diabetes / reactive hypoglycemia — afternoon crashes, post-meal sleepiness, hunger between meals.
- Chronic infection (EBV reactivation, Lyme, chronic sinus, dental) — persistent low-grade infection drives inflammation and cortisol dysregulation.
- Autoimmune disease — lupus, rheumatoid arthritis, celiac, and others all produce fatigue often before more specific symptoms emerge.
- Primary adrenal insufficiency (Addison's disease) — rare but missed; characterized by hyperpigmentation, weight loss, hyponatremia, hyperkalemia, and salt craving; demands immediate ACTH stimulation testing.
- Secondary (central) adrenal insufficiency — pituitary or hypothalamic disease; consider after head trauma, pituitary surgery, long opioid use, or chronic glucocorticoid use.
- Cushing's syndrome — ironically the opposite problem (chronic high cortisol from a tumor or exogenous steroid), but presents with fatigue plus weight gain, easy bruising, purple striae, hypertension; rule out with 24-hour urinary free cortisol or late-night salivary cortisol.
- ME/CFS and fibromyalgia — legitimate diagnoses with documented HPA changes; require their own management framework beyond stress reduction.
- Long COVID and post-viral fatigue syndromes — documented HPA hypofunction is well described.
The order of testing should reflect prior probability. In a 40-year-old woman with fatigue, run iron studies and a full thyroid panel before ordering a DUTCH test.
Management and Recovery
Recovery from HPA dysregulation is mostly behavioral and circadian. Supplements and adaptogens have a supporting role; they cannot outpace a fundamentally chaotic schedule, ongoing toxic stress, or untreated sleep apnea. The order matters:
1. Sleep is the foundation
- Consistent wake time, every day including weekends, is more important than total hours. The wake time is the most powerful zeitgeber resetting the HPA axis.
- Morning sunlight within 30 minutes of waking, 5–15 minutes outdoors without sunglasses. This anchors the cortisol awakening response and the evening melatonin rise.
- Dim, warm light after sunset; minimize bright overhead lights and blue-spectrum screens after 9 PM.
- Cool, dark bedroom: 65–68°F (18–20°C); blackout curtains.
- If insomnia is severe, treat it directly (CBT-I, sleep study to rule out apnea) before assuming "adrenal fatigue."
2. Blood sugar stability
- Eat within 60 minutes of waking: protein and fat (eggs, yogurt, nuts) more than carbohydrates. A high-carb breakfast on a depleted system spikes and crashes blood sugar.
- Don't skip meals while in recovery; reactive hypoglycemia is itself an HPA stressor.
- Limit caffeine to before noon, and consider a multi-week caffeine taper if you depend on multiple cups daily — caffeine half-life is 5–7 hours and afternoon coffee directly disrupts cortisol decline and sleep architecture.
- Avoid alcohol as a sleep aid; it fragments deep sleep and elevates 3 AM cortisol.
3. Stress modulation
- Daily mindfulness or meditation: even 10 minutes of slow breathing (4-second in, 6-second out) measurably lowers afternoon cortisol over weeks.
- Yoga, tai chi, restorative practices: lower cortisol while building parasympathetic tone better than high-intensity exercise during recovery.
- Address the root stressor — difficult marriage, untenable job, caregiving without support. Supplements cannot compensate for ongoing adversity.
- Therapy, especially trauma-focused (EMDR, somatic experiencing) when relevant, can normalize HPA reactivity in ways no nutraceutical can.
4. Adaptogenic herbs
"Adaptogens" are plants that buffer stress responses by modulating the HPA axis in both directions — lowering excess cortisol and supporting blunted output. Quality varies enormously by extract; standardized products from reputable brands matter.
- Ashwagandha (Withania somnifera) — the best-studied adaptogen for HPA support. KSM-66 or Sensoril extracts at 300–600 mg/day have shown consistent reductions in serum cortisol, perceived stress, and improvements in sleep across multiple randomized trials. Avoid in pregnancy and in people with active hyperthyroidism.
- Rhodiola rosea — particularly useful for fatigue, mental performance, and burnout. Standardized to 3% rosavins / 1% salidroside, dosed at 200–400 mg/day taken in the morning (it can be activating; not for evening use).
- Holy basil / Tulsi (Ocimum sanctum) — gentler than ashwagandha, useful for anxiety and inflammation; 300–600 mg/day of standardized extract or as a daily tea.
- Eleuthero (Siberian ginseng), Schisandra, Cordyceps — secondary options with some evidence; rotate rather than stack.
5. Nutrient support
- Magnesium glycinate 200–400 mg before bed — supports parasympathetic tone, sleep, and stress reactivity.
- Vitamin C 500–1000 mg/day — the adrenal cortex concentrates ascorbate at 100x serum levels and uses it for cortisol synthesis.
- B-complex with active forms (methylfolate, methyl-B12, P5P) — cofactors for catecholamine and cortisol metabolism.
- Vitamin D3 2000–5000 IU/day to a serum target of 40–60 ng/mL — deficiency is independently associated with fatigue and HPA dysregulation.
- Omega-3 fatty acids 1–2 g EPA+DHA daily — lower inflammatory tone and modulate cortisol reactivity.
6. What to avoid
- Self-prescribed hydrocortisone or pregnenolone — suppresses the HPA axis and can cause iatrogenic adrenal insufficiency. Only use under endocrinology supervision after testing confirms true insufficiency.
- "Adrenal glandular" extracts from animal adrenals — unregulated cortisol content, unpredictable doses, no quality control.
- Stimulants stacked on stimulants — coffee plus pre-workout plus more coffee. The cycle of "needing more" to function is itself a sign of HPA dysregulation.
- Heroic exercise — high-intensity training during a hypofunctional phase delays recovery. Walking, gentle resistance, and yoga first; rebuild intensity as the curve normalizes.
Recovery timelines vary. Mild HPA dysregulation often resolves in 6–12 weeks with consistent sleep, sunlight, and blood sugar work. Severe cases — especially post-burnout or post-viral — can take 12–24 months and demand patience. Repeating four-point salivary cortisol every 3–6 months helps track real progress beyond how you feel on any given day.
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to this condition. Each link opens a live PubMed query.
- HPA axis dysfunction chronic stress
- Cortisol awakening response
- Adrenal fatigue evidence-based review
- Salivary cortisol diurnal
- Ashwagandha cortisol stress
- Rhodiola fatigue
- Holy basil ocimum sanctum cortisol
- Chronic fatigue syndrome HPA
- Burnout cortisol
- Allostatic load
- Primary adrenal insufficiency Addison's
- DHEA supplementation HPA
Connections
- Ashwagandha
- Insulin Resistance
- Addison's Disease
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Diabetes
- Depression
- Anxiety
- Insomnia
- Fatigue
- Brain Fog
- Vitamin B12
- Vitamin D3
- Magnesium
- Cortisol Test
- DHEA-S Test
- Sleep Hygiene
- Burnout